virus
3D Animation Captures Viral Infection in Action
Posted on by Lawrence Tabak, D.D.S., Ph.D.
With the summer holiday season now in full swing, the blog will also swing into its annual August series. For most of the month, I will share with you just a small sampling of the colorful videos and snapshots of life captured in a select few of the hundreds of NIH-supported research labs around the country.
To get us started, let’s turn to the study of viruses. Researchers now can generate vast amounts of data relatively quickly on a virus of interest. But data are often displayed as numbers or two-dimensional digital images on a computer screen. For most virologists, it’s extremely helpful to see a virus and its data streaming in three dimensions. To do so, they turn to a technological tool that we all know so well: animation.
This research animation features the chikungunya virus, a sometimes debilitating, mosquito-borne pathogen transmitted mainly in developing countries in Africa, Asia and the Americas. The animation illustrates large amounts of research data to show how the chikungunya virus infects our cells and uses its specialized machinery to release its genetic material into the cell and seed future infections. Let’s take a look.
In the opening seconds, you see how receptor binding glycoproteins (light blue), which are proteins with a carbohydrate attached on the viral surface, dock with protein receptors (yellow) on a host cell. At five seconds, the virus is drawn inside the cell. The change in the color of the chikungunya particle shows that it’s coated in a vesicle, which helps the virus make its way unhindered through the cytoplasm.
At 10 seconds, the virus then enters an endosome, ubiquitous bubble-like compartments that transport material from outside the cell into the cytosol, the fluid part of the cytoplasm. Once inside the endosome, the acidic environment makes other glycoproteins (red, blue, yellow) on the viral surface change shape and become more flexible and dynamic. These glycoproteins serve as machinery that enables them to reach out and grab onto the surrounding endosome membrane, which ultimately will be fused with the virus’s own membrane.
As more of those fusion glycoproteins grab on, fold back on themselves, and form into hairpin-like shapes, they pull the membranes together. The animation illustrates not only the changes in protein organization, but the resulting effects on the integrity of the membrane structures as this dynamic process proceeds. At 53 seconds, the viral protein shell, or capsid (green), which contains the virus’ genetic instructions, is released back out into the cell where it will ultimately go on to make more virus.
This remarkable animation comes from Margot Riggi and Janet Iwasa, experts in visualizing biology at the University of Utah’s Animation Lab, Salt Lake City. Their data source was researcher Kelly Lee, University of Washington, Seattle, who collaborated closely with Riggi and Iwasa on this project. The final product was considered so outstanding that it took the top prize for short videos in the 2022 BioArt Awards competition, sponsored by the Federation of American Societies for Experimental Biology (FASEB).
The Lee lab uses various research methods to understand the specific shape-shifting changes that chikungunya and other viruses perform as they invade and infect cells. One of the lab’s key visual tools is cryo-electron microscopy (Cryo-EM), specifically cryo-electron tomography (cryo-ET). Cryto-ET enables complex 3D structures, including the intermediate state of biological reactions, to be captured and imaged in remarkably fine detail.
In a study in the journal Nature Communications [1] last year, Lee’s team used cryo-ET to reveal how the chikungunya virus invades and delivers its genetic cargo into human cells to initiate a new infection. While Lee’s cryo-ET data revealed stages of the virus entry process and fine structural details of changes to the virus as it enters a cell and starts an infection, it still represented a series of snapshots with missing steps in between. So, Lee’s lab teamed up with The Animation Lab to help beautifully fill in the gaps.
Visualizing chikungunya and similar viruses in action not only makes for informative animations, it helps researchers discover better potential targets to intervene in this process. This basic research continues to make progress, and so do ongoing efforts to develop a chikungunya vaccine [2] and specific treatments that would help give millions of people relief from the aches, pains, and rashes associated with this still-untreatable infection.
References:
[1] Visualization of conformational changes and membrane remodeling leading to genome delivery by viral class-II fusion machinery. Mangala Prasad V, Blijleven JS, Smit JM, Lee KK. Nat Commun. 2022 Aug 15;13(1):4772. doi: 10.1038/s41467-022-32431-9. PMID: 35970990; PMCID: PMC9378758.
[2] Experimental chikungunya vaccine is safe and well-tolerated in early trial, National Institute of Allergy and Infectious Diseases news release, April 27, 2020.
Links:
Chikungunya Virus (Centers for Disease Control and Prevention, Atlanta)
Global Arbovirus Initiative (World Health Organization, Geneva, Switzerland)
The Animation Lab (University of Utah, Salt Lake City)
Video: Janet Iwasa (TED Speaker)
Lee Lab (University of Washington, Seattle)
BioArt Awards (Federation of American Societies for Experimental Biology, Rockville, MD)
NIH Support: National Institute of General Medical Sciences; National Institute of Allergy and Infectious Diseases
Study Reveals How Epstein-Barr Virus May Lead to Cancer
Posted on by Lawrence Tabak, D.D.S., Ph.D.
Chances are good that you’ve had an Epstein-Barr virus (EBV) infection, usually during childhood. More than 90 percent of us have, though we often don’t know it. That’s because most EBV infections are mild or produce no symptoms at all.
But in some people, EBV can lead to other health problems. The virus can cause infectious mononucleosis (“mono”), type 1 diabetes, and other ailments. It also can persist in our bodies for years and cause increased risk later in life for certain cancers, such as lymphoma, leukemia, and head and neck cancer. Now, an NIH-funded team has some of the best evidence yet to explain how this EBV that hangs around may lead to cancer [1].
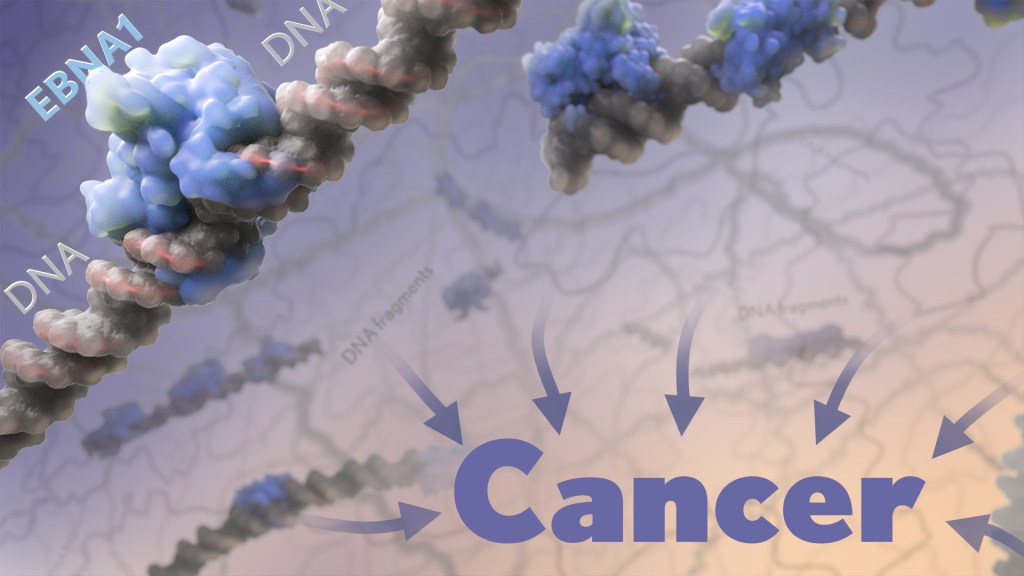
The paper, published recently in the journal Nature, shows that a key viral protein readily binds to a particular spot on a particular human chromosome. Where the protein accumulates, the chromosome becomes more prone to breaking for reasons that aren’t yet fully known. What the study makes clearer is that the breakage produces latently infected cells that are more likely over time to become cancerous.
This discovery paves the way potentially for ways to screen for and identify those at particular risk for developing EBV-associated cancers. It may also fuel the development of promising new ways to prevent these cancers from arising in the first place.
The work comes from a team led by Don Cleveland and Julia Su Zhou Li, University of California San Diego’s Ludwig Cancer Research, La Jolla, CA. Over the years, it’s been established that EBV, a type of herpes virus, often is detected in certain cancers, particularly in people with a long-term latent infection. What interested the team is a viral protein, called EBNA1, which routinely turns up in those same EBV-related cancers.
The EBNA1 protein is especially interesting because it binds viral DNA in particular spots, which allows the virus to persist and make more copies of itself. This discovery raised the intriguing possibility that the protein may also bind similar sequences in human DNA. While it had been suggested previously that this interaction might play a role in EBV-associated cancers, the details had remained murky—until now.
In the new study, the researchers first made uninfected human cells produce the viral EBNA1 protein. They then peered inside them with a microscope to see where those proteins went. In both healthy and cancerous human cells, they watched as EBNA1 proteins built up at two distinct spots and confirmed that this accumulation was dependent on the protein’s ability to bind DNA.
Next, they mapped where exactly EBNA1 binds to human DNA. Interestingly, it was along a repetitive non-protein-coding stretch of DNA on human chromosome 11. This region includes more than 300 copies of an 18-letter sequence that looks quite similar to the EBNA1-binding sites in its own viral genome.
What’s more, the researchers noticed that the repetitive DNA there takes on a structure that’s known for being unstable. And these so-called fragile sites are inherently prone to breaking.
The team went on to uncover evidence that the buildup of EBNA1 at this already fragile site only makes matters worse. In EBV-infected cells, increasing the amount of EBNA1 protein led to more chromosome 11 breaks. Those breaks showed up within a single day in about 40 percent of cells.
For these cells, those breaks also may be a double whammy. That’s because the breaks are located next to neighboring genes with long recognized roles in regulating cell growth. When altered, these genes can contribute to turning a cell cancerous.
To further nail down the link to cancer, the researchers looked to whole-genome sequencing data for more than 2,400 cancers including 38 tumor types from the international Pan-Cancer Analysis of Whole Genomes consortium [2]. They found that tumors with detectable EBV also had an unusually high number of chromosome 11 abnormalities. In fact, that was true in every single case of head and neck cancer.
The findings suggest that people will vary in their susceptibility to EBNA1-induced DNA breaks along chromosome 11 based on the amount of EBNA1 protein in their latently infected cells. It also will depend on the number of EBV-like DNA repeats present in their DNA.
Given these new findings, it’s worth noting that the presence of EBV and the very same viral protein has been implicated also in the link between EBV and multiple sclerosis (MS) [3]. Together, these recent findings are a reminder of the value in pursuing an EBV vaccine that might thwart this infection and its associated conditions, including certain cancers and MS. And, we’re getting there. In fact, an early-stage clinical trial for an experimental EBV vaccine is now ongoing here at the NIH Clinical Center.
References:
[1] Chromosomal fragile site breakage by EBV-encoded EBNA1 at clustered repeats. Li JSZ, Abbasi A, Kim DH, Lippman SM, Alexandrov LB, Cleveland DW. Nature. 2023 Apr 12.
[2] Pan-cancer analysis of whole genomes. ICGC/TCGA Pan-Cancer Analysis of Whole Genomes Consortium. Nature.2020 Feb;578(7793):82-93.
[3] Clonally expanded B cells in multiple sclerosis bind EBV EBNA1 and GlialCAM. Lanz TV, Brewer RC, Steinman L, Robinson WH, et al. Nature. 2022 Mar;603(7900):321-327.
Links:
About Epstein-Barr Virus (Centers for Disease Control and Prevention, Atlanta)
Head and Neck Cancer (National Cancer Institute,/NIH)
Multiple Sclerosis (National Institute of Neurological Disorders and Stroke/NIH)
Don W. Cleveland Lab (University of California San Diego, La Jolla, CA)
NIH Support: National Institute of General Medical Sciences; National Institute of Environmental Health Sciences; National Cancer Institute
A Look Back at Science’s 2022 Breakthroughs
Posted on by Lawrence Tabak, D.D.S., Ph.D.
Happy New Year! I hope everyone finished 2022 with plenty to celebrate, whether it was completing a degree or certification, earning a promotion, attaining a physical fitness goal, or publishing a hard-fought scientific discovery.
If the latter, you are in good company. Last year produced some dazzling discoveries, and the news and editorial staff at the journal Science kept a watchful eye on the most high-impact advances of 2022. In December, the journal released its list of the top 10 advances across the sciences, from astronomy to zoology. In case you missed it, Science selected NASA’s James Webb Space Telescope (JWST) as the 2022 Breakthrough of the Year [1].
This unique space telescope took 20 years to complete, but it has turned out to be time well spent. Positioned 1.5-million-kilometers from Earth, the JWST and its unprecedented high-resolution images of space have unveiled the universe anew for astronomers and wowed millions across the globe checking in online. The telescope’s image stream, beyond its sheer beauty, will advance study of the early Universe, allowing astronomers to discover distant galaxies, explore the early formation of stars, and investigate the possibility of life on other planets.
While the biomedical sciences didn’t take home the top prize, they were well represented among Science’s runner-up breakthroughs. Some of these biomedical top contenders also have benefited, directly or indirectly, from NIH efforts and support. Let’s take a look:
RSV vaccines nearing the finish line: It’s been one of those challenging research marathons. But scientists last year started down the homestretch with the first safe-and-effective vaccine for respiratory syncytial virus (RSV), a leading cause of severe respiratory illness in the very young and the old.
In August, the company Pfizer presented evidence that its experimental RSV vaccine candidate offered protection for those age 60 and up. Later, they showed that the same vaccine, when administered to pregnant women, helped to protect their infants against RSV for six months after birth. Meanwhile, in October, the company GSK announced encouraging results from its late-stage phase III trial of an RSV vaccine in older adults.
As Science noted, the latest clinical progress also shows the power of basic science. For example, researchers have been working with chemically inactivated versions of the virus to develop the vaccine. But these versions have a key viral surface protein that changes its shape after fusing with a cell to start an infection. In this configuration, the protein elicits only weak levels of needed protective antibodies.
Back in 2013, Barney Graham, then with NIH’s National Institute of Allergy and Infectious Diseases (NIAID), and colleagues, solved the problem [2]. Graham’s NIH team discovered a way to lock the protein into its original prefusion state, which the immune system can better detect. This triggers higher levels of potent antibodies, and the discovery kept the science—and the marathon—moving forward.
These latest clinical advances come as RSV and other respiratory viruses, including SARS-CoV-2, the cause of COVID-19, are sending an alarming number of young children to the hospital. The hope is that researchers will cross the finish line this year or next, and we’ll have the first approved RSV vaccine.
Virus fingered as cause of multiple sclerosis: Researchers have long thought that multiple sclerosis, or MS, has a viral cause. Pointing to the right virus with the required high degree of certainty has been the challenge, slowing progress on the treatment front for those in need. As published in Science last January, Alberto Ascherio, Harvard T.H. Chan School of Public Health, Boston, and colleagues produced the strongest evidence yet that MS is caused by the Epstein-Barr virus (EBV), a herpesvirus also known for causing infectious mononucleosis [3].
The link between EBV and MS had long been suspected. But it was difficult to confirm because EBV infections are so widespread, and MS is so disproportionately rare. In the recent study, the NIH-supported researchers collected blood samples every other year from more than 10 million young adults in the U.S. military, including nearly 1,000 who were diagnosed with MS during their service. The evidence showed that the risk of an MS diagnosis increased 32-fold after EBV infection, but it held steady following infection with any other virus. Levels in blood serum of a biomarker for MS neurodegeneration also went up only after an EBV infection, suggesting that the viral illness is a leading cause for MS.
Further evidence came last year from a discovery published in the journal Nature by William Robinson, Stanford University School of Medicine, Stanford, CA, and colleagues. The NIH-supported team found a close resemblance between an EBV protein and one made in the healthy brain and spinal cord [4]. The findings suggest an EBV infection may produce antibodies that mistakenly attack the protective sheath surrounding our nerve cells. Indeed, the study showed that up to one in four people with MS had antibodies that bind both proteins.
This groundbreaking research suggests that an EBV vaccine and/or antiviral drugs that thwart this infection might ultimately prevent or perhaps even cure MS. Of note, NIAID launched last May an early-stage clinical trial for an experimental EBV vaccine at the NIH Clinical Center, Bethesda, MD.
AI Gets Creative: Science’s 2021 Breakthrough of the Year was AI-powered predictions of protein structure. In 2022, AI returned to take another well-deserved bow. This time, Science singled out AI’s now rapidly accelerating entry into once uniquely human attributes, such as artistic expression and scientific discovery.
On the scientific discovery side, Science singled out AI’s continued progress in getting creative with the design of novel proteins for vaccines and myriad other uses. One technique, called “hallucination,” generates new proteins from scratch. Researchers input random amino acid sequences into the computer, and it randomly and continuously mutates them into sequences that other AI tools are confident will fold into stable proteins. This greatly simplifies the process of protein design and frees researchers to focus their efforts on creating a protein with a desired function.
AI research now engages scientists around world, including hundreds of NIH grantees. Taking a broader view of AI, NIH recently launched the Artificial Intelligence/Machine Learning Consortium to Advance Health Equity and Researcher Diversity (AIM-AHEAD) Program. It will help to create greater diversity within the field, which is a must. A lack of diversity could perpetuate harmful biases in how AI is used, how algorithms are developed and trained, and how findings are interpreted to avoid health disparities and inequities for underrepresented communities.
And there you have it, some of the 2022 breakthroughs from Science‘s news and editorial staff. Of course, the highlighted biomedical breakthroughs don’t capture the full picture of research progress. There were many other milestone papers published in 2022 that researchers worldwide will build upon in the months and years ahead to make further progress in their disciplines and, for some, draw the attention of Science’s news and editorial staff. Here’s to another productive year in biomedical research, which the blog will continue to feature and share with you as it unfolds in 2023.
References:
[1] 2022 Breakthrough of the Year. Science. Dec 15, 2022.
[2] Structure of RSV fusion glycoprotein trimer bound to a prefusion-specific neutralizing antibody. McLellan JS, Chen M, Leung S, Kwong PD, Graham BS, et al. Science. 2013 May 31;340(6136):1113-1117.
[3] Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. Bjornevik K, Cortese M, Healy BC, Kuhle J, Mina MJ, Leng Y, Elledge SJ, Niebuhr DW, Scher AI, Munger KL, Ascherio A. Science. 2022 Jan 21;375(6578):296-301.
[4] Clonally expanded B cells in multiple sclerosis bind EBV EBNA1 and GlialCAM. Lanz TV, Brewer RC, Steinman L, Robinson WH, et al. Nature. 2022 Mar;603(7900):321-327.
Links:
Respiratory Syncytial Virus (RSV) (National Institute of Allergy and Infectious Diseases/NIH)
Multiple Sclerosis (National Institute of Neurological Disorders and Stroke/NIH)
Barney Graham (Morehouse School of Medicine, Atlanta)
Alberto Ascherio (Harvard T.H. Chan School of Public Health, Boston)
Robinson Lab (Stanford Medicine, Stanford, CA)
James Webb Space Telescope (Goddard Space Flight Center/NASA, Greenbelt, MD)
Finding New Ways to Fight Coronavirus … From Studying Bats
Posted on by Dr. Francis Collins

David Veesler has spent nearly 20 years imaging in near-atomic detail the parts of various viruses, including coronaviruses, that enable them to infect Homo sapiens. In fact, his lab at the University of Washington, Seattle, was the first to elucidate the 3D architecture of the now infamous spike protein, which coronaviruses use to gain entry into human cells [1]. He uses these fundamental insights to guide the design of vaccines and therapeutics, including promising monoclonal antibodies.
Now, Veesler and his lab are turning to another mammal in their search for new leads for the next generation of antiviral treatments, including ones aimed at the coronavirus that causes COVID-19, SARS-CoV-2. With support from a 2020 NIH Director’s Pioneer Award, Veesler will study members of the order Chiroptera. Or, more colloquially, bats.
Why bats? Veesler says bats are remarkable creatures. They are the only mammals capable of sustained flight. They rarely get cancer and live unusually long lives for such small creatures. More importantly for Veesler’s research, bats host a wide range of viruses—more than any other mammal species. Despite carrying all of these viruses, bats rarely show symptoms of being sick. Yet they are the source for many of the viruses that have spilled over into humans with devastating effect, including rabies, Ebola virus, Nipah and Hendra viruses, severe acute respiratory syndrome coronavirus (SARS-CoV), and, likely, SARS-CoV-2.
Beyond what is already known about bats’ intriguing qualities, Veesler says humans still have much to discover about these flying mammals, including how their immune systems cope with such an onslaught of viral invaders. For example, it turns out that a bat’s learned, or adaptive, immune system is, for the most part, uncharted territory. As such, it offers an untapped source of potentially promising viral inhibitors just waiting to be unearthed, fully characterized, and then used to guide the development of new kinds of anti-viral therapeutics.
In his studies, Veesler will work with collaborators studying bats around the world to characterize their antibody production. He wants to learn how these antibodies contribute to bats’ impressive ability to tolerate viruses and other pathogens. What is it about the structure of bat antibodies that make them different from human antibodies? And, how can those structural differences serve as blueprints for promising new treatments to combat many potentially deadly viruses?
Interestingly, Veesler’s original grant proposal makes no mention of SARS-CoV-2 or COVID-19. That’s because he submitted it just months before the first reports of the novel coronavirus in Wuhan, China. But Veesler doesn’t consider himself a visionary by expanding his research to bats. He and others had been working on closely related coronaviruses for years, inspired by earlier outbreaks, including SARS in 2002 and Middle East respiratory syndrome (MERS) in 2012 (although MERS apparently came from camels). The researcher didn’t see SARS-CoV-2 coming, but he recognized the potential for some kind of novel coronavirus outbreak in the future.
These days, the Veesler lab has been hard at work to understand SARS-CoV-2 and the human immune response to the virus. His team showed that SARS-CoV-2 uses the human receptor ACE2 to gain entry into our cells [2]. He’s also a member of the international research team that identified a human antibody, called S309, from a person who’d been infected with SARS in 2003. This antibody is showing promise for treating COVID-19 [3], now in a phase 3 clinical trial in the United States.
In another recent study, reported as a pre-print in bioRxiv, Veesler’s team mapped dozens of distinct human antibodies capable of neutralizing SARS-CoV-2 by their ability to hit viral targets outside of the well-known spike protein [4]. Such discoveries may form the basis for new and promising combinations of antibodies to treat COVID-19 that won’t be disabled by concerning new variations in the SARS-CoV-2 spike protein. Perhaps, in the future, such therapeutic cocktails may include modified bat-inspired antibodies too.
References:
[1] Cryo-electron microscopy structure of a coronavirus spike glycoprotein trimer. Walls AC, Tortorici MA, Bosch BJ, Frenz B, Rottier PJM, DiMaio F, Rey FA, Veesler D. Nature. 2016 Mar 3;531(7592):114-117.
[2] Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Cell. 2020 Apr 16;181(2):281-292.e6.
[3] Cross-neutralization of SARS-CoV-2 by a human monoclonal SARS-CoV antibody. Pinto D, Park YJ, Beltramello M, Veesler D, Cortil D, et al. Nature.18 May 2020 [Epub ahead of print]
[4] N-terminal domain antigenic mapping reveals a site of vulnerability for SARS-CoV-2. McCallum M, Marco A, Lempp F, Tortorici MA, Pinto D, Walls AC, Whelan SPJ, Virgin HW, Corti D, Pizzuto MS, Veesler D, et al. bioRxiv. 2021 Jan 14.
Links:
COVID-19 Research (NIH)
Veesler Lab (University of Washington, Seattle)
Veesler Project Information (NIH RePORTER)
NIH Director’s Pioneer Award Program (Common Fund)
NIH Support: Common Fund; National Institute of Allergy and Infectious Diseases
Capturing Viral Shedding in Action
Posted on by Dr. Francis Collins

You’ve probably seen some amazing high-resolution images of SARS-CoV-2, the novel coronavirus that causes COVID-19, on television and the web. What you might not know is that many of these images, including the ones shown here, were produced at Rocky Mountain Laboratories (RML), a part of NIH’s National Institute of Allergy and Infectious Diseases (NIAID) that’s located in the small Montana town of Hamilton.
The head of RML’s Electron Microscopy Unit, Elizabeth Fischer, was the researcher who took this portrait of SARS-CoV-2. For more than 25 years, Fischer has snapped stunning images of dangerous viruses and microbes, including some remarkable shots of the deadly Ebola virus. She also took some of the first pictures of the coronavirus that causes Middle East respiratory syndrome (MERS), which arose from camels and continues to circulate at low levels in people.
The NIAID facility uses a variety of microscopy techniques, including state-of-the-art cryo-electron microscopy (cryo-EM). But the eye-catching image you see here was taken with a classic scanning electron microscope (SEM).
SEM enables visualization of particles, including viruses, that are too small to be seen with traditional light microscopy. It does so by focusing electrons, instead of light, into a beam that scans the surface of a sample that’s first been dehydrated, chemically preserved, and then coated with a thin layer of metal. As electrons bounce off the sample’s surface, microscopists such as Fischer are able to capture its precise topology. The result is a gray-scale micrograph like the one you see above on the left. To make the image easier to interpret, Fischer hands the originals off to RML’s Visual Medical Arts Department, which uses colorization to make key features pop like they do in the image on the right.
So, what exactly are you seeing in this image? The orange-brown folds and protrusions are part of the surface of a single cell that’s been infected with SARS-CoV-2. This particular cell comes from a commonly studied primate kidney epithelial cell line. The small, blue spheres emerging from the cell surface are SARS-CoV-2 particles.
This picture is quite literally a snapshot of viral shedding, a process in which viral particles are released from a dying cell. This image gives us a window into how devastatingly effective SARS-CoV-2 appears to be at co-opting a host’s cellular machinery: just one infected cell is capable of releasing thousands of new virus particles that can, in turn, be transmitted to others.
While capturing a fixed sample on the microscope is fairly straightforward for a pro like Fischer, developing a sample like this one involves plenty of behind-the-scenes trial and error by NIAID investigators. As you might imagine, to see the moment that viruses emerge from an infected cell, you have to get the timing just right.
By capturing many shots of the coronavirus using the arsenal of microscopes available at RML and elsewhere, researchers are learning more every day about how SARS-CoV-2 enters a cell, moves inside it, and then emerges to infect other cells. In addition to advancing scientific knowledge, Fischer notes that images like these also hold the remarkable power to make an invisible enemy visible to the world at large.
Making SARS-CoV-2 tangible helps to demystify the challenges that all of us now face as a result of the COVID-19 pandemic. The hope is it will encourage each and every one of us to do our part to fight it, whether that means digging into the research, working on the front lines, or staying at home to prevent transmission and flatten the curve. And, if you could use some additional inspiration, don’t miss the NIAID’s image gallery on Flickr, which includes some of Fischer’s finest work.
Links:
Coronavirus (COVID-19) (NIH)
Rocky Mountain Laboratories (National Institute of Allergy and Infectious Diseases/NIH)
Elizabeth Fischer (National Institute of Allergy and Infectious Diseases/NIH)
NIH Support: National Institute of Allergy and Infectious Diseases
Bringing Needed Structure to COVID-19 Drug Development
Posted on by Dr. Francis Collins
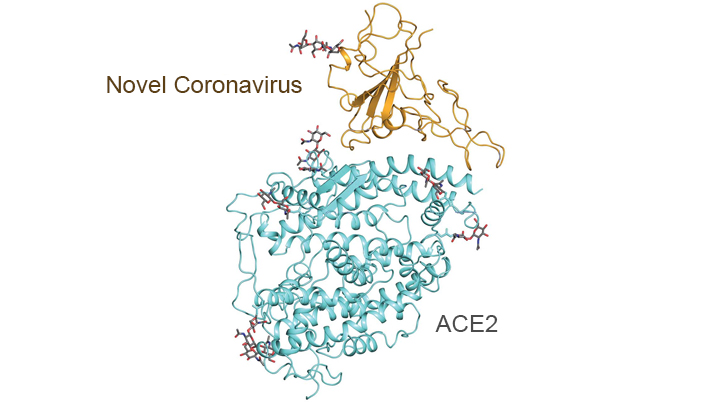
With so much information swirling around these days about the coronavirus disease 2019 (COVID-19) pandemic, it would be easy to miss one of the most interesting and significant basic science reports of the past few weeks. It’s a paper published in the journal Science [1] that presents an atomic-scale snapshot showing the 3D structure of the spike protein on the novel coronavirus attached to a human cell surface protein called ACE2, or angiotensin converting enzyme 2. ACE2 is the receptor that the virus uses to gain entry.
What makes this image such a big deal is that it shows—in exquisite detail—how the coronavirus attaches to human cells before infecting them and making people sick. The structural map of this interaction will help guide drug developers, atom by atom, in devising safe and effective ways to treat COVID-19.
This new work, conducted by a team led by Qiang Zhou, Westlake Institute for Advanced Study, Hangzhou, China, took advantage of a high-resolution imaging tool called cryo-electron microscopy (cryo-EM). This approach involves flash-freezing molecules in liquid nitrogen and bombarding them with electrons to capture their images with a special camera. When all goes well, cryo-EM can solve the structure of intricate macromolecular complexes in a matter of days, including this one showing the interaction between a viral protein and human protein.
Zhou’s team began by mapping the structure of human ACE2 in a complex with B0AT1, which is a membrane protein that it helps to fold. In the context of this complex, ACE2 is a dimer—a scientific term for a compound composed of two very similar units. Additional mapping revealed how the surface protein of the novel coronavirus interacts with ACE2, indicating how the virus’s two trimeric (3-unit) spike proteins might bind to an ACE2 dimer. After confirmation by further research, these maps may well provide a basis for the design and development of therapeutics that specifically target this critical interaction.
The ACE2 protein resides on the surface of cells in many parts of the human body, including the heart and lungs. The protein is known to play a prominent role in the body’s complex system of regulating blood pressure. In fact, a class of drugs that inhibit ACE and related proteins are frequently prescribed to help control high blood pressure, or hypertension. These ACE inhibitors lower blood pressure by causing blood vessels to relax.
Since the COVID-19 outbreak, many people have wondered whether taking ACE inhibitors would be helpful or detrimental against coronavirus infection. This is of particular concern to doctors whose patients are already taking the medications to control hypertension. Indeed, data from China and elsewhere indicate hypertension is one of several coexisting conditions that have consistently been reported to be more common among people with COVID-19 who develop life-threatening severe acute respiratory syndrome.
In a new report in this week’s New England Journal of Medicine, a team of U.K. and U.S. researchers, partly supported by NIH, examined the use of ACE inhibitors and other angiotensin-receptor blockers (ARBs) in people with COVID-19. The team, led by Scott D. Solomon of Brigham and Women’s Hospital and Harvard Medical School, Boston, found that current evidence in humans is insufficient to support or refute claims that ACE inhibitors or ARBs may be helpful or harmful to individuals with COVID-19.
The researchers concluded that these anti-hypertensive drugs should be continued in people who have or at-risk for COVID-19, stating: “Although additional data may further inform the treatment of high-risk patients … clinicians need to be cognizant of the unintended consequences of prematurely discontinuing proven therapies in response to hypothetical concerns.” [2]
Research is underway to generate needed data on the use of ACE inhibitors and similar drugs in the context of the COVID-19 pandemic, as well as to understand more about the basic mechanisms underlying this rapidly spreading viral disease. This kind of fundamental research isn’t necessarily the stuff that will make headlines, but it likely will prove vital to guiding the design of effective drugs that can help bring this serious global health crisis under control.
References:
[1] Structural basis for the recognition of the SARS-CoV-2 by full-length human ACE2. Yan R, Zhang Y, Li Y, Xia L, Guo Y, Zhou Q. Science. 27 March 2020. [Epub ahead of publication]
[2] Renin–Angiotensin–Aldosterone System Inhibitors in Patients with Covid-19. Vaduganathan M, Vardeny O, Michel T, McMurray J, Pfeffer MA, Solomon SD. 30 NEJM. March 2020 [Epub ahead of Publication]
Links:
Coronavirus (COVID-19) (NIH)
COVID-19, MERS & SARS (National Institute of Allergy and Infectious Diseases/NIH)
Transformative High Resolution Cryo-Electron Microscopy (Common Fund/NIH)
Qiang Zhou (Westlake Institute for Advanced Study, Zhejiang Province)
Scott D. Solomon (Brigham and Women’s Hospital, Boston)
NIH Support: National Center for Advancing Translational Sciences; National Heart, Lung, and Blood Institute
To Beat COVID-19, Social Distancing is a Must
Posted on by Dr. Francis Collins

Even in less challenging times, many of us try to avoid close contact with someone who is sneezing, coughing, or running a fever to avoid getting sick ourselves. Our attention to such issues has now been dramatically heightened by the emergence of a novel coronavirus causing a pandemic of an illness known as COVID-19.
Many have wondered if we couldn’t simply protect ourselves by avoiding people with symptoms of respiratory illness. Unfortunately, the answer is no. A new study shows that simply avoiding symptomatic people will not go far enough to curb the COVID-19 pandemic. That’s because researchers have discovered that many individuals can carry the novel coronavirus without showing any of the typical symptoms of COVID-19: fever, dry cough, and shortness of breath. But these asymptomatic or only mildly ill individuals can still shed virus and infect others.
This conclusion adds further weight to the recent guidance from U.S. public health experts: what we need most right now to slow the stealthy spread of this new coronavirus is a full implementation of social distancing. What exactly does social distancing mean? Well, for starters, it is recommended that people stay at home as much as possible, going out only for critical needs like groceries and medicines, or to exercise and enjoy the outdoors in wide open spaces. Other recommendations include avoiding gatherings of more than 10 people, no handshakes, regular handwashing, and, when encountering someone outside of your immediate household, trying to remain at least 6 feet apart.
These may sound like extreme measures. But the new study by NIH-funded researchers, published in the journal Science, documents why social distancing may be our best hope to slow the spread of COVID-19 [1]. Here are a few highlights of the paper, which looks back to January 2020 and mathematically models the spread of the coronavirus within China:
• For every confirmed case of COVID-19, there are likely another five to 10 people with undetected infections.
• Although they are thought to be only about half as infectious as individuals with confirmed COVID-19, individuals with undetected infections were so prevalent in China that they apparently were the infection source for 86 percent of confirmed cases.
• After China established travel restrictions and social distancing, the spread of COVID-19 slowed considerably.
The findings come from a small international research team that included NIH grantee Jeffrey Shaman, Columbia University Mailman School of Public Health, New York. The team developed a computer model that enabled researchers to simulate the time and place of infections in a grid of 375 Chinese cities. The researchers did so by combining existing data on the spread of COVID-19 in China with mobility information collected by a location-based service during the country’s popular 40-day Spring Festival, when travel is widespread.
As these new findings clearly demonstrate, each of us must take social distancing seriously in our daily lives. Social distancing helped blunt the pandemic in China, and it will work in other nations, including the United States. While many Americans will likely spend weeks working and studying from home and practicing other social distancing measures, the stakes remain high. If this pandemic isn’t contained, this novel coronavirus could well circulate around the globe for years to come, at great peril to us and our loved ones.
As we commit ourselves to spending more time at home, progress continues to be made in using the power of biomedical research to combat this novel coronavirus. A notable step this week was the launch of an early-stage human clinical trial of an investigational vaccine, called mRNA-1273, to protect against COVID-19 [2]. The vaccine candidate was developed by researchers at NIH’s National Institute of Allergy and Infectious Diseases (NIAID) and their collaborators at the biotechnology company Moderna, Inc., Cambridge, MA.
This Phase 1 NIAID-supported trial will look at the safety of the vaccine—which cannot cause infection because it is made of RNA, not the whole coronavirus—in 45 healthy adults. The first volunteer was injected this past Monday at Kaiser Permanente Washington Health Research Institute, Seattle. If all goes well and larger follow-up clinical studies establish the vaccine’s safety and efficacy, it will then be necessary to scale up production to make millions of doses. While initiating this trial in record time is reason for hope, it is important to be realistic about all of the steps that still remain. If the vaccine candidate proves safe and effective, it will likely take at least 12–18 months before it would be widely available.
In the meantime, social distancing remains one of the best weapons we have to slow the silent spread of this virus and flatten the curve of the COVID-19 pandemic. This will give our health-care professionals, hospitals, and other institutions more valuable time to prepare, protect themselves, and aid the many people whose lives may be on the line from this coronavirus.
Importantly, saving lives from COVID-19 requires all of us—young, old and in-between—to take part. Healthy young people, whose risk of dying from coronavirus is not zero but quite low, might argue that they shouldn’t be constrained by social distancing. However, the research highlighted here demonstrates that such individuals are often the unwitting vector for a dangerous virus that can do great harm—and even take the lives of older and more vulnerable people. Think about your grandparents. Then skip the big gathering. We are all in this together
References:
[1] Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2). Li R, Pei S, Chen B, Song Y, Zhang T, Yang W, Shaman J. Science. 16 March 2020. [Preprint ahead of publication]
[2] NIH clinical trial of investigational vaccine for COVID-19 begins. NIH News Release, March 16, 2020.
Links:
Coronavirus (COVID-19) (NIH)
COVID-19, MERS & SARS (National Institute of Allergy and Infectious Diseases/NIH)
Coronavirus (COVID-19) (Centers for Disease Control and Prevention, Atlanta)
NIH Support: National Institute of Allergy and Infectious Diseases; National Institute of General Medical Sciences
Structural Biology Points Way to Coronavirus Vaccine
Posted on by Dr. Francis Collins
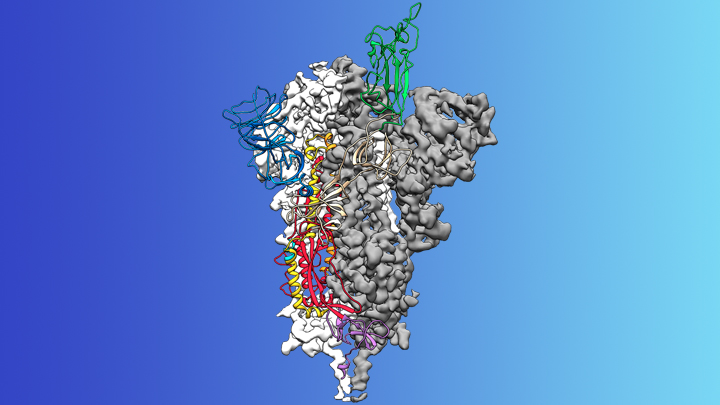
Credit: McLellan Lab, University of Texas at Austin
The recent COVID-19 outbreak of a novel type of coronavirus that began in China has prompted a massive global effort to contain and slow its spread. Despite those efforts, over the last month the virus has begun circulating outside of China in multiple countries and territories.
Cases have now appeared in the United States involving some affected individuals who haven’t traveled recently outside the country. They also have had no known contact with others who have recently arrived from China or other countries where the virus is spreading. The NIH and other U.S. public health agencies stand on high alert and have mobilized needed resources to help not only in its containment, but in the development of life-saving interventions.
On the treatment and prevention front, some encouraging news was recently reported. In record time, an NIH-funded team of researchers has created the first atomic-scale map of a promising protein target for vaccine development [1]. This is the so-called spike protein on the new coronavirus that causes COVID-19. As shown above, a portion of this spiky surface appendage (green) allows the virus to bind a receptor on human cells, causing other portions of the spike to fuse the viral and human cell membranes. This process is needed for the virus to gain entry into cells and infect them.
Preclinical studies in mice of a candidate vaccine based on this spike protein are already underway at NIH’s Vaccine Research Center (VRC), part of the National Institute of Allergy and Infectious Diseases (NIAID). An early-stage phase I clinical trial of this vaccine in people is expected to begin within weeks. But there will be many more steps after that to test safety and efficacy, and then to scale up to produce millions of doses. Even though this timetable will potentially break all previous speed records, a safe and effective vaccine will take at least another year to be ready for widespread deployment.
Coronaviruses are a large family of viruses, including some that cause “the common cold” in healthy humans. In fact, these viruses are found throughout the world and account for up to 30 percent of upper respiratory tract infections in adults.
This outbreak of COVID-19 marks the third time in recent years that a coronavirus has emerged to cause severe disease and death in some people. Earlier coronavirus outbreaks included SARS (severe acute respiratory syndrome), which emerged in late 2002 and disappeared two years later, and MERS (Middle East respiratory syndrome), which emerged in 2012 and continues to affect people in small numbers.
Soon after COVID-19 emerged, the new coronavirus, which is closely related to SARS, was recognized as its cause. NIH-funded researchers including Jason McLellan, an alumnus of the VRC and now at The University of Texas at Austin, were ready. They’d been studying coronaviruses in collaboration with NIAID investigators for years, with special attention to the spike proteins.
Just two weeks after Chinese scientists reported the first genome sequence of the virus [2], McLellan and his colleagues designed and produced samples of its spike protein. Importantly, his team had earlier developed a method to lock coronavirus spike proteins into a shape that makes them both easier to analyze structurally via the high-resolution imaging tool cryo-electron microscopy and to use in vaccine development efforts.
After locking the spike protein in the shape it takes before fusing with a human cell to infect it, the researchers reconstructed its atomic-scale 3D structural map in just 12 days. Their results, published in Science, confirm that the spike protein on the virus that causes COVID-19 is quite similar to that of its close relative, the SARS virus. It also appears to bind human cells more tightly than the SARS virus, which may help to explain why the new coronavirus appears to spread more easily from person to person, mainly by respiratory transmission.
McLellan’s team and his NIAID VRC counterparts also plan to use the stabilized spike protein as a probe to isolate naturally produced antibodies from people who’ve recovered from COVID-19. Such antibodies might form the basis of a treatment for people who’ve been exposed to the virus, such as health care workers.
The NIAID is now working with the biotechnology company Moderna, Cambridge, MA, to use the latest findings to develop a vaccine candidate using messenger RNA (mRNA), molecules that serve as templates for making proteins. The goal is to direct the body to produce a spike protein in such a way to elicit an immune response and the production of antibodies. An early clinical trial of the vaccine in people is expected to begin in the coming weeks. Other vaccine candidates are also in preclinical development.
Meanwhile, the first clinical trial in the U.S. to evaluate an experimental treatment for COVID-19 is already underway at the University of Nebraska Medical Center’s biocontainment unit [3]. The NIH-sponsored trial will evaluate the safety and efficacy of the experimental antiviral drug remdesivir in hospitalized adults diagnosed with COVID-19. The first participant is an American who was repatriated after being quarantined on the Diamond Princess cruise ship in Japan.
As noted, the risk of contracting COVID-19 in the United States is currently low, but the situation is changing rapidly. One of the features that makes the virus so challenging to stay in front of is its long latency period before the characteristic flu-like fever, cough, and shortness of breath manifest. In fact, people infected with the virus may not show any symptoms for up to two weeks, allowing them to pass it on to others in the meantime. You can track the reported cases in the United States on the Centers for Disease Control and Prevention’s website.
As the outbreak continues over the coming weeks and months, you can be certain that NIH and other U.S. public health organizations are working at full speed to understand this virus and to develop better diagnostics, treatments, and vaccines.
References:
[1] Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Wrapp D, Wang N, Corbett KS, Goldsmith JA, Hsieh CL, Abiona O, Graham BS, McLellan JS. Science. 2020 Feb 19.
[2] A new coronavirus associated with human respiratory disease in China. Wu F, Zhao S, Yu B, Chen YM, Wang W, Song ZG, Hu Y, Tao ZW, Tian JH, Pei YY, Yuan ML, Zhang YL, Dai FH, Liu Y, Wang QM, Zheng JJ, Xu L, Holmes EC, Zhang YZ. Nature. 2020 Feb 3.
[3] NIH clinical trial of remdesivir to treat COVID-19 begins. NIH News Release. Feb 25, 2020.
Links:
Coronaviruses (National Institute of Allergy and Infectious Diseases/NIH)
Coronavirus (COVID-19) (NIAID)
Coronavirus Disease 2019 (Centers for Disease Control and Prevention, Atlanta)
NIH Support: National Institute of Allergy and Infectious Diseases
Celebrating 2019 Biomedical Breakthroughs
Posted on by Dr. Francis Collins

Happy New Year! As we say goodbye to the Teens, let’s take a look back at 2019 and some of the groundbreaking scientific discoveries that closed out this remarkable decade.
Each December, the reporters and editors at the journal Science select their breakthrough of the year, and the choice for 2019 is nothing less than spectacular: An international network of radio astronomers published the first image of a black hole, the long-theorized cosmic singularity where gravity is so strong that even light cannot escape [1]. This one resides in a galaxy 53 million light-years from Earth! (A light-year equals about 6 trillion miles.)
Though the competition was certainly stiff in 2019, the biomedical sciences were well represented among Science’s “runner-up” breakthroughs. They include three breakthroughs that have received NIH support. Let’s take a look at them:
In a first, drug treats most cases of cystic fibrosis: Last October, two international research teams reported the results from phase 3 clinical trials of the triple drug therapy Trikafta to treat cystic fibrosis (CF). Their data showed Trikafta effectively compensates for the effects of a mutation carried by about 90 percent of people born with CF. Upon reviewing these impressive data, the Food and Drug Administration (FDA) approved Trikafta, developed by Vertex Pharmaceuticals.
The approval of Trikafta was a wonderful day for me personally, having co-led the team that isolated the CF gene 30 years ago. A few years later, I wrote a song called “Dare to Dream” imagining that wonderful day when “the story of CF is history.” Though we’ve still got more work to do, we’re getting a lot closer to making that dream come true. Indeed, with the approval of Trikafta, most people with CF have for the first time ever a real chance at managing this genetic disease as a chronic condition over the course of their lives. That’s a tremendous accomplishment considering that few with CF lived beyond their teens as recently as the 1980s.
Such progress has been made possible by decades of work involving a vast number of researchers, many funded by NIH, as well as by more than two decades of visionary and collaborative efforts between the Cystic Fibrosis Foundation and Aurora Biosciences (now, Vertex) that built upon that fundamental knowledge of the responsible gene and its protein product. Not only did this innovative approach serve to accelerate the development of therapies for CF, it established a model that may inform efforts to develop therapies for other rare genetic diseases.
Hope for Ebola patients, at last: It was just six years ago that news of a major Ebola outbreak in West Africa sounded a global health emergency of the highest order. Ebola virus disease was then recognized as an untreatable, rapidly fatal illness for the majority of those who contracted it. Though international control efforts ultimately contained the spread of the virus in West Africa within about two years, over 28,600 cases had been confirmed leading to more than 11,000 deaths—marking the largest known Ebola outbreak in human history. Most recently, another major outbreak continues to wreak havoc in northeastern Democratic Republic of Congo (DRC), where violent civil unrest is greatly challenging public health control efforts.
As troubling as this news remains, 2019 brought a needed breakthrough for the millions of people living in areas susceptible to Ebola outbreaks. A randomized clinical trial in the DRC evaluated four different drugs for treating acutely infected individuals, including an antibody against the virus called mAb114, and a cocktail of anti-Ebola antibodies referred to as REGN-EB3. The trial’s preliminary data showed that about 70 percent of the patients who received either mAb114 or the REGN-EB3 antibody cocktail survived, compared with about half of those given either of the other two medicines.
So compelling were these preliminary results that the trial, co-sponsored by NIH’s National Institute of Allergy and Infectious Diseases (NIAID) and the DRC’s National Institute for Biomedical Research, was halted last August. The results were also promptly made public to help save lives and stem the latest outbreak. All Ebola patients in the DRC treatment centers now are treated with one or the other of these two options. The trial results were recently published.
The NIH-developed mAb114 antibody and the REGN-EB3 cocktail are the first therapeutics to be shown in a scientifically rigorous study to be effective at treating Ebola. This work also demonstrates that ethically sound clinical research can be conducted under difficult conditions in the midst of a disease outbreak. In fact, the halted study was named Pamoja Tulinde Maisha (PALM), which means “together save lives” in Kiswahili.
To top off the life-saving progress in 2019, the FDA just approved the first vaccine for Ebola. Called Ervebo (earlier rVSV-ZEBOV), this single-dose injectable vaccine is a non-infectious version of an animal virus that has been genetically engineered to carry a segment of a gene from the Zaire species of the Ebola virus—the virus responsible for the current DRC outbreak and the West Africa outbreak. Because the vaccine does not contain the whole Zaire virus, it can’t cause Ebola. Results from a large study in Guinea conducted by the WHO indicated that the vaccine offered substantial protection against Ebola virus disease. Ervebo, produced by Merck, has already been given to over 259,000 individuals as part of the response to the DRC outbreak. The NIH has supported numerous clinical trials of the vaccine, including an ongoing study in West Africa.
Microbes combat malnourishment: Researchers discovered a few years ago that abnormal microbial communities, or microbiomes, in the intestine appear to contribute to childhood malnutrition. An NIH-supported research team followed up on this lead with a study of kids in Bangladesh, and it published last July its groundbreaking finding: that foods formulated to repair the “gut microbiome” helped malnourished kids rebuild their health. The researchers were able to identify a network of 15 bacterial species that consistently interact in the gut microbiomes of Bangladeshi children. In this month-long study, this bacterial network helped the researchers characterize a child’s microbiome and/or its relative state of repair.
But a month isn’t long enough to determine how the new foods would help children grow and recover. The researchers are conducting a similar study that is much longer and larger. Globally, malnutrition affects an estimated 238 million children under the age 5, stunting their normal growth, compromising their health, and limiting their mental development. The hope is that these new foods and others adapted for use around the world soon will help many more kids grow up to be healthy adults.
Measles Resurgent: The staff at Science also listed their less-encouraging 2019 Breakdowns of the Year, and unfortunately the biomedical sciences made the cut with the return of measles in the U.S. Prior to 1963, when the measles vaccine was developed, 3 to 4 million Americans were sickened by measles each year. Each year about 500 children would die from measles, and many more would suffer lifelong complications. As more people were vaccinated, the incidence of measles plummeted. By the year 2000, the disease was even declared eliminated from the U.S.
But, as more parents have chosen not to vaccinate their children, driven by the now debunked claim that vaccines are connected to autism, measles has made a very preventable comeback. Last October, the Centers for Disease Control and Prevention (CDC) reported an estimated 1,250 measles cases in the United States at that point in 2019, surpassing the total number of cases reported annually in each of the past 25 years.
The good news is those numbers can be reduced if more people get the vaccine, which has been shown repeatedly in many large and rigorous studies to be safe and effective. The CDC recommends that children should receive their first dose by 12 to 15 months of age and a second dose between the ages of 4 and 6. Older people who’ve been vaccinated or have had the measles previously should consider being re-vaccinated, especially if they live in places with low vaccination rates or will be traveling to countries where measles are endemic.
Despite this public health breakdown, 2019 closed out a memorable decade of scientific discovery. The Twenties will build on discoveries made during the Teens and bring us even closer to an era of precision medicine to improve the lives of millions of Americans. So, onward to 2020—and happy New Year!
Reference:
[1] 2019 Breakthrough of the Year. Science, December 19, 2019.
NIH Support: These breakthroughs represent the culmination of years of research involving many investigators and the support of multiple NIH institutes.
How Measles Leave the Body Prone to Future Infections
Posted on by Dr. Francis Collins

As a kid who was home-schooled on a Virginia farm in the 1950s, I wasn’t around other kids very much, and so didn’t get exposed to measles. And there was no vaccine yet. Later on as a medical resident, I didn’t recognize that I wasn’t immune. So when I was hospitalized with a severe febrile illness at age 29, it took a while to figure out the diagnosis. Yes, it was measles. I have never been that sick before or since. I was lucky not to have long-term consequences, and now I’m learning that there may be even more to consider.
With the big push to get kids vaccinated, you’ve probably heard about some of the very serious complications of measles: hearing-threatening ear infections, bronchitis, laryngitis, and even life-threatening forms of pneumonia and encephalitis. But now comes word of yet another way in which the measles can be devastating—one that may also have long-term consequences for a person’s health.
In a new study in the journal Science, a research team, partly funded by NIH, found that the measles virus not only can make children deathly ill, it can cause their immune systems to forget how to ward off other common infections [1]. The virus does this by wiping out up to nearly three-quarters of the protective antibodies that a child’s body has formed in response to past microbial invaders and vaccinations. This immune “amnesia” can leave a child more vulnerable to re-contracting infections, such as influenza or respiratory syncytial virus (RSV), that they may have been protected against before they came down with measles.
The finding comes as yet another reason to feel immensely grateful that, thanks to our highly effective vaccination programs, most people born in the U.S. from the 1960s onward should never have to experience the measles.
There had been hints that the measles virus might somehow suppress a person’s immune system. Epidemiological evidence also had suggested that measles infections might lead to increased susceptibility to infection for years afterwards [2]. Scientists had even suspected this might be explained by a kind of immune amnesia. The trouble was that there wasn’t any direct proof that such a phenomenon actually existed.
In the new work, the researchers, led by Michael Mina, Tomasz Kula, and Stephen Elledge, Howard Hughes Medical Institute and Brigham and Women’s Hospital, Boston, took advantage of a tool developed a few years ago in the Elledge lab called VirScan [3]. VirScan detects antibodies in blood samples acquired as a result of a person’s past encounters with hundreds of viruses, bacteria, or vaccines, providing a comprehensive snapshot of acquired immunity at a particular moment in time.
To look for evidence of immune amnesia following the measles, the research team needed blood samples gathered from people both before and after infection. These types of samples are currently hard to come by in the U.S. thanks to the success of vaccines. By partnering with Rik de Swart, Erasmus University Medical Center, Rotterdam, Netherlands, they found the samples that they needed.
During a recent measles outbreak in the Netherlands, de Swart had gathered blood samples from children living in communities with low vaccination rates. Elledge’s group used VirScan with 77 unvaccinated kids to measure antibodies in samples collected before and about two months after their measles infections.
That included 34 children who had mild infections and 43 who had severe measles. The researchers also examined blood samples from five children who remained uninfected and 110 kids who hadn’t been exposed to the measles virus.
The VirScan data showed that the infected kids, not surprisingly, produced antibodies to the measles virus. But their other antibodies dropped and seemed to be disappearing. In fact, depending on the severity of measles infection, the kids showed on average a loss of around 40 percent of their antibody memory, with greater losses in children with severe cases of the measles. In at least one case, the loss reached a whopping 73 percent.
This all resonates with me. I do recall that after my bout with the measles, I seemed to be coming down with a lot of respiratory infections. I attributed that to the lifestyle of a medical resident—being around lots of sick patients and not getting much sleep. But maybe it was more than that.
The researchers suggest that the loss of immune memory may stem from the measles virus destroying some of the long-lived cells in bone marrow. These cells remember past infections and, based on that immunological memory, churn out needed antibodies to thwart reinvading viruses.
Interestingly, after a measles infection, the children’s immune systems still responded to new infections and could form new immune memories. But it appears the measles caused long term, possibly permanent, losses of a significant portion of previously acquired immunities. This loss of immune memory put the children at a distinct disadvantage should those old bugs circulate again.
It’s important to note that, unlike measles infection, the MMR (measles, mumps, rubella) vaccine does NOT compromise previously acquired immunity. So, these findings come as yet another reminder of the public value of measles vaccination.
Prior to 1963, when the measles vaccine was developed, 3 to 4 million Americans got the measles each year. As more people were vaccinated, the incidence of measles plummeted. By the year 2000, the disease was declared eliminated from the U.S.
Unfortunately, measles has made a come back, fueled by vaccine refusals. In October, the Centers for Disease Control and Prevention (CDC) reported an estimated 1,250 measles cases in the United States so far in 2019, surpassing the total number of cases reported annually in each of the past 25 years [4].
Around the world, measles continues to infect 7 million people each year, leading to an estimated 120,000 deaths. Based on the new findings, Elledge’s team now suspects the actual toll of the measles may be five times greater, due to the effects of immune amnesia.
The good news is those numbers can be reduced if more people get the vaccine, which has been shown repeatedly in many large and rigorous studies to be safe and effective. The CDC recommends that children should receive their first dose by 12 to 15 months of age and a second dose between the ages of 4 and 6. Older people who’ve been vaccinated or have had the measles previously should consider being re-vaccinated, especially if they live in places with low vaccination rates or will be traveling to countries where measles are endemic.
References:
[1] Measles virus infection diminishes preexisting antibodies that offer protection from other pathogens. Mina MJ, Kula T, Leng Y, Li M, de Vries RD, Knip M, Siljander H, Rewers M, Choy DF, Wilson MS, Larman HB, Nelson AN, Griffin DE, de Swart RL, Elledge SJ. et al. Science. 2019 Nov 1; 366 (6465): 599-606.
[2] Long-term measles-induced immunomodulation increases overall childhood infectious disease mortality. Mina MJ, Metcalf CJE, De Swart RL, Osterhaus ADME, Grenfell BT. Science. 2015 May 8; 348(6235).
[3] Viral immunology. Comprehensive serological profiling of human populations using a synthetic human virome. Xu GJ, Kula T, Xu Q, Li MZ, Vernon SD, Ndung’u T, Ruxrungtham K, Sanchez J, Brander C, Chung RT, O’Connor KC, Walker B, Larman HB, Elledge SJ. Science. 2015 Jun 5;348(6239):aaa0698.
[4] Measles cases and outbreaks. Centers for Disease Control and Prevention. Oct. 11, 2019.
Links:
Measles (MedlinePlus Medical Encyclopedia/National Library of Medicine/NIH)
Measles History (Centers for Disease Control and Prevention)
Vaccines (National Institute of Allergy and Infectious Diseases/NIAID)
Vaccines Protect Your Community (Vaccines.gov)
Elledge Lab (Harvard Medical School, Boston)
NIH Support: National Institute of Allergy and Infectious Diseases; National Institute of Diabetes and Digestive and Kidney Diseases
Next Page