epidemic
Coping with the Collision of Public Health Crises: COVID-19 and Substance Use Disorders
Posted on by Dr. Francis Collins

For the past half-dozen years, I’ve had the privilege of attending the Rx Drug and Heroin Abuse Summit. And I was counting on learning more about this national crisis this April in Nashville, where I was scheduled to take part in a session with Dr. Nora Volkow, Director of NIH’s National Institute on Drug Abuse. But because of the physical distancing needed to help flatten the deadly curve of the coronavirus-19 (COVID-19) pandemic, it proved to be impossible for anyone to attend in person. Still, the summit did go on for almost three days—virtually!
Dr. Volkow and I took part by sharing a video of a recent conversation we had via videoconference. Since we couldn’t take live questions, we solicited some in advance. Here’s a condensed transcript highlighting portions of our dialogue that focused on the impact of the COVID-19 pandemic on individuals struggling with substance abuse disorders, along with all those who are trying to help them.
VOLKOW: Hello, Francis. Nice to see you, virtually!
COLLINS: Nice to see you too. I’m in my home office here, where I’ve been pretty much for the last three weeks. I’ve been stepping outdoors to occasionally get a breath of fresh air, but trying to live up to all those recommendations about social distancing—or at least physical distancing. I’m trying to keep my social connections going, even if they’re electronic.
I think we’re all feeling this is a time of some stress for us at NIH. We are trying to do everything we can to address this COVID crisis and speed up the process of developing vaccines and therapeutics and all kinds of other things. How are you doing? What’s it like being sequestered back in your home space when you are somebody with so much energy?
VOLKOW: Francis, it’s not easy. I actually am very, very restless. We probably are all experiencing that anxiety of uncertainty, looking at the news and how devastating it is. But I think what makes it easier is if we can do something. Working with everything that we have to try to help others, I think, provides some relief.
COLLINS: Yes, we’re going to talk about that right now. In fact, let’s talk about the way in which this crisis, the global pandemic called COVID-19, is colliding with another public health crisis, which is that of substance use disorder. You recently wrote about this collision in an article in the Annals of Internal Medicine. What does this mean? What are some of the unique challenges that COVID-19 brings to people suffering from addiction?
VOLKOW: I’m glad you are bringing up this point because it’s one of the issues of greatest concern for all of us who are working in the field of substance use disorders. We had not yet been able to contain the epidemic of opioid fatalities, and then we were hit by this tsunami of COVID.
We immediately can recognize the unique challenges of COVID-19 for people having an addiction. Some of these are structural; the healthcare system is not prepared to take care of them. They relate also to stigma and social issues. The concept of social distancing makes such people even more vulnerable because it interferes with many of the support systems that can help them to reach recovery. And, on top of that, drugs themselves negatively influence human physiology, making one more vulnerable to getting infected and more vulnerable to worse outcomes. So that’s why there is tremendous concern about these two epidemics colliding with one another.
COLLINS: How has this influenced treatment delivery for people with substance use disorders, who are counting on that to be able to keep themselves from slipping backward?
VOLKOW: Well, that has been very challenging. We’re hearing from multiple sources that it’s become harder for patients to be able to access treatment. And that relates, for example, to access of medications for opioid use disorders, which are the main strategy—and the most effective one—that we have to prevent people from dying from overdoses.
Some clinics are decreasing the number of patients that they can take care of. The healthcare system is also much less able to initiate persons on buprenorphine. And because of social isolation, if you overdose, the likelihood that someone can rescue you with naloxone is much lower. We don’t yet have statistics on about how that’s influencing fatalities, but we are very concerned.
COLLINS: Nora, you are one of the lead persons for NIH’s Helping to End Addiction Long-term (HEAL) initiative. How has the COVID-19 pandemic affected all the grand research plans that we had put in place as part of our big vision of how NIH could help with the substance use disorder crisis?
VOLKOW: Well, $900 million had recently been deployed on research. That is incredibly meritorious, and some of that research had already started. Unfortunately, it has had to stop almost completely. Why? Because the research that’s relying on the healthcare system, for example, is no longer able to focus on research when they have other clinical needs to meet.
Also, research to bring medication-assisted treatments to prison inmates has stopped. Prisons are not allowing the researchers to go on site because they are closing the doors to outsiders, since they are places at high risk for the spread of COVID-19. Furthermore, some institutional review boards (IRBs) are actually closing, making it impossible to recruit patients for the clinical trials. So, most studies have come to a halt. The issue now is how can we become creative and use virtual technologies to advance some of the goals that we aim to achieve with the HEAL initiative.
COLLINS: Of course, this applies to many other areas of NIH-supported research. Most clinical trials, unless they’re for life-threating conditions, are pretty much in a state of hibernation. We can’t justify having people get out there in ways that might put them at risk of COVID-19. So, yes, it’s a tough time for clinical research all over. And that’s certainly what’s happened with the opioid use disorder problems. Still, I think our teams are really devoted to making sure they make the best of this time, doing things that they can do in terms of planning and setting up data systems.
Meanwhile, bring us up to date on what’s happened as far as the state of the opioid crisis. Are there trends there that we ought to look at for a minute?
VOLKOW: Yes, it’s important to actually keep our eyes on the epidemic, because it’s changing so very rapidly. It’s gone from prescription opioids to heroin to synthetic opioids like fentanyl. And what we have observed ramping up over the past two or three years is an increase in fatalities from the use of psychostimulant drugs.
For example, the number of deaths from methamphetamine has increased five-fold over a period of six years. Similarly, deaths from cocaine are going up. The reality is that people are now dying not just from opioids, but from mixtures of drugs and stimulant drugs, most notably methamphetamine.
COLLINS: So, what can we learn from what we’ve been doing about opioid addiction, and try to apply that to this emerging methamphetamine crisis?
VOLKOW: Unfortunately, we do not have effective medications to treat methamphetamine addiction like we do for opioid use disorders. We also do not have an overdose reversal like we have with naloxone. So, in that respect, it is more challenging.
COLLINS: People sometimes think we’re only focused on trying to treat the problems that we have now. What about prevention? One of the questions we received in our HEAL mailbox was: How can small town communities create an environment where addiction does not take root in the next generation of young people? I’m sure you want to talk about the rewarding power of social interactions, even though right now we’re being somewhat deprived of those, at least face-to-face.
VOLKOW: I’m glad you’re bringing up that question, Francis. Because when you asked at the start of our conversation about how I am doing, I sort of said, “Well, it’s not easy.” But the positive component was that sense that we have a shared mission: we can help others. And the lack of a sense of mission, the lack of a purpose in life, has been identified as one of the factors that make people more vulnerable to take drugs.
Feeling irrelevant, feeling that no one cares for you, is probably one of the most devastating feelings a human being can have. Epidemiological studies show that social isolation and neglect increase dramatically the risk of taking drugs, and, if you are trying to stop taking drugs, it increases that risk of relapse. And so that’s an issue right now of great concern. The challenge is “How do we provide social support for people at risk of substance abuse during the COVID-19 pandemic?”
Also, independent of COVID-19, I think that we as a nation have to face the concept that we have made America vulnerable to drugs because we have eroded that social sense of community. If we are to prevent future generations from getting addicted to drugs, we should build meaningful interactions between people. We should give each individual an opportunity to be part of a society that appreciates them. We do need each other in very, very fundamental ways. We need others for our well-being. If we don’t have that then we become very vulnerable.
COLLINS: Well, here’s one last question from the mailbox. Somebody notes that the “L” in HEAL stands for “long-term.” That is, Helping End Addiction Long-term. The questioner asks: “What’s our vision of a long-term goal and how do we imagine getting there?”
Mine very simply is that we would have an environment that would support people in productive ways, so that the distractions of things that turn out to be destructive are not so tempting, and that the possibility of having meaning in everyone’s life becomes greater.
Ironically, because of COVID-19, we are in the midst of a circumstance where economic distress is pressing on people and social distancing is being required. Seems like we’re going the wrong way. But if you look back in history, often these times of national crisis have been times when people did have the chance to survey what really matters around them, and perhaps to regain a sense of meaning and significance. That’s my maybe slightly over-optimistic view of the current era that we’re in.
Nora, what do you think?
VOLKOW: Francis, I will agree with you. I think that we need to create a society that provides social support and allows people to participate in a meaningful way. If we want to achieve integration of people into society, one of the things that we need to do urgently is remove the stigma of addiction because when you stigmatise someone, you are socially isolating them.
No one likes to be mistreated or discriminated against. So, if you are a person who is addicted and you are afraid of discrimination, you will not seek help. You will continue to isolate. So I think as we’re dealing with the opioid crisis, as we’re dealing with COVID-19, we cannot tolerate discrimination. We cannot tolerate stigma. And we need to be very creative to identify it and to create models that will actually eliminate it.
COLLINS: That’s a wonderful view of where we need to get to. All of these developments give me hope for our capacity to deal with this crisis by working together.
I want to say to all of you who’re listening to this in your own virtual spaces, how much I admire the work that you all are doing, in a selfless way, to try to help our nation deal with what has clearly been a terrible tragedy in far too many lives. I wish you all the best in continuing those creative and energetic efforts, even in the midst of the COVID-19 pandemic. NIH wants to be your ally. We want to be your source of information. We want to be your source of evidence for what works. We want to be your friends.
So, thank you for listening, and thank you, Nora Volkow, for joining me in this discussion today with all of the talent and leadership that you represent. I wish the best health to all of you. Stay safe and keep the progress going!
Links:
Video: Fireside Chat Between NIH, NIDA Heads Addresses COVID-19, the HEAL Initiative, and the Opioids Crisis (National Institute on Drug Abuse/NIH)
COVID-19 Resources (NIDA)
COVID-19: Potential Implications for Individuals with Substance Use Disorders, Nora’s Blog (NIDA)
NIDA Director outlines potential risks to people who smoke and use drugs during COVID-19 pandemic (NIDA)
Collision of the COVID-19 and Addiction Epidemics. Volkow ND. Ann Intern Med. 2 April 2020. [Epub ahead of print]
Helping to End Addiction Long-term (HEAL) Initiative (NIH)
Rx Drug Abuse & Heroin Summit, A 2020 Virtual Experience
Can Smart Phone Apps Help Beat Pandemics?
Posted on by Dr. Francis Collins

In recent weeks, most of us have spent a lot of time learning about coronavirus disease 2019 (COVID-19) and thinking about what’s needed to defeat this and future pandemic threats. When the time comes for people to come out of their home seclusion, how will we avoid a second wave of infections? One thing that’s crucial is developing better ways to trace the recent contacts of individuals who’ve tested positive for the disease-causing agent—in this case, a highly infectious novel coronavirus.
Traditional contact tracing involves a team of public health workers who talk to people via the phone or in face-to-face meetings. This time-consuming, methodical process is usually measured in days, and can even stretch to weeks in complex situations with multiple contacts. But researchers are now proposing to take advantage of digital technology to try to get contact tracing done much faster, perhaps in just a few hours.
Most smart phones are equipped with wireless Bluetooth technology that creates a log of all opt-in mobile apps operating nearby—including opt-in apps on the phones of nearby people. This has prompted a number of research teams to explore the idea of creating an app to notify individuals of exposure risk. Specifically, if a smart phone user tests positive today for COVID-19, everyone on their recent Bluetooth log would be alerted anonymously and advised to shelter at home. In fact, in a recent paper in the journal Science, a British research group has gone so far to suggest that such digital tracing may be valuable in the months ahead to improve our chances of keeping COVID-19 under control [1].
The British team, led by Luca Ferretti, Christophe Fraser, and David Bonsall, Oxford University, started their analyses using previously published data on COVID-19 outbreaks in China, Singapore, and aboard the Diamond Princess cruise ship. With a focus on prevention, the researchers compared the different routes of transmission, including from people with and without symptoms of the infection.
Based on that data, they concluded that traditional contact tracing was too slow to keep pace with the rapidly spreading COVID-19 outbreaks. During the three outbreaks studied, people infected with the novel coronavirus had a median incubation period of about five days before they showed any symptoms of COVID-19. Researchers estimated that anywhere from one-third to one-half of all transmissions came from asymptomatic people during this incubation period. Moreover, assuming that symptoms ultimately arose and an infected person was then tested and received a COVID-19 diagnosis, public health workers would need at least several more days to perform the contact tracing by traditional means. By then, they would have little chance of getting ahead of the outbreak by isolating the infected person’s contacts to slow its rate of transmission.
When they examined the situation in China, the researchers found that available data show a correlation between the roll-out of smart phone contact-tracing apps and the emergence of what appears to be sustained suppression of COVID-19 infection. Their analyses showed that the same held true in South Korea, where data collected through a smart phone app was used to recommend quarantine.
Despite its potential benefits in controlling or even averting pandemics, the British researchers acknowledged that digital tracing poses some major ethical, legal, and social issues. In China, people were required to install the digital tracing app on their phones if they wanted to venture outside their immediate neighborhoods. The app also displayed a color-coded warning system to enforce or relax restrictions on a person’s movements around a city or province. The Chinese app also relayed to a central database the information that it had gathered on phone users’ movements and COVID-19 status, raising serious concerns about data security and privacy of personal information.
In their new paper, the Oxford team, which included a bioethicist, makes the case for increased social dialogue about how best to employ digital tracing in ways the benefit human health. This is a far-reaching discussion with implications far beyond times of pandemic. Although the team analyzed digital tracing data for COVID-19, the algorithms that drive these apps could be adapted to track the spread of other common infectious diseases, such as seasonal influenza.
The study’s authors also raised another vital point. Even the most-sophisticated digital tracing app won’t be of much help if smart phone users don’t download it. Without widespread installation, the apps are unable to gather enough data to enable effective digital tracing. Indeed, the researchers estimate that about 60 percent of new COVID-19 cases in a community would need to be detected–and roughly the same percentage of contacts traced—to squelch the spread of the deadly virus.
Such numbers have app designers working hard to discover the right balance between protecting public health and ensuring personal rights. That includes NIH grantee Trevor Bedford, Fred Hutchinson Cancer Research Center, Seattle. He and his colleagues just launched NextTrace, a project that aims to build an opt-in app community for “digital participatory contact tracing” of COVID-19. Here at NIH, we have a team that is actively exploring the kind of technology that could achieve the benefits without unduly compromising personal privacy.
Bedford emphasizes that he and his colleagues aren’t trying to duplicate efforts already underway. Rather, they want to collaborate with others help to build a scientifically and ethically sound foundation for digital tracing aimed at improving the health of all humankind.
Reference:
[1] Quantifying SARS-CoV-2 transmission suggests epidemic control with digital contact tracing. Ferretti L, Wymant C, Kendall M, Zhao L, Nurtay A, Abeler-Dörner L, Parker M, Bonsall D, Fraser C. Science. 2020 Mar 31. [Epub ahead of print]
Links:
Coronavirus (COVID-19) (NIH)
COVID-19, MERS & SARS (National Institute of Allergy and Infectious Diseases/NIH)
NextTrace (Fred Hutchinson Cancer Research Center, Seattle)
Bedford Lab (Fred Hutchinson Cancer Research Center)
NIH Support: National Institute of General Medical Sciences
Structural Biology Points Way to Coronavirus Vaccine
Posted on by Dr. Francis Collins
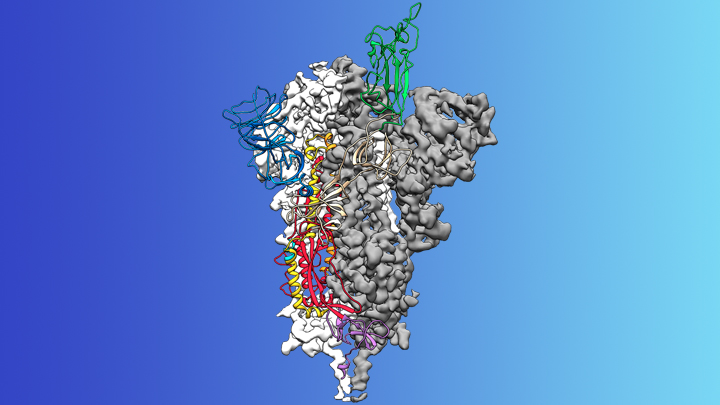
Credit: McLellan Lab, University of Texas at Austin
The recent COVID-19 outbreak of a novel type of coronavirus that began in China has prompted a massive global effort to contain and slow its spread. Despite those efforts, over the last month the virus has begun circulating outside of China in multiple countries and territories.
Cases have now appeared in the United States involving some affected individuals who haven’t traveled recently outside the country. They also have had no known contact with others who have recently arrived from China or other countries where the virus is spreading. The NIH and other U.S. public health agencies stand on high alert and have mobilized needed resources to help not only in its containment, but in the development of life-saving interventions.
On the treatment and prevention front, some encouraging news was recently reported. In record time, an NIH-funded team of researchers has created the first atomic-scale map of a promising protein target for vaccine development [1]. This is the so-called spike protein on the new coronavirus that causes COVID-19. As shown above, a portion of this spiky surface appendage (green) allows the virus to bind a receptor on human cells, causing other portions of the spike to fuse the viral and human cell membranes. This process is needed for the virus to gain entry into cells and infect them.
Preclinical studies in mice of a candidate vaccine based on this spike protein are already underway at NIH’s Vaccine Research Center (VRC), part of the National Institute of Allergy and Infectious Diseases (NIAID). An early-stage phase I clinical trial of this vaccine in people is expected to begin within weeks. But there will be many more steps after that to test safety and efficacy, and then to scale up to produce millions of doses. Even though this timetable will potentially break all previous speed records, a safe and effective vaccine will take at least another year to be ready for widespread deployment.
Coronaviruses are a large family of viruses, including some that cause “the common cold” in healthy humans. In fact, these viruses are found throughout the world and account for up to 30 percent of upper respiratory tract infections in adults.
This outbreak of COVID-19 marks the third time in recent years that a coronavirus has emerged to cause severe disease and death in some people. Earlier coronavirus outbreaks included SARS (severe acute respiratory syndrome), which emerged in late 2002 and disappeared two years later, and MERS (Middle East respiratory syndrome), which emerged in 2012 and continues to affect people in small numbers.
Soon after COVID-19 emerged, the new coronavirus, which is closely related to SARS, was recognized as its cause. NIH-funded researchers including Jason McLellan, an alumnus of the VRC and now at The University of Texas at Austin, were ready. They’d been studying coronaviruses in collaboration with NIAID investigators for years, with special attention to the spike proteins.
Just two weeks after Chinese scientists reported the first genome sequence of the virus [2], McLellan and his colleagues designed and produced samples of its spike protein. Importantly, his team had earlier developed a method to lock coronavirus spike proteins into a shape that makes them both easier to analyze structurally via the high-resolution imaging tool cryo-electron microscopy and to use in vaccine development efforts.
After locking the spike protein in the shape it takes before fusing with a human cell to infect it, the researchers reconstructed its atomic-scale 3D structural map in just 12 days. Their results, published in Science, confirm that the spike protein on the virus that causes COVID-19 is quite similar to that of its close relative, the SARS virus. It also appears to bind human cells more tightly than the SARS virus, which may help to explain why the new coronavirus appears to spread more easily from person to person, mainly by respiratory transmission.
McLellan’s team and his NIAID VRC counterparts also plan to use the stabilized spike protein as a probe to isolate naturally produced antibodies from people who’ve recovered from COVID-19. Such antibodies might form the basis of a treatment for people who’ve been exposed to the virus, such as health care workers.
The NIAID is now working with the biotechnology company Moderna, Cambridge, MA, to use the latest findings to develop a vaccine candidate using messenger RNA (mRNA), molecules that serve as templates for making proteins. The goal is to direct the body to produce a spike protein in such a way to elicit an immune response and the production of antibodies. An early clinical trial of the vaccine in people is expected to begin in the coming weeks. Other vaccine candidates are also in preclinical development.
Meanwhile, the first clinical trial in the U.S. to evaluate an experimental treatment for COVID-19 is already underway at the University of Nebraska Medical Center’s biocontainment unit [3]. The NIH-sponsored trial will evaluate the safety and efficacy of the experimental antiviral drug remdesivir in hospitalized adults diagnosed with COVID-19. The first participant is an American who was repatriated after being quarantined on the Diamond Princess cruise ship in Japan.
As noted, the risk of contracting COVID-19 in the United States is currently low, but the situation is changing rapidly. One of the features that makes the virus so challenging to stay in front of is its long latency period before the characteristic flu-like fever, cough, and shortness of breath manifest. In fact, people infected with the virus may not show any symptoms for up to two weeks, allowing them to pass it on to others in the meantime. You can track the reported cases in the United States on the Centers for Disease Control and Prevention’s website.
As the outbreak continues over the coming weeks and months, you can be certain that NIH and other U.S. public health organizations are working at full speed to understand this virus and to develop better diagnostics, treatments, and vaccines.
References:
[1] Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Wrapp D, Wang N, Corbett KS, Goldsmith JA, Hsieh CL, Abiona O, Graham BS, McLellan JS. Science. 2020 Feb 19.
[2] A new coronavirus associated with human respiratory disease in China. Wu F, Zhao S, Yu B, Chen YM, Wang W, Song ZG, Hu Y, Tao ZW, Tian JH, Pei YY, Yuan ML, Zhang YL, Dai FH, Liu Y, Wang QM, Zheng JJ, Xu L, Holmes EC, Zhang YZ. Nature. 2020 Feb 3.
[3] NIH clinical trial of remdesivir to treat COVID-19 begins. NIH News Release. Feb 25, 2020.
Links:
Coronaviruses (National Institute of Allergy and Infectious Diseases/NIH)
Coronavirus (COVID-19) (NIAID)
Coronavirus Disease 2019 (Centers for Disease Control and Prevention, Atlanta)
NIH Support: National Institute of Allergy and Infectious Diseases
How Influenza Pandemics Occur
Posted on by Dr. Francis Collins
| Credit: National Institute of Allergy and Infectious Diseases, NIH |
Flu season is upon us! Check out this NIH video to see how these pandemics emerge and spread new flu viruses around the globe.
The Diabetes Threat
Posted on by Dr. Francis Collins
The number of Americans diagnosed with type 2 diabetes rose from 1.5 million in 1958 to 18.8 million in 2010. That’s an increase of epidemic proportions. Even more disturbing, another 7 million Americans have type 2 diabetes, but don’t know it and, consequently, can’t take steps to control the disease. Altogether, over 8% of the U.S. population now has this potentially deadly metabolic condition.
- Type 2 diabetes wreaks havoc on the body by raising the levels of glucose in the blood, increasing the risk of blindness, heart disease, kidney failure, nerve damage, and even Alzheimer’s disease.
- Pre-diabetes is a condition in which blood glucose levels are higher than normal, but not high enough to be called diabetes. 79 million U.S. adults age 20 and older have pre-diabetes.
- NIH studies have shown that losing just 6–7% of body weight and increasing physical activity can prevent or delay pre-diabetes from progressing to diabetes. 85% of people with diabetes are overweight.

A View of the U.S. Obesity Epidemic
Posted on by Dr. Francis Collins
 in U.S. Adults in 1985")
 in U.S. Adults in 1995")
 in U.S. Adults in 2005")
 in U.S. Adults in 2010")
These snapshots reveal a very disturbing trend: the rise in obesity in the US from 1985 to 2010. Today one third of adults in the US are obese, another third are overweight.
Because obesity has risen to epidemic levels—causing devastating and costly health problems, reducing life expectancy, and provoking stigma and discrimination—the NIH has established the NIH Obesity Research Task Force to accelerate progress in obesity research. For example, why are some individuals more susceptible to obesity? Can knowledge of biology and behavior be leveraged to develop better intervention strategies? What strategies work? For whom? Can these approaches be scaled up?