Zika virus
This Is Why NIH Invests in Global Health Research
Posted on by Roger I. Glass, M.D., Ph.D., Fogarty International Center

Efforts over the past few years to end the COVID-19 pandemic clearly reveal how global health impacts individual wellbeing and national security. At NIH, the Fogarty International Center helps the other institutes become engaged with global health research, which investigates the dual burden of infectious disease and non-communicable disease.
Global health research also encompasses data science, economics, genetics, climate change science, and many other disciplines. For more than 50 years, Fogarty has been building partnerships among institutions in the U.S. and abroad, while training the next generation of scientists focused on universal health needs.
America’s investment in Fogarty has paid rich dividends
During the pandemic, in particular, we’ve seen researchers trained by our programs make scientific discoveries that contributed to international security. Take Jessica Manning, a former Fogarty fellow who now conducts malaria research in Phnom Penh, Cambodia. Her team at the Ministry of Health sequenced the viral strain of SARS-CoV-2, the cause of COVID-19, infecting the first Cambodian patient and documented early the spread of this novel coronavirus outside of China.
Similarly, Christian Happi, director of the African Centre of Excellence for the Genomics of Infectious Disease, Ede, Nigeria, sequenced the first SARS-CoV-2 genome in Africa. Happi was able to do it by adapting the sequencing and analytical pipelines that he’d created back when he was a Fogarty grantee studying Ebola.
In Botswana, Sikhulile Moyo leveraged the skills he’d acquired while supported by a Fogarty HIV research training grant with Max Essex, Harvard School of Public Health, Cambridge, MA, to track COVID-19 mutations for his country’s Ministry of Health. Last November, he alerted the world of a new Omicron variant. Within six weeks, Omicron became the dominant global strain, challenging the ability of COVID vaccines to control its spread. In the Dominican Republic, William Duke, a national commission member, used what he’d learned as a Fogarty trainee to help create a national COVID-19 intervention plan to prevent and control the disease.
Fogarty’s fostering of global health leaders is one way we advance scientific expertise while ensuring our nation’s biosecurity. Another is by finding effective ways to study abroad the same health conditions that affect our own population.
Research conducted in Colombia, for example, may provide clues for preventing Alzheimer’s disease in the U.S. Fogarty support brought together neuroscientists Kenneth Kosik, University of California, Santa Barbara, and Francisco Lopera, University of Antioquia, Colombia, to study members of the largest-known family with an early-onset, rapidly progressive form of the disease. Over the years, Kosik and Lopera have trained local scientists, explored gene therapy targets, investigated biomarkers to monitor disease progression, and conducted drug trials in search of a cure for Alzheimer’s.
Researchers in other fields also discover unique opportunities to investigate populations with high rates of disease. Siana Nkya, a Fogarty grantee based in Tanzania, has devoted her career to studying the genetic determinants of sickle cell disease, which affects many people around the world, including in the U.S. We hope that US-African partnerships might develop improved, affordable treatments and a cure for all patients with this devastating disease. Similarly, people in the U.S. have access to state-of-the-art HIV treatment studies in places around the globe where incidence rates are higher.
Fogarty has supported many milestone achievements in HIV research over the years. Among them is a study that took place in nine countries. The research, led by Myron Cohen of the University of North Carolina at Chapel Hill, established that antiretroviral therapy can prevent sexual transmission of HIV-1 among couples in which one person is infected and the other is not. In fact, this research informs current HIV treatment recommendations worldwide, including in the U.S.
Americans will also undoubtedly benefit from projects funded by Fogarty’s Global Brain and Nervous System Disorders Research across the Lifespan program. For example, psychologist Tatiana Balachova, University of Oklahoma, Oklahoma City, has designed an intervention for women in Russia to prevent fetal alcohol spectrum disorders. In another project in South Africa, Sandra and Joseph Jacobson, Wayne State University, Detroit, conducted the first-ever prospective longitudinal study of the syndrome. Findings from both projects are ripe for translation within an American context.
Other examples of Global Brain program investigations with broad implications in our own country include studying early psychosis in China; capacity building for schizophrenia research in Macedonia; exploring family consequences from the Zika virus in Brazil; and studying dementia and related health and social challenges in Lebanon.
These are just a few examples of Fogarty’s work and its unique mission. What is most remarkable about Fogarty is that just under 90 percent of our grants are co-funded by at least one other NIH institute, center, or office. Collaboration, both within borders and across them, is Fogarty’s formula for success.
Links:
Fogarty International Center (NIH)
Overview of Brain Disorders: Research Across the Lifespan (Fogarty)
Former Fogarty Scholar Dr Jessica Manning Helps Cambodia Respond to COVID (Fogarty)
Christian Happi: Former Fogarty Grantee Leads COVID-19 Genomics Work in Africa (Fogarty)
Sikhulile Moyo: Fogarty Fellow Recognized for Omicron Discovery (Fogarty)
William Duke: Former Fogarty HIV Trainee Helps Lead Dominican Republic’s COVID Response (Fogarty)
Kenneth Kosic and Francisco Lopera: NIH Support Spurs Alzheimer’s Research in Colombia (Fogarty)
Former Fogarty fellow Siana Nkya Tackles Sickle Cell Disease in Tanzania (Fogarty)
Tatiana Balachova: Researchers Tackle Fetal Alcohol Syndrome in Russia (Fogarty)
Sandra and Joseph Jacobson: Fetal Alcohol Exposure Research Supported by NIAAA in South Africa, Ukraine and Russia Improves Prevention, Outcomes (Fogarty)
Note: Dr. Lawrence Tabak, who performs the duties of the NIH Director, has asked the heads of NIH’s Institutes and Centers (ICs) to contribute occasional guest posts to the blog to highlight some of the interesting science that they support and conduct. This is the 22nd in the series of NIH IC guest posts that will run until a new permanent NIH director is in place.
Uncovering a Hidden Zika Outbreak in Cuba
Posted on by Dr. Francis Collins

When Brazilian health officials discovered four years ago that the mosquito-borne Zika virus could cause severe birth defects and other serious health problems, it prompted a major effort across the Americas to curb the infection by controlling mosquitoes and issuing travel advisories. By mid-2017, the hard work seemed to have paid off, and reports of new Zika infections had nearly stopped.
But it turns out Zika may be tougher to control than once thought. New research shows that a large, previously hidden outbreak of Zika virus disease occurred in Cuba, just when it looked like the worst of the epidemic was over. The finding suggests that the Zika virus can linger over long periods, and that mosquito control efforts alone may slow, but not necessarily stop, the march of this potentially devastating infectious disease.
When combating global epidemics, it’s critical to track the spread of dangerous viruses from one place to the next. But some viruses can be tougher to monitor than others, and that certainly has been the case with Zika in the Americas. Though the virus can harm unborn children, many people infected with Zika never feel lousy enough to go to the doctor. Those who do often have symptoms that overlap with other prevalent tropical diseases, such as dengue and chikungunya fever, making it hard to recognize Zika.
That’s why in Brazil, where Zika arrived in the Americas by early 2014, this unexpected viral intruder went undetected for well over a year. By then, it had spread unnoticed to Honduras, circulating rapidly to other Central American nations and Mexico—likely by late 2014 and into 2015.
In the United States, even with close monitoring, a small local outbreak of Zika virus in Florida also went undetected for about three months in 2016 [1]. Then, in 2017, Florida officials began noticing something strange: new cases of Zika infection in people who had traveled to Cuba.
This came as a real surprise because Cuba, unlike most other Caribbean islands, was thought to have avoided an outbreak. What’s more, by then the Zika epidemic in the Americas had slowed to a trickle, prompting the World Health Organization to delist it as a global public health emergency of international concern.
Given the Cuban observation, some wondered whether the Zika epidemic in the Americas was really over. Among them was an NIH-supported research team, including Nathan Grubaugh, Yale School of Public Health, New Haven, CT; Sharon Isern and Scott Michael, Florida Gulf Coast University, Fort Myers; and Kristian Andersen, The Scripps Research Institute, La Jolla, CA, who worked closely with the Florida Department of Health, including Andrea Morrison.
As published in Cell, the team was able to document a previously unreported outbreak in Cuba after the epidemic had seemingly ended [2]. Interestingly, another research group in Spain also recently made a similar observation about Zika in Cuba [3].
In the Cell paper, the researchers show that between June 2017 and October 2018, all but two of 155 cases—a whopping 98 percent of travel-associated Zika infections—traced back to Cuba. Further analysis suggests that the outbreak in Cuba was likely of similar magnitude to outbreaks that occurred in other Caribbean nations.
Their estimates suggest there were likely many thousands of Zika cases in Cuba, and more than 5,000 likely should have been diagnosed and reported in 2017. The only difference was the timing. The Cuban outbreak of Zika virus occurred about a year after infections subsided elsewhere in the Caribbean.
To fill in more of the blanks, the researchers relied on Zika virus genomes from nine infected Florida travelers who returned from Cuba in 2017 and 2018. The sequencing data support multiple introductions of Zika virus to Cuba from other Caribbean islands in the summer of 2016.
The outbreak peaked about a year after the virus made its way to Cuba, similar to what happened in other places. But the Cuban outbreak was likely delayed by a year thanks to an effective mosquito control campaign by local authorities, following detection of the Brazilian outbreak. While information is lacking, including whether Zika infections had caused birth defects, it’s likely those efforts were relaxed once the emergency appeared to be over elsewhere in the Caribbean, and the virus took hold.
The findings serve as yet another reminder that the Zika virus—first identified in the Zika Forest in Uganda in 1947 and for many years considered a mostly inconsequential virus [4]—has by no means been eliminated. Indeed, such unrecognized and delayed outbreaks of Zika raise the risk of travelers innocently spreading the virus to other parts of the world.
The encouraging news is that, with travel surveillance data and genomic tools —enabled by open science—it is now possible to detect such outbreaks. By combining resources and data, it will be possible to develop even more effective and responsive surveillance frameworks to pick up on emerging health threats in the future.
In the meantime, work continues to develop a vaccine for the Zika virus, with more than a dozen clinical trials underway that pursue a variety of vaccination strategies. With the Zika pandemic resolved in the Americas, these studies can be harder to conduct, since proof of efficacy is not possible without active infections. But, as this paper shows, we must remain ready for future outbreaks of this unique and formidable virus.
References:
[1] Genomic epidemiology reveals multiple introductions of Zika virus into the United States. Grubaugh et al. Nature. 2017 Jun 15;546(7658):401-405.
[2] Travel surveillance and genomics uncover a hidden Zika outbreak during the waning epidemic. Grubaugh ND, Saraf S, Gangavarapu K, Watts A, Tan AL, Oidtman RJ, Magnani DM, Watkins DI, Palacios G, Hamer DH; GeoSentinel Surveillance Network, Gardner LM, Perkins TA, Baele G, Khan K, Morrison A, Isern S, Michael SF, Andersen .KG, et. al. Cell. 2019 Aug 22;178(5):1057-1071.e11.
[3] Mirroring the Zika epidemics in Cuba: The view from a European imported diseases clinic. Almuedo-Riera A, Rodriguez-Valero N, Camprubí D, Losada Galván I, Zamora-Martinez C, Pousibet-Puerto J, Subirà C, Martinez MJ, Pinazo MJ, Muñoz J. Travel Med Infect Dis. 2019 Jul – Aug;30:125-127.
[4] Pandemic Zika: A Formidable Challenge to Medicine and Public Health. Morens DM, Fauci AS. J Infect Dis. 2017 Dec 16;216(suppl_10):S857-S859.
Links:
Video: Uncovering Hidden Zika Outbreaks (Florida Gulf Coast University, Fort Myers)
Zika Virus (National Institute of Allergy and Infectious Diseases/NIH)
Zika Virus Vaccines (NIAID)
Zika Free Florida (Florida Department of Health, Tallahassee)
Grubaugh Lab (Yale School of Public Health, New Haven, CT)
Andersen Lab (The Scripps Research Institute, La Jolla, CA)
NIH Support: National Institute of Allergy and Infectious Diseases; National Center for Advancing Translational Sciences
Tracing Spread of Zika Virus in the Americas
Posted on by Dr. Francis Collins

Caption: Here I am visiting the Ziika Forest area of Uganda, where the Zika virus was first identified in 1947.
Credit: National Institutes of Health
A couple of summers ago, the threat of mosquito-borne Zika virus disease in tropical areas of the Americas caused major concern, and altered the travel plans of many. The concern was driven by reports of Zika-infected women giving birth to babies with small heads and incompletely developed brains (microcephaly), as well as other serious birth defects. So, with another summer vacation season now upon us, you might wonder what’s become of Zika.
While pregnant women and couples planning on having kids should still take extra precautions [1] when travelling outside the country, the near-term risk of disease outbreaks has largely subsided because so many folks living in affected areas have already been exposed to the virus and developed protective immunity. But the Zika virus—first identified in the Ziika Forest in Uganda in 1947—has by no means been eliminated, making it crucial to learn more about how it spreads to avert future outbreaks. It’s very likely we have not heard the last of Zika in the Western hemisphere.
Recently, an international research team, partly funded by NIH, used genomic tools to trace the spread of the Zika virus. Genomic analysis can be used to build a “family tree” of viral isolates, and such analysis suggests that the first Zika cases in Central America were reported about a year after the virus had actually arrived and begun to spread.
The Zika virus, having circulated for decades in Africa and Asia before sparking a major outbreak in French Polynesia in 2013, slipped undetected across the Pacific Ocean into Brazil early in 2014, as established in previous studies. The new work reveals that by that summer, the bug had already hopped unnoticed to Honduras, spreading rapidly to other Central American nations and Mexico—likely by late 2014 and into 2015 [2].
Sequencing Human Genome with Pocket-Sized “Nanopore” Device
Posted on by Dr. Francis Collins

Caption: MinION sequencing device plugged into a laptop/Oxford Nanopore Technologies
It’s hard to believe, but it’s been almost 15 years since we successfully completed the Human Genome Project, ahead of schedule and under budget. I was proud to stand with my international colleagues in a celebration at the Library of Congress on April 14, 2003 (which happens to be my birthday), to announce that we had stitched together the very first reference sequence of the human genome at a total cost of about $400 million. As remarkable as that achievement was, it was just the beginning of our ongoing effort to understand the human genome, and to use that understanding to improve human health.
That first reference human genome was sequenced using automated machines that were the size of small phone booths. Since then, breathtaking progress has been made in developing innovative technologies that have made DNA sequencing far easier, faster, and more affordable. Now, a report in Nature Biotechnology highlights the latest advance: the sequencing and assembly of a human genome using a pocket-sized device [1]. It was generated using several “nanopore” devices that can be purchased online with a “starter kit” for just $1,000. In fact, this new genome sequence—completed in a matter of weeks—includes some notoriously hard-to-sequence stretches of DNA, filling several key gaps in our original reference genome.
Could Zika Virus Have Lasting Impact on Male Fertility?
Posted on by Dr. Francis Collins
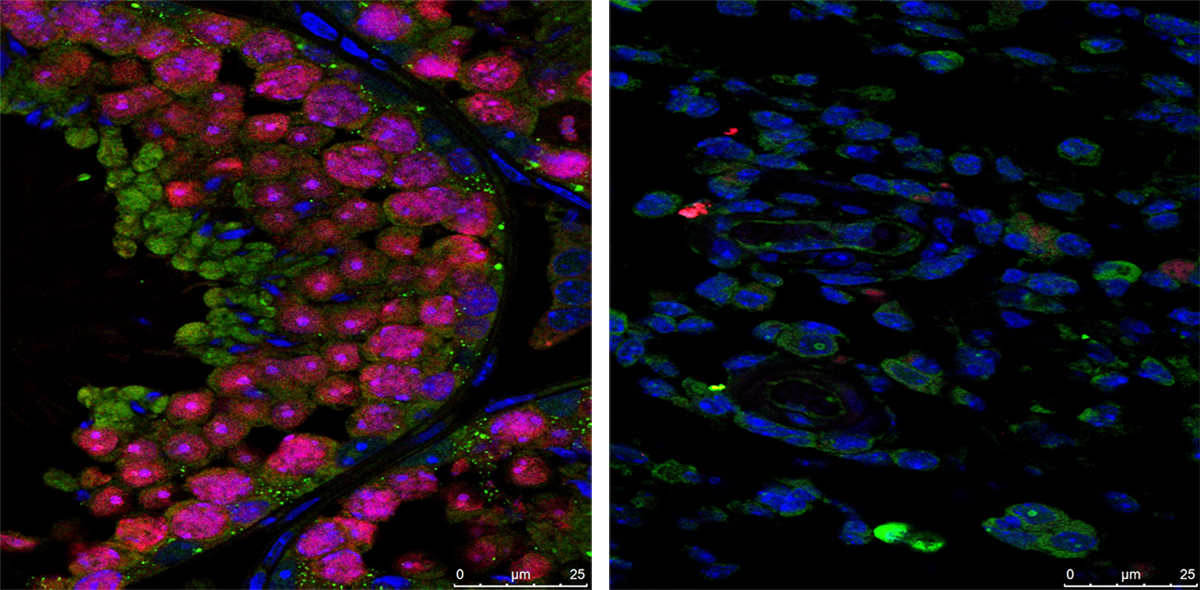
Caption: Immunofluorescence staining showing that the testes of Zika-free mice (left) are full of developing sperm (pink), while the testes of Zika-infected mice (right) contain very few sperm.
Credit: Prabagaran Esakky, Washington University School of Medicine, St. Louis
Recent research has shown that the mosquito-borne Zika virus has the potential to cause serious health problems, including severe birth defects in humans. But the damaging effects of Zika might not end there: results of a new mouse study show that the virus may also have an unexpected negative—and possibly long-lasting—impact on male fertility.
In work published in the journal Nature, an NIH-funded research team found that Zika infections can persist for many weeks in the reproductive systems of male mice [1]. As a result of this infection, levels of testosterone and other sex hormones drop, sperm counts fall, and, in some animals, the testicles shrink to 1/10th of their normal size, possibly irreversibly. All of this adds up to Zika-infected male mice that are significantly less fertile than their healthy counterparts—producing about a quarter as many viable offspring as normal when mated with female mice. While mice are certainly not humans, the results underscore the urgent need for additional research to examine the full spectrum of Zika’s health effects in men, women, and children of both sexes.
Treating Zika Infection: Repurposed Drugs Show Promise
Posted on by Dr. Francis Collins
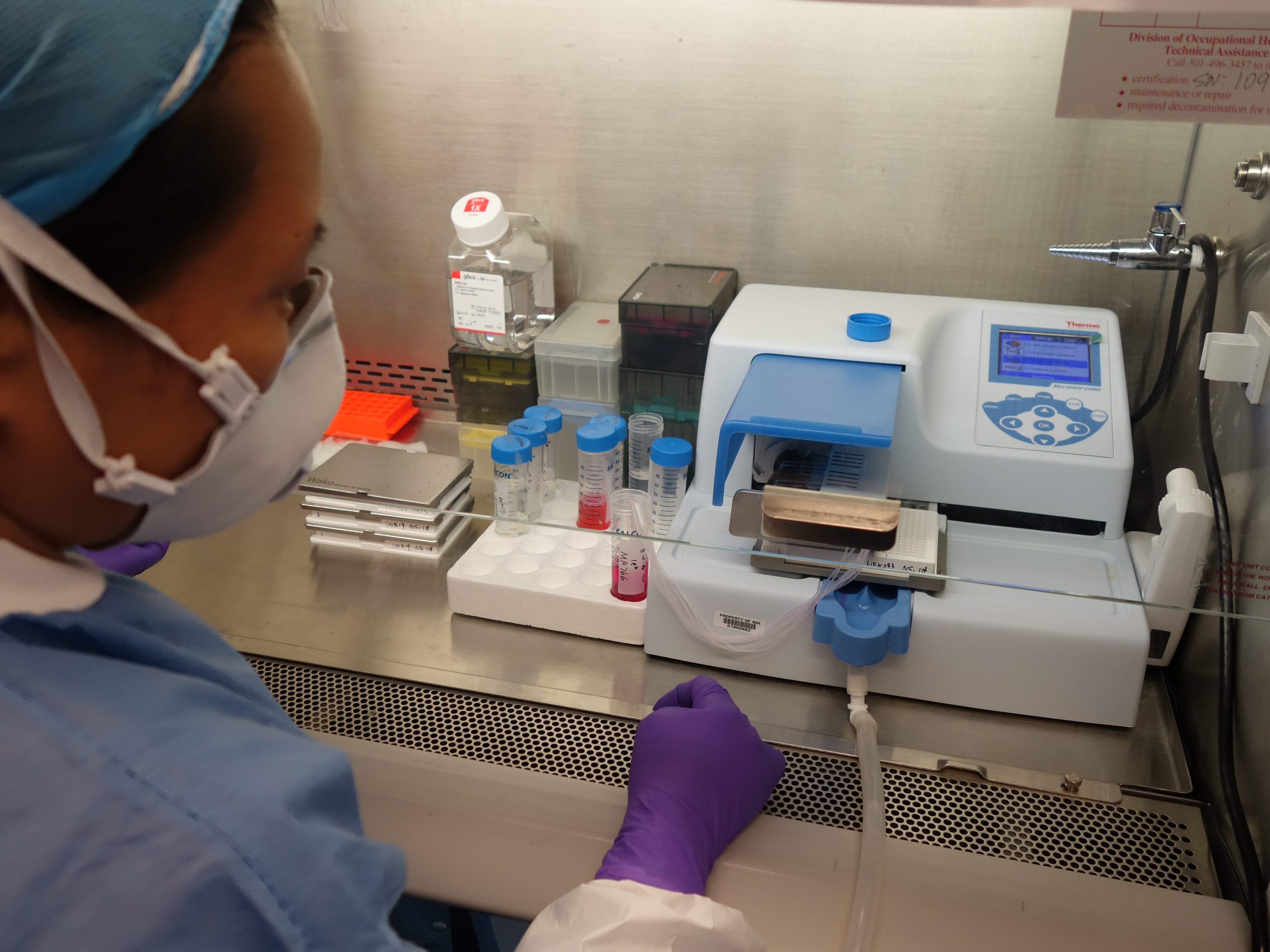
Credit: National Center for Advancing Translational Sciences, NIH
In response to the health threat posed by the recent outbreak of Zika virus in Latin America and its recent spread to Puerto Rico and Florida, researchers have been working at a furious pace to learn more about the mosquito-borne virus. Considerable progress has been made in understanding how Zika might cause babies to be born with unusually small heads and other abnormalities and in developing vaccines that may guard against Zika infection.
Still, there remains an urgent need to find drugs that can be used to treat people already infected with the Zika virus. A team that includes scientists at NIH’s National Center for Advancing Translational Sciences (NCATS) now has some encouraging news on this front. By testing 6,000 FDA-approved drugs and experimental chemical compounds on Zika-infected human cells in the lab, they’ve shown that some existing drugs might be repurposed to fight Zika infection and prevent the virus from harming the developing brain [1]. While additional research is needed, the new findings suggest it may be possible to speed development and approval of new treatments for Zika infection.
Zika Vaccine: Two Candidates Show Promise in Mice
Posted on by Dr. Francis Collins
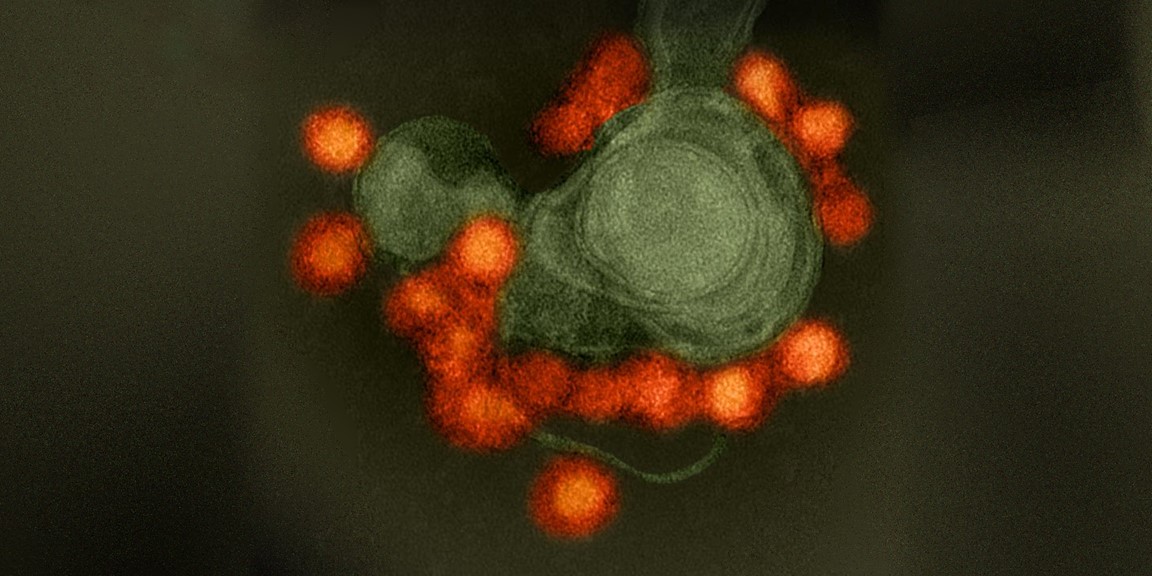
Caption: Zika virus (red), isolated from a microcephaly case in Brazil. The virus is associated with cellular membranes in the center.
Credit: NIAID
Last February, the World Health Organization declared a public health emergency over concerns about very serious birth defects in Brazil and their possible link to Zika virus. But even before then, concerns about the unprecedented spread of Zika virus in Brazil and elsewhere in Latin America had prompted NIH-funded scientists to step up their efforts to combat this emerging infectious disease threat. Over the last year, research aimed at understanding the mosquito-borne virus has progressed rapidly, and we now appear to be getting closer to a Zika vaccine.
In a recent study in the journal Nature, researchers found that a single dose of either of two experimental vaccines completely protected mice against a major viral strain responsible for the Zika outbreak in Brazil [1]. Caution is certainly warranted when extrapolating these (or any other) findings from mice to people. But, taking into account the fact that researchers have already developed safe and effective human vaccines for several related viruses, the new work represents a very encouraging milestone on the road toward a much-needed Zika vaccine for humans.
Snapshots of Life: Portrait of Zika Virus
Posted on by Dr. Francis Collins
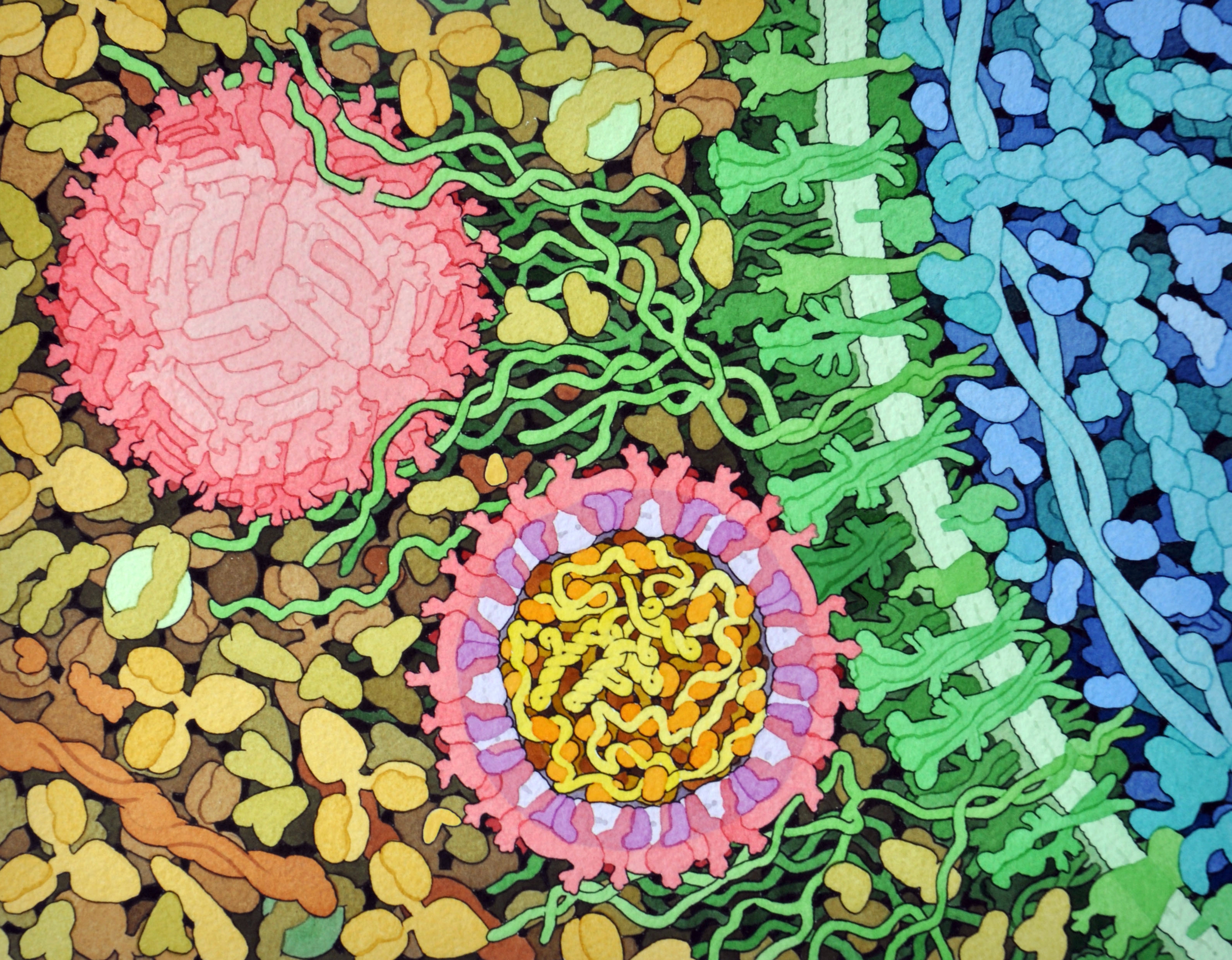
Credit: David Goodsell, The Scripps Research Institute
This lively interplay of shape and color is an artistic rendering of the Zika virus preparing to enter a cell (blue) by binding to its protein receptors (green). The spherical structures (pink) represent two Zika viruses in a blood vessel filled with blood plasma cells (tan). The virus in the middle in cross section shows viral envelope proteins (red) studding the outer surface, with membrane proteins (pink) embedded in a fatty layer of lipids (light purples). In the innermost circle, you can see the viral genome (yellow) coiled around capsid proteins (orange).
This image was sketched and hand-painted with watercolors by David Goodsell, a researcher and illustrator at The Scripps Research Institute, La Jolla, CA. Goodsell put paint and science to paper as part of the “Molecule of the Month” series run by RCSB Protein Data Bank (PDB), which NIH co-supports with the National Science Foundation and the Department of Energy. The PDB, which contains structural data on thousands of proteins and small molecules, uses its “Molecule of the Month” series to help students visualize a molecule or virus and to encourage their exploration of structural biology and its applications to medicine.
Zika and Birth Defects: The Evidence Mounts
Posted on by Dr. Francis Collins

Caption: Human neural progenitor cells (gray) infected with Zika virus (green) increased the enzyme caspase-3 (red), suggesting increased cell death.
Credit: Sarah C. Ogden, Florida State University, Tallahassee
Recently, public health officials have raised major concerns over the disturbing spread of the mosquito-borne Zika virus among people living in and traveling to many parts of Central and South America [1]. While the symptoms of Zika infection are typically mild, grave concerns have arisen about its potential impact during pregnancy. The concerns stem from the unusual number of births of children with microcephaly, a very serious condition characterized by a small head and damaged brain, coinciding with the spread of Zika virus. Now, two new studies strengthen the connection between Zika and an array of birth defects, including, but not limited to, microcephaly.
In the first study, NIH-funded laboratory researchers show that Zika virus can infect and kill human neural progenitor cells [2]. Those progenitor cells give rise to the cerebral cortex, a portion of the brain often affected in children with microcephaly. The second study, involving a small cohort of women diagnosed with Zika virus during their pregnancies in Rio de Janeiro, Brazil, suggests that the attack rate is disturbingly high, and microcephaly is just one of many risks to the developing fetus. [3]