HIV
Immune Resilience is Key to a Long and Healthy Life
Posted on by Lawrence Tabak, D.D.S., Ph.D.

Do you feel as if you or perhaps your family members are constantly coming down with illnesses that drag on longer than they should? Or, maybe you’re one of those lucky people who rarely becomes ill and, if you do, recovers faster than others.
It’s clear that some people generally are more susceptible to infectious illnesses, while others manage to stay healthier or bounce back more quickly, sometimes even into old age. Why is this? A new study from an NIH-supported team has an intriguing answer [1]. The difference, they suggest, may be explained in part by a new measure of immunity they call immune resilience—the ability of the immune system to rapidly launch attacks that defend effectively against infectious invaders and respond appropriately to other types of inflammatory stressors, including aging or other health conditions, and then quickly recover, while keeping potentially damaging inflammation under wraps.
The findings in the journal Nature Communications come from an international team led by Sunil Ahuja, University of Texas Health Science Center and the Department of Veterans Affairs Center for Personalized Medicine, both in San Antonio. To understand the role of immune resilience and its effect on longevity and health outcomes, the researchers looked at multiple other studies including healthy individuals and those with a range of health conditions that challenged their immune systems.
By looking at multiple studies in varied infectious and other contexts, they hoped to find clues as to why some people remain healthier even in the face of varied inflammatory stressors, ranging from mild to more severe. But to understand how immune resilience influences health outcomes, they first needed a way to measure or grade this immune attribute.
The researchers developed two methods for measuring immune resilience. The first metric, a laboratory test called immune health grades (IHGs), is a four-tier grading system that calculates the balance between infection-fighting CD8+ and CD4+ T-cells. IHG-I denotes the best balance tracking the highest level of resilience, and IHG-IV denotes the worst balance tracking the lowest level of immune resilience. An imbalance between the levels of these T cell types is observed in many people as they age, when they get sick, and in people with autoimmune diseases and other conditions.
The researchers also developed a second metric that looks for two patterns of expression of a select set of genes. One pattern associated with survival and the other with death. The survival-associated pattern is primarily related to immune competence, or the immune system’s ability to function swiftly and restore activities that encourage disease resistance. The mortality-associated genes are closely related to inflammation, a process through which the immune system eliminates pathogens and begins the healing process but that also underlies many disease states.
Their studies have shown that high expression of the survival-associated genes and lower expression of mortality-associated genes indicate optimal immune resilience, correlating with a longer lifespan. The opposite pattern indicates poor resilience and a greater risk of premature death. When both sets of genes are either low or high at the same time, immune resilience and mortality risks are more moderate.
In the newly reported study initiated in 2014, Ahuja and his colleagues set out to assess immune resilience in a collection of about 48,500 people, with or without various acute, repetitive, or chronic challenges to their immune systems. In an earlier study, the researchers showed that this novel way to measure immune status and resilience predicted hospitalization and mortality during acute COVID-19 across a wide age spectrum [2].
The investigators have analyzed stored blood samples and publicly available data representing people, many of whom were healthy volunteers, who had enrolled in different studies conducted in Africa, Europe, and North America. Volunteers ranged in age from 9 to 103 years. They also evaluated participants in the Framingham Heart Study, a long-term effort to identify common factors and characteristics that contribute to cardiovascular disease.
To examine people with a wide range of health challenges and associated stresses on their immune systems, the team also included participants who had influenza or COVID-19, and people living with HIV. They also included kidney transplant recipients, people with lifestyle factors that put them at high risk for sexually transmitted infections, and people who’d had sepsis, a condition in which the body has an extreme and life-threatening response following an infection.
The question in all these contexts was the same: How well did the two metrics of immune resilience predict an individual’s health outcomes and lifespan? The short answer is that immune resilience, longevity, and better health outcomes tracked together well. Those with metrics indicating optimal immune resilience generally had better health outcomes and lived longer than those who had lower scores on the immunity grading scale. Indeed, those with optimal immune resilience were more likely to:
- Live longer,
- Resist HIV infection or the progression from HIV to AIDS,
- Resist symptomatic influenza,
- Resist a recurrence of skin cancer after a kidney transplant,
- Survive COVID-19, and
- Survive sepsis.
The study also revealed other interesting findings. While immune resilience generally declines with age, some people maintain higher levels of immune resilience as they get older for reasons that aren’t yet known, according to the researchers. Some people also maintain higher levels of immune resilience despite the presence of inflammatory stress to their immune systems such as during HIV infection or acute COVID-19. People of all ages can show high or low immune resilience. The study also found that higher immune resilience is more common in females than it is in males.
The findings suggest that there is a lot more to learn about why people differ in their ability to preserve optimal immune resilience. With further research, it may be possible to develop treatments or other methods to encourage or restore immune resilience as a way of improving general health, according to the study team.
The researchers suggest it’s possible that one day checkups of a person’s immune resilience could help us to understand and predict an individual’s health status and risk for a wide range of health conditions. It could also help to identify those individuals who may be at a higher risk of poor outcomes when they do get sick and may need more aggressive treatment. Researchers may also consider immune resilience when designing vaccine clinical trials.
A more thorough understanding of immune resilience and discovery of ways to improve it may help to address important health disparities linked to differences in race, ethnicity, geography, and other factors. We know that healthy eating, exercising, and taking precautions to avoid getting sick foster good health and longevity; in the future, perhaps we’ll also consider how our immune resilience measures up and take steps to achieve or maintain a healthier, more balanced, immunity status.
References:
[1] Immune resilience despite inflammatory stress promotes longevity and favorable health outcomes including resistance to infection. Ahuja SK, Manoharan MS, Lee GC, McKinnon LR, Meunier JA, Steri M, Harper N, Fiorillo E, Smith AM, Restrepo MI, Branum AP, Bottomley MJ, Orrù V, Jimenez F, Carrillo A, Pandranki L, Winter CA, Winter LA, Gaitan AA, Moreira AG, Walter EA, Silvestri G, King CL, Zheng YT, Zheng HY, Kimani J, Blake Ball T, Plummer FA, Fowke KR, Harden PN, Wood KJ, Ferris MT, Lund JM, Heise MT, Garrett N, Canady KR, Abdool Karim SS, Little SJ, Gianella S, Smith DM, Letendre S, Richman DD, Cucca F, Trinh H, Sanchez-Reilly S, Hecht JM, Cadena Zuluaga JA, Anzueto A, Pugh JA; South Texas Veterans Health Care System COVID-19 team; Agan BK, Root-Bernstein R, Clark RA, Okulicz JF, He W. Nat Commun. 2023 Jun 13;14(1):3286. doi: 10.1038/s41467-023-38238-6. PMID: 37311745.
[2] Immunologic resilience and COVID-19 survival advantage. Lee GC, Restrepo MI, Harper N, Manoharan MS, Smith AM, Meunier JA, Sanchez-Reilly S, Ehsan A, Branum AP, Winter C, Winter L, Jimenez F, Pandranki L, Carrillo A, Perez GL, Anzueto A, Trinh H, Lee M, Hecht JM, Martinez-Vargas C, Sehgal RT, Cadena J, Walter EA, Oakman K, Benavides R, Pugh JA; South Texas Veterans Health Care System COVID-19 Team; Letendre S, Steri M, Orrù V, Fiorillo E, Cucca F, Moreira AG, Zhang N, Leadbetter E, Agan BK, Richman DD, He W, Clark RA, Okulicz JF, Ahuja SK. J Allergy Clin Immunol. 2021 Nov;148(5):1176-1191. doi: 10.1016/j.jaci.2021.08.021. Epub 2021 Sep 8. PMID: 34508765; PMCID: PMC8425719.
Links:
COVID-19 Research (NIH)
HIV Info (NIH)
Sepsis (National Institute of General Medical Sciences/NIH)
Sunil Ahuja (University of Texas Health Science Center, San Antonio)
Framingham Heart Study (National Heart, Lung, and Blood Institute/NIH)
“A Secret to Health and Long Life? Immune Resilience, NIAID Grantees Report,” NIAID Now Blog, June 13, 2023
NIH Support: National Institute of Allergy and Infectious Diseases; National Institute on Aging; National Institute of Mental Health; National Institute of General Medical Sciences; National Heart, Lung, and Blood Institute
Encouraging First-in-Human Results for a Promising HIV Vaccine
Posted on by Lawrence Tabak, D.D.S., Ph.D.

In recent years, we’ve witnessed some truly inspiring progress in vaccine development. That includes the mRNA vaccines that were so critical during the COVID-19 pandemic, the first approved vaccine for respiratory syncytial virus (RSV), and a “universal flu vaccine” candidate that could one day help to thwart future outbreaks of more novel influenza viruses.
Inspiring progress also continues to be made toward a safe and effective vaccine for HIV, which still infects about 1.5 million people around the world each year [1]. A prime example is the recent first-in-human trial of an HIV vaccine made in the lab from a unique protein nanoparticle, a molecular construct measuring just a few billionths of a meter.
The results of this early phase clinical study, published recently in the journal Science Translational Medicine [2] and earlier in Science [3], showed that the experimental HIV nanoparticle vaccine is safe in people. While this vaccine alone will not offer HIV protection and is intended to be part of an eventual broader, multistep vaccination regimen, the researchers also determined that it elicited a robust immune response in nearly all 36 healthy adult volunteers.
How robust? The results show that the nanoparticle vaccine, known by the lab name eOD-GT8 60-mer, successfully expanded production of a rare type of antibody-producing immune B cell in nearly all recipients.
What makes this rare type of B cell so critical is that it is the cellular precursor of other B cells capable of producing broadly neutralizing antibodies (bnAbs) to protect against diverse HIV variants. Also very good news, the vaccine elicited broad responses from helper T cells. They play a critical supportive role for those essential B cells and their development of the needed broadly neutralizing antibodies.
For decades, researchers have brought a wealth of ideas to bear on developing a safe and effective HIV vaccine. However, crossing the finish line—an FDA-approved vaccine—has proved profoundly difficult.
A major reason is the human immune system is ill equipped to recognize HIV and produce the needed infection-fighting antibodies. And yet the medical literature includes reports of people with HIV who have produced the needed antibodies, showing that our immune system can do it.
But these people remain relatively rare, and the needed robust immunity clocks in only after many years of infection. On top of that, HIV has a habit of mutating rapidly to produce a wide range of identity-altering variants. For a vaccine to work, it most likely will need to induce the production of bnAbs that recognize and defend against not one, but the many different faces of HIV.
To make the uncommon more common became the quest of a research team that includes scientists William Schief, Scripps Research and IAVI Neutralizing Antibody Center, La Jolla, CA; M. Juliana McElrath, Fred Hutchinson Cancer Center, Seattle; and Kristen Cohen, a former member of the McElrath lab now at Moderna, Cambridge, MA. The team, with NIH collaborators and support, has been plotting out a stepwise approach to train the immune system into making the needed bnAbs that recognize many HIV variants.
The critical first step is to prime the immune system to make more of those coveted bnAb-precursor B cells. That’s where the protein nanoparticle known as eOD-GT8 60-mer enters the picture.
This nanoparticle, administered by injection, is designed to mimic a small, highly conserved segment of an HIV protein that allows the virus to bind and infect human cells. In the body, those nanoparticles launch an immune response and then quickly vanish. But because this important protein target for HIV vaccines is so tiny, its signal needed amplification for immune system detection.
To boost the signal, the researchers started with a bacterial protein called lumazine synthase (LumSyn). It forms the scaffold, or structural support, of the self-assembling nanoparticle. Then, they added to the LumSyn scaffold 60 copies of the key HIV protein. This louder HIV signal is tailored to draw out and engage those very specific B cells with the potential to produce bnAbs.
As the first-in-human study showed, the nanoparticle vaccine was safe when administered twice to each participant eight weeks apart. People reported only mild to moderate side effects that went away in a day or two. The vaccine also boosted production of the desired B cells in all but one vaccine recipient (35 of 36). The idea is that this increase in essential B cells sets the stage for the needed additional steps—booster shots that can further coax these cells along toward making HIV protective bnAbs.
The latest finding in Science Translational Medicine looked deeper into the response of helper T cells in the same trial volunteers. Again, the results appear very encouraging. The researchers observed CD4 T cells specific to the HIV protein and to the LumSyn in 84 percent and 93 percent of vaccine recipients. Their analyses also identified key hotspots that the T cells recognized, which is important information for refining future vaccines to elicit helper T cells.
The team reports that they’re now collaborating with Moderna, the developer of one of the two successful mRNA-based COVID-19 vaccines, on an mRNA version of eOD-GT8 60-mer. That’s exciting because mRNA vaccines are much faster and easier to produce and modify, which should now help to move this line of research along at a faster clip.
Indeed, two International AIDS Vaccine Initiative (IAVI)-sponsored clinical trials of the mRNA version are already underway, one in the U.S. and the other in Rwanda and South Africa [4]. It looks like this team and others are now on a promising track toward following the basic science and developing a multistep HIV vaccination regimen that guides the immune response and its stepwise phases in the right directions.
As we look back on more than 40 years of HIV research, it’s heartening to witness the progress that continues toward ending the HIV epidemic. This includes the recent FDA approval of the drug Apretude, the first injectable treatment option for pre-exposure prevention of HIV, and the continued global commitment to produce a safe and effective vaccine.
References:
[1] Global HIV & AIDS statistics fact sheet. UNAIDS.
[2] A first-in-human germline-targeting HIV nanoparticle vaccine induced broad and publicly targeted helper T cell responses. Cohen KW, De Rosa SC, Fulp WJ, deCamp AC, Fiore-Gartland A, Laufer DS, Koup RA, McDermott AB, Schief WR, McElrath MJ. Sci Transl Med. 2023 May 24;15(697):eadf3309.
[3] Vaccination induces HIV broadly neutralizing antibody precursors in humans. Leggat DJ, Cohen KW, Willis JR, Fulp WJ, deCamp AC, Koup RA, Laufer DS, McElrath MJ, McDermott AB, Schief WR. Science. 2022 Dec 2;378(6623):eadd6502.
[4] IAVI and Moderna launch first-in-Africa clinical trial of mRNA HIV vaccine development program. IAVI. May 18, 2022.
Links:
Progress Toward an Eventual HIV Vaccine, NIH Research Matters, Dec. 13, 2022.
NIH Statement on HIV Vaccine Awareness Day 2023, Auchincloss H, Kapogiannis, B. May, 18, 2023.
HIV Vaccine Development (National Institute of Allergy and Infectious Diseases/NIH)
International AIDS Vaccine Initiative (IAVI) (New York, NY)
William Schief (Scripps Research, La Jolla, CA)
Julie McElrath (Fred Hutchinson Cancer Center, Seattle, WA)
McElrath Lab (Fred Hutchinson Cancer Center, Seattle, WA)
NIH Support: National Institute of Allergy and Infectious Diseases
Thank You, Dr. Fauci
Posted on by Lawrence Tabak, D.D.S., Ph.D.

This Is Why NIH Invests in Global Health Research
Posted on by Roger I. Glass, M.D., Ph.D., Fogarty International Center

Efforts over the past few years to end the COVID-19 pandemic clearly reveal how global health impacts individual wellbeing and national security. At NIH, the Fogarty International Center helps the other institutes become engaged with global health research, which investigates the dual burden of infectious disease and non-communicable disease.
Global health research also encompasses data science, economics, genetics, climate change science, and many other disciplines. For more than 50 years, Fogarty has been building partnerships among institutions in the U.S. and abroad, while training the next generation of scientists focused on universal health needs.
America’s investment in Fogarty has paid rich dividends
During the pandemic, in particular, we’ve seen researchers trained by our programs make scientific discoveries that contributed to international security. Take Jessica Manning, a former Fogarty fellow who now conducts malaria research in Phnom Penh, Cambodia. Her team at the Ministry of Health sequenced the viral strain of SARS-CoV-2, the cause of COVID-19, infecting the first Cambodian patient and documented early the spread of this novel coronavirus outside of China.
Similarly, Christian Happi, director of the African Centre of Excellence for the Genomics of Infectious Disease, Ede, Nigeria, sequenced the first SARS-CoV-2 genome in Africa. Happi was able to do it by adapting the sequencing and analytical pipelines that he’d created back when he was a Fogarty grantee studying Ebola.
In Botswana, Sikhulile Moyo leveraged the skills he’d acquired while supported by a Fogarty HIV research training grant with Max Essex, Harvard School of Public Health, Cambridge, MA, to track COVID-19 mutations for his country’s Ministry of Health. Last November, he alerted the world of a new Omicron variant. Within six weeks, Omicron became the dominant global strain, challenging the ability of COVID vaccines to control its spread. In the Dominican Republic, William Duke, a national commission member, used what he’d learned as a Fogarty trainee to help create a national COVID-19 intervention plan to prevent and control the disease.
Fogarty’s fostering of global health leaders is one way we advance scientific expertise while ensuring our nation’s biosecurity. Another is by finding effective ways to study abroad the same health conditions that affect our own population.
Research conducted in Colombia, for example, may provide clues for preventing Alzheimer’s disease in the U.S. Fogarty support brought together neuroscientists Kenneth Kosik, University of California, Santa Barbara, and Francisco Lopera, University of Antioquia, Colombia, to study members of the largest-known family with an early-onset, rapidly progressive form of the disease. Over the years, Kosik and Lopera have trained local scientists, explored gene therapy targets, investigated biomarkers to monitor disease progression, and conducted drug trials in search of a cure for Alzheimer’s.
Researchers in other fields also discover unique opportunities to investigate populations with high rates of disease. Siana Nkya, a Fogarty grantee based in Tanzania, has devoted her career to studying the genetic determinants of sickle cell disease, which affects many people around the world, including in the U.S. We hope that US-African partnerships might develop improved, affordable treatments and a cure for all patients with this devastating disease. Similarly, people in the U.S. have access to state-of-the-art HIV treatment studies in places around the globe where incidence rates are higher.
Fogarty has supported many milestone achievements in HIV research over the years. Among them is a study that took place in nine countries. The research, led by Myron Cohen of the University of North Carolina at Chapel Hill, established that antiretroviral therapy can prevent sexual transmission of HIV-1 among couples in which one person is infected and the other is not. In fact, this research informs current HIV treatment recommendations worldwide, including in the U.S.
Americans will also undoubtedly benefit from projects funded by Fogarty’s Global Brain and Nervous System Disorders Research across the Lifespan program. For example, psychologist Tatiana Balachova, University of Oklahoma, Oklahoma City, has designed an intervention for women in Russia to prevent fetal alcohol spectrum disorders. In another project in South Africa, Sandra and Joseph Jacobson, Wayne State University, Detroit, conducted the first-ever prospective longitudinal study of the syndrome. Findings from both projects are ripe for translation within an American context.
Other examples of Global Brain program investigations with broad implications in our own country include studying early psychosis in China; capacity building for schizophrenia research in Macedonia; exploring family consequences from the Zika virus in Brazil; and studying dementia and related health and social challenges in Lebanon.
These are just a few examples of Fogarty’s work and its unique mission. What is most remarkable about Fogarty is that just under 90 percent of our grants are co-funded by at least one other NIH institute, center, or office. Collaboration, both within borders and across them, is Fogarty’s formula for success.
Links:
Fogarty International Center (NIH)
Overview of Brain Disorders: Research Across the Lifespan (Fogarty)
Former Fogarty Scholar Dr Jessica Manning Helps Cambodia Respond to COVID (Fogarty)
Christian Happi: Former Fogarty Grantee Leads COVID-19 Genomics Work in Africa (Fogarty)
Sikhulile Moyo: Fogarty Fellow Recognized for Omicron Discovery (Fogarty)
William Duke: Former Fogarty HIV Trainee Helps Lead Dominican Republic’s COVID Response (Fogarty)
Kenneth Kosic and Francisco Lopera: NIH Support Spurs Alzheimer’s Research in Colombia (Fogarty)
Former Fogarty fellow Siana Nkya Tackles Sickle Cell Disease in Tanzania (Fogarty)
Tatiana Balachova: Researchers Tackle Fetal Alcohol Syndrome in Russia (Fogarty)
Sandra and Joseph Jacobson: Fetal Alcohol Exposure Research Supported by NIAAA in South Africa, Ukraine and Russia Improves Prevention, Outcomes (Fogarty)
Note: Dr. Lawrence Tabak, who performs the duties of the NIH Director, has asked the heads of NIH’s Institutes and Centers (ICs) to contribute occasional guest posts to the blog to highlight some of the interesting science that they support and conduct. This is the 22nd in the series of NIH IC guest posts that will run until a new permanent NIH director is in place.
Finding HIV’s ‘Sweet Spot’
Posted on by Lawrence Tabak, D.D.S., Ph.D.
Each year, about 30,000 people in the United States contract the human immunodeficiency virus (HIV), the cause of AIDS [1]. Thankfully, most can control their HIV infections with antiretroviral therapy and will lead productive, high-quality lives. Many will even reach a point where they have no detectable levels of virus circulating in their blood. However, all must still worry that the undetectable latent virus hidden in their systems could one day reactivate and lead to a range of serious health complications.
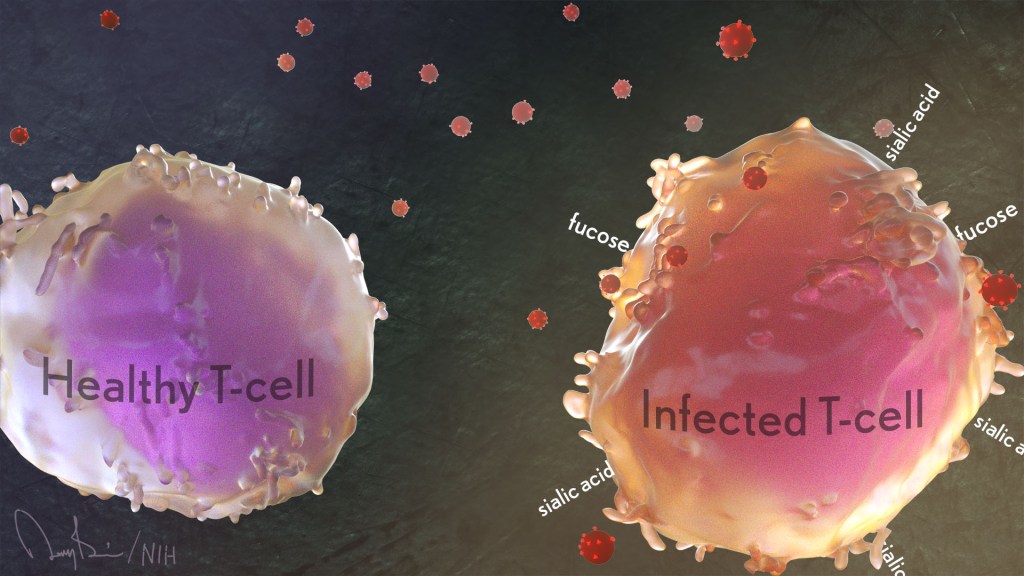
Now, an NIH-funded team has found that patterns of sugars at the surface of our own human immune cells affect their vulnerability to HIV infection. These data suggest it may be possible to find the infected immune cells harboring the last vestiges of virus by reading the sugar profiles on their surfaces. If so, it would move us a step closer to eliminating latent HIV infection and ultimately finding a cure for this horrible virus.
These fascinating new findings come from a team led by Nadia Roan, Gladstone Institutes, San Francisco and Mohamed Abdel-Mohsen, The Wistar Institute, Philadelphia, PA. Among its many areas of study, the Roan lab is interested in why HIV favors infecting specific subsets of a special type of immune cell called memory CD4 T cells. These cells come in different varieties. They also play important roles in the immune system’s ability to recall past infections and launch a rapid response to an emerging repeat infection.
For years, her team and others have tried to understand the interplay between HIV and human immune cells primarily by studying the proteins present at the cell surface. But living cells and their proteins also are coated in sugars and, the presence or absence of these carbohydrates is essential to their biochemistry.
In the new study, published in the journal eLife, the researchers included for the first time the patterns of these sugars in their study of cell surface proteins [2]. They, like many labs, hadn’t done so previously for technical reasons: it’s much easier to track these proteins than sugars.
To overcome this technical hurdle, Roan’s team turned to an approach that it uses for quantifying levels of proteins on the surface of single cells. The method, called CyTOF, uses metal-studded antibodies that stick to proteins, uniquely marking precise patterns of selected proteins, in this case, on individual HIV-infected cells.
In collaboration with Abdel-Mohsen, a glycobiology expert, they adapted this method for cell surface sugars. They did it by adding molecules called lectins, which stick to sugar molecules with specific shapes and compositions.
With this innovation, Roan and team report that they learned to characterize and quantify levels of 34 different proteins on the cell surface simultaneously with five types of sugars. Their next questions were: Could those patterns of cell-surface sugars help them differentiate between different types of immune cells? If so, might those patterns help to define a cell’s susceptibility to HIV?
The answer appears to be yes to both questions. Their studies revealed tremendous diversity in the patterns of sugars at the cells surfaces. Those patterns varied depending on a cell’s tissue of origin—in this case, from blood, tonsil, or the reproductive tract. The patterns also varied depending on the immune cell type—memory CD4 T cells versus other T cells or antibody-producing B cells.
Those sugar and protein profiles offered important clues as to which cells HIV prefers to infect. More specifically, compared to uninfected memory CD4 T cells, the infected ones had higher surface levels of two sugars, known as fucose [3] and sialic acid [4]. What’s more, during HIV infection, levels of both sugars increased.
Scientists already knew that HIV changes the proteins that the infected memory CD4 T cell puts on its surface, a process known as viral remodeling. Now it appears that something similar happens with sugars, too. The new findings suggest the virus increases levels of sialic acid at the cell surface in ways that may help the virus to survive. That’s especially intriguing because sialic acid also is associated with a cell’s ability to avoid detection by the immune system.
The Roan and Abdel-Mohsen labs now plan to team up again to apply their new method to study latent infection. They want to find sugar-based patterns that define those lingering infected cells and see if it’s possible to target them and eliminate the lingering HIV.
What’s also cool is this study indicates that by performing single-cell analyses and sorting cells based on their sugar and protein profiles, it may be possible to discover distinct new classes of immune and other cells that have eluded earlier studies. As was the case with HIV, this broader protein-sugar profile could hold the key to gaining deeper insights into disease processes throughout the body.
References:
[1] Diagnoses of HIV infection in the United States and dependent areas, 2020. HIV Surveillance Report, May 2020; 33; Centers for Disease Control and Prevention.
[2] Single-cell glycomics analysis by CyTOF-Lec reveals glycan features defining cells differentially susceptible to HIV. Ma T, McGregor M, Giron L, Xie G, George AF, Abdel-Mohsen M, Roan NR.eLife 2022 July 5;11:e78870
[3] Biological functions of fucose in mammals. Schneider M, Al-Shareffi E, Haltiwanger RS. Glycobiology. 2016 Jun;26(6):543.
[4] Sialic acids and other nonulosonic acids. Lewis AL, Chen X, Schnaar RL, Varki A. In Essentials of Glycobiology [Internet]. 4th edition. Cold Spring Harbor (NY): Cold Spring Harbor Laboratory Press; 2022.
Links:
HIV/AIDS (National Institute of Allergy and Infectious Diseases/NIH)
Roan Lab (University of California, San Francisco)
Mohamed Abdel-Mohsen (The Wistar Institute, Philadelphia, PA)
NIH Support: National Institute of Allergy and Infectious Diseases; National Institute of Diabetes and Digestive and Kidney Diseases; National Institute on Aging; National Institute of Neurological Disorders and Stroke
What A Year It Was for Science Advances!
Posted on by Dr. Francis Collins
At the close of every year, editors and writers at the journal Science review the progress that’s been made in all fields of science—from anthropology to zoology—to select the biggest advance of the past 12 months. In most cases, this Breakthrough of the Year is as tough to predict as the Oscar for Best Picture. Not in 2020. In a year filled with a multitude of challenges posed by the emergence of the deadly coronavirus disease 2019 (COVID-2019), the breakthrough was the development of the first vaccines to protect against this pandemic that’s already claimed the lives of more than 360,000 Americans.
In keeping with its annual tradition, Science also selected nine runner-up breakthroughs. This impressive list includes at least three areas that involved efforts supported by NIH: therapeutic applications of gene editing, basic research understanding HIV, and scientists speaking up for diversity. Here’s a quick rundown of all the pioneering advances in biomedical research, both NIH and non-NIH funded:
Shots of Hope. A lot of things happened in 2020 that were unprecedented. At the top of the list was the rapid development of COVID-19 vaccines. Public and private researchers accomplished in 10 months what normally takes about 8 years to produce two vaccines for public use, with more on the way in 2021. In my more than 25 years at NIH, I’ve never encountered such a willingness among researchers to set aside their other concerns and gather around the same table to get the job done fast, safely, and efficiently for the world.
It’s also pretty amazing that the first two conditionally approved vaccines from Pfizer and Moderna were found to be more than 90 percent effective at protecting people from infection with SARS-CoV-2, the coronavirus that causes COVID-19. Both are innovative messenger RNA (mRNA) vaccines, a new approach to vaccination.
For this type of vaccine, the centerpiece is a small, non-infectious snippet of mRNA that encodes the instructions to make the spike protein that crowns the outer surface of SARS-CoV-2. When the mRNA is injected into a shoulder muscle, cells there will follow the encoded instructions and temporarily make copies of this signature viral protein. As the immune system detects these copies, it spurs the production of antibodies and helps the body remember how to fend off SARS-CoV-2 should the real thing be encountered.
It also can’t be understated that both mRNA vaccines—one developed by Pfizer and the other by Moderna in conjunction with NIH’s National Institute of Allergy and Infectious Diseases—were rigorously evaluated in clinical trials. Detailed data were posted online and discussed in all-day meetings of an FDA Advisory Committee, open to the public. In fact, given the high stakes, the level of review probably was more scientifically rigorous than ever.
First CRISPR Cures: One of the most promising areas of research now underway involves gene editing. These tools, still relatively new, hold the potential to fix gene misspellings—and potentially cure—a wide range of genetic diseases that were once to be out of reach. Much of the research focus has centered on CRISPR/Cas9. This highly precise gene-editing system relies on guide RNA molecules to direct a scissor-like Cas9 enzyme to just the right spot in the genome to cut out or correct a disease-causing misspelling.
In late 2020, a team of researchers in the United States and Europe succeeded for the first time in using CRISPR to treat 10 people with sickle cell disease and transfusion-dependent beta thalassemia. As published in the New England Journal of Medicine, several months after this non-heritable treatment, all patients no longer needed frequent blood transfusions and are living pain free [1].
The researchers tested a one-time treatment in which they removed bone marrow from each patient, modified the blood-forming hematopoietic stem cells outside the body using CRISPR, and then reinfused them into the body. To prepare for receiving the corrected cells, patients were given toxic bone marrow ablation therapy, in order to make room for the corrected cells. The result: the modified stem cells were reprogrammed to switch back to making ample amounts of a healthy form of hemoglobin that their bodies produced in the womb. While the treatment is still risky, complex, and prohibitively expensive, this work is an impressive start for more breakthroughs to come using gene editing technologies. NIH, including its Somatic Cell Genome Editing program, continues to push the technology to accelerate progress and make gene editing cures for many disorders simpler and less toxic.
Scientists Speak Up for Diversity: The year 2020 will be remembered not only for COVID-19, but also for the very public and inescapable evidence of the persistence of racial discrimination in the United States. Triggered by the killing of George Floyd and other similar events, Americans were forced to come to grips with the fact that our society does not provide equal opportunity and justice for all. And that applies to the scientific community as well.
Science thrives in safe, diverse, and inclusive research environments. It suffers when racism and bigotry find a home to stifle diversity—and community for all—in the sciences. For the nation’s leading science institutions, there is a place and a calling to encourage diversity in the scientific workplace and provide the resources to let it flourish to everyone’s benefit.
For those of us at NIH, last year’s peaceful protests and hashtags were noticed and taken to heart. That’s one of the many reasons why we will continue to strengthen our commitment to building a culturally diverse, inclusive workplace. For example, we have established the NIH Equity Committee. It allows for the systematic tracking and evaluation of diversity and inclusion metrics for the intramural research program for each NIH institute and center. There is also the recently founded Distinguished Scholars Program, which aims to increase the diversity of tenure track investigators at NIH. Recently, NIH also announced that it will provide support to institutions to recruit diverse groups or “cohorts” of early-stage research faculty and prepare them to thrive as NIH-funded researchers.
AI Disentangles Protein Folding: Proteins, which are the workhorses of the cell, are made up of long, interconnected strings of amino acids that fold into a wide variety of 3D shapes. Understanding the precise shape of a protein facilitates efforts to figure out its function, its potential role in a disease, and even how to target it with therapies. To gain such understanding, researchers often try to predict a protein’s precise 3D chemical structure using basic principles of physics—including quantum mechanics. But while nature does this in real time zillions of times a day, computational approaches have not been able to do this—until now.
Of the roughly 170,000 proteins mapped so far, most have had their structures deciphered using powerful imaging techniques such as x-ray crystallography and cryo–electron microscopy (cryo-EM). But researchers estimate that there are at least 200 million proteins in nature, and, as amazing as these imaging techniques are, they are laborious, and it can take many months or years to solve 3D structure of a single protein. So, a breakthrough certainly was needed!
In 2020, researchers with the company Deep Mind, London, developed an artificial intelligence (AI) program that rapidly predicts most protein structures as accurately as x-ray crystallography and cryo-EM can map them [2]. The AI program, called AlphaFold, predicts a protein’s structure by computationally modeling the amino acid interactions that govern its 3D shape.
Getting there wasn’t easy. While a complete de novo calculation of protein structure still seemed out of reach, investigators reasoned that they could kick start the modeling if known structures were provided as a training set to the AI program. Utilizing a computer network built around 128 machine learning processors, the AlphaFold system was created by first focusing on the 170,000 proteins with known structures in a reiterative process called deep learning. The process, which is inspired by the way neural networks in the human brain process information, enables computers to look for patterns in large collections of data. In this case, AlphaFold learned to predict the underlying physical structure of a protein within a matter of days. This breakthrough has the potential to accelerate the fields of structural biology and protein research, fueling progress throughout the sciences.
How Elite Controllers Keep HIV at Bay: The term “elite controller” might make some people think of video game whizzes. But here, it refers to the less than 1 percent of people living with human immunodeficiency virus (HIV) who’ve somehow stayed healthy for years without taking antiretroviral drugs. In 2020, a team of NIH-supported researchers figured out why this is so.
In a study of 64 elite controllers, published in the journal Nature, the team discovered a link between their good health and where the virus has inserted itself in their genomes [3]. When a cell transcribes a gene where HIV has settled, this so-called “provirus,” can produce more virus to infect other cells. But if it settles in a part of a chromosome that rarely gets transcribed, sometimes called a gene desert, the provirus is stuck with no way to replicate. Although this discovery won’t cure HIV/AIDS, it points to a new direction for developing better treatment strategies.
In closing, 2020 presented more than its share of personal and social challenges. Among those challenges was a flood of misinformation about COVID-19 that confused and divided many communities and even families. That’s why the editors and writers at Science singled out “a second pandemic of misinformation” as its Breakdown of the Year. This divisiveness should concern all of us greatly, as COVID-19 cases continue to soar around the country and our healthcare gets stretched to the breaking point. I hope and pray that we will all find a way to come together, both in science and in society, as we move forward in 2021.
References:
[1] CRISPR-Cas9 gene editing for sickle cell disease and β-thalassemia. Frangoul H et al. N Engl J Med. 2020 Dec 5.
[2] ‘The game has changed.’ AI triumphs at protein folding. Service RF. Science. 04 Dec 2020.
[3] Distinct viral reservoirs in individuals with spontaneous control of HIV-1. Jiang C et al. Nature. 2020 Sep;585(7824):261-267.
Links:
COVID-19 Research (NIH)
2020 Science Breakthrough of the Year (American Association for the Advancement of Science, Washington, D.C)
See the Human Cardiovascular System in a Whole New Way
Posted on by Dr. Francis Collins
Watch this brief video and you might guess you’re seeing an animated line drawing, gradually revealing a delicate take on a familiar system: the internal structures of the human body. But this movie doesn’t capture the work of a talented sketch artist. It was created using the first 3D, full-body imaging device using positron emission tomography (PET).
The device is called an EXPLORER (EXtreme Performance LOng axial REsearch scanneR) total-body PET scanner. By pairing this scanner with an advanced method for reconstructing images from vast quantities of data, the researchers can make movies.
For this movie in particular, the researchers injected small amounts of a short-lived radioactive tracer—an essential component of all PET scans—into the lower leg of a study volunteer. They then sat back as the scanner captured images of the tracer moving up the leg and into the body, where it enters the heart. The tracer moves through the heart’s right ventricle to the lungs, back through the left ventricle, and up to the brain. Keep watching, and, near the 30-second mark, you will see in closer focus a haunting capture of the beating heart.
This groundbreaking scanner was developed and tested by Jinyi Qi, Simon Cherry, Ramsey Badawi, and their colleagues at the University of California, Davis [1]. As the NIH-funded researchers reported recently in Proceedings of the National Academy of Sciences, their new scanner can capture dynamic changes in the body that take place in a tenth of a second [2]. That’s faster than the blink of an eye!
This movie is composed of frames captured at 0.1-second intervals. It highlights a feature that makes this scanner so unique: its ability to visualize the whole body at once. Other medical imaging methods, including MRI, CT, and traditional PET scans, can be used to capture beautiful images of the heart or the brain, for example. But they can’t show what’s happening in the heart and brain at the same time.
The ability to capture the dynamics of radioactive tracers in multiple organs at once opens a new window into human biology. For example, the EXPLORER system makes it possible to measure inflammation that occurs in many parts of the body after a heart attack, as well as to study interactions between the brain and gut in Parkinson’s disease and other disorders.
EXPLORER also offers other advantages. It’s extra sensitive, which enables it to capture images other scanners would miss—and with a lower dose of radiation. It’s also much faster than a regular PET scanner, making it especially useful for imaging wiggly kids. And it expands the realm of research possibilities for PET imaging studies. For instance, researchers might repeatedly image a person with arthritis over time to observe changes that may be related to treatments or exercise.
Currently, the UC Davis team is working with colleagues at the University of California, San Francisco to use EXPLORER to enhance our understanding of HIV infection. Their preliminary findings show that the scanner makes it easier to capture where the human immunodeficiency virus (HIV), the cause of AIDS, is lurking in the body by picking up on signals too weak to be seen on traditional PET scans.
While the research potential for this scanner is clearly vast, it also holds promise for clinical use. In fact, a commercial version of the scanner, called uEXPLORER, has been approved by the FDA and is in use at UC Davis [3]. The researchers have found that its improved sensitivity makes it much easier to detect cancers in patients who are obese and, therefore, harder to image well using traditional PET scanners.
As soon as the COVID-19 outbreak subsides enough to allow clinical research to resume, the researchers say they’ll begin recruiting patients with cancer into a clinical study designed to compare traditional PET and EXPLORER scans directly.
As these researchers, and other researchers around the world, begin to put this new scanner to use, we can look forward to seeing many more remarkable movies like this one. Imagine what they will reveal!
References:
[1] First human imaging studies with the EXPLORER total-body PET scanner. Badawi RD, Shi H, Hu P, Chen S, Xu T, Price PM, Ding Y, Spencer BA, Nardo L, Liu W, Bao J, Jones T, Li H, Cherry SR. J Nucl Med. 2019 Mar;60(3):299-303.
[2] Subsecond total-body imaging using ultrasensitive positron emission tomography. Zhang X, Cherry SR, Xie Z, Shi H, Badawi RD, Qi J. Proc Natl Acad Sci U S A. 2020 Feb 4;117(5):2265-2267.
[3] “United Imaging Healthcare uEXPLORER Total-body Scanner Cleared by FDA, Available in U.S. Early 2019.” Cision PR Newswire. January 22, 2019.
Links:
Positron Emission Tomography (PET) (NIH Clinical Center)
EXPLORER Total-Body PET Scanner (University of California, Davis)
Cherry Lab (UC Davis)
Badawi Lab (UC Davis Medical Center, Sacramento)
NIH Support: National Cancer Institute; National Institute of Biomedical Imaging and Bioengineering; Common Fund
Exploring Drug Repurposing for COVID-19 Treatment
Posted on by Dr. Francis Collins

It usually takes more than a decade to develop a safe, effective anti-viral therapy. But, when it comes to coronavirus disease 2019 (COVID-19), we don’t have that kind of time. One way to speed the process may be to put some old drugs to work against this new disease threat. This is generally referred to as “drug repurposing.”
NIH has been doing everything possible to encourage screens of existing drugs that have been shown safe for human use. In a recent NIH-funded study in the journal Nature, researchers screened a chemical “library” that contained nearly 12,000 existing drug compounds for their potential activity against SARS-CoV-2, the novel coronavirus that causes COVID-19 [1]. The results? In tests in both non-human primate and human cell lines grown in laboratory conditions, 21 of these existing drugs showed potential for repurposing to thwart the novel coronavirus—13 of them at doses that likely could be safely given to people. The majority of these drugs have been tested in clinical trials for use in HIV, autoimmune diseases, osteoporosis, and other conditions.
These latest findings come from an international team led by Sumit Chanda, Sanford Burnham Prebys Medical Discovery Institute, La Jolla, CA. The researchers took advantage of a small-molecule drug library called ReFRAME [2], which was created in 2018 by Calibr, a non-profit drug discovery division of Scripps Research, La Jolla, CA.
In collaboration with Yuen Kwok-Yung’s team at the University of Hong Kong, the researchers first developed a high-throughput method that enabled them to screen rapidly each of the 11,987 drug compounds in the ReFRAME library for their potential to block SARS-CoV-2 in cells grown in the lab. The first round of testing narrowed the list of possible COVID-19 drugs to about 300. Next, using lower concentrations of the drugs in cells exposed to a second strain of SARS-CoV-2, they further narrowed the list to 100 compounds that could reliably limit growth of the coronavirus by at least 40 percent.
Generally speaking, an effective anti-viral drug is expected to show greater activity as its concentration is increased. So, Chanda’s team then tested those 100 drugs for evidence of such a dose-response relationship. Twenty-one of them passed this test. This group included remdesivir, a drug originally developed for Ebola virus disease and recently authorized by the U.S. Food and Drug Administration (FDA) for emergency use in the treatment of COVID-19. Remdesivir could now be considered a positive control.
These findings raised another intriguing question: Could any of the other drugs with a dose-response relationship work well in combination with remdesivir to block SARS-CoV-2 infection? Indeed, the researchers found that four of them could.
Further study showed that some of the most promising drugs on the list reduced the number of SARS-CoV-2 infected cells by 65 to 85 percent. The most potent of these was apilimod, a drug that has been evaluated in clinical trials for treating Crohn’s disease, rheumatoid arthritis, and other autoimmune conditions. Apilimod is now being evaluated in the clinic for its ability to prevent the progression of COVID-19. Another potential antiviral to emerge from the study is clofazimine, a 70-year old FDA-approved drug that is on the World Health Organization’s list of essential medicines for the treatment of leprosy.
Overall, the findings suggest that there may be quite a few existing drugs and/or experimental drugs fairly far along in the development pipeline that have potential to be repurposed for treating COVID-19. What’s more, some of them might also work well in combination with remdesivir, or perhaps other drugs, as treatment “cocktails,” such as those used to successfully treat HIV and hepatitis C.
This is just one of a wide variety of drug screening efforts that are underway, using different libraries and different assays to detect activity against SARS-CoV-2. The NIH’s National Center for Advancing Translational Sciences has established an open data portal to collect all of these data as quickly and openly as possible. As NIH continues its efforts to use the power of science to end the COVID-19 pandemic, it is critically important that we explore as many avenues as possible for developing diagnostics, treatments, and vaccines.
References:
[1] Discovery of SARS-CoV-2 antiviral drugs through large-scale compound repurposing. Riva L, Yuan S, Yin X, et al. Nature. 2020 Jul 24 [published online ahead of print]
[2] The ReFRAME library as a comprehensive drug repurposing library and its application to the treatment of cryptosporidiosis. Janes J, Young ME, Chen E, et al. Proc Natl Acad Sci USA. 2018;115(42):10750-10755.
Links:
Coronavirus (COVID-19) (NIH)
ReFRAMEdb (Scripps Research, La Jolla, CA)
The Chanda Lab (Sanford Burnham Prebys Medical Discovery Institute, La Jolla, CA)
Yuen Kwok-Yung (University of Hong Kong)
OpenData|Covid-19 (National Center for Advancing Translational Sciences/NIH)
NIH Support: National Institute of Allergy and Infectious Diseases; National Institute of General Medical Sciences
Finding Antibodies that Neutralize SARS-CoV-2
Posted on by Dr. Francis Collins

It’s now clear that nearly everyone who recovers from coronavirus disease 2019 (COVID-19) produces antibodies that specifically target SARS-CoV-2, the novel coronavirus that causes the infection. Yet many critical questions remain. A major one is: just how well do those particular antibodies neutralize the virus to fight off the infection and help someone recover from COVID-19? Fortunately, most people get better—but should the typical antibody response take the credit?
A new NIH-funded study of nearly 150 people who recovered from COVID-19 offers some essential insight. The study, published in the journal Nature, shows that most people, in fact, do produce antibodies that can effectively neutralize SARS-CoV-2. But there is a catch: 99 percent of the study’s participants didn’t make enough neutralizing antibodies to mount an ideal immune response.
The good news is that when researchers looked at individuals who mounted a strong immune response, they were able to identify three antibodies (depicted above) that were extremely effective at neutralizing SARS-CoV-2. By mass-producing copies of these antibodies as so-called monoclonal antibodies, the researchers can now better evaluate their potential as treatments to help people who don’t make strongly neutralizing antibodies, or not enough of them.
These findings come from a team led by Michel Nussenzweig, Paul Bieniasz, and Charles Rice at The Rockefeller University, New York, and Pamela Bjorkman at the California Institute of Technology, Pasadena. In the Nussenzweig lab, the team has spent years searching for broadly neutralizing antibodies against the human immunodeficiency virus (HIV). In response to the COVID-19 pandemic and its great urgency, Nussenzweig and team shifted their focus recently to look for promising antibodies against SARS-CoV-2.
Antibodies are blood proteins that the immune system makes to neutralize viruses or other foreign invaders. The immune system doesn’t make just one antibody to thwart an invader; it makes a whole family of antibodies. But not all antibodies in that family are created equal. They can vary widely in where they latch onto a virus like SARS-CoV-2, and that determines how effective each will be at blocking it from infecting human cells. That’s one reason why people respond differently to infections such as COVID-19.
In early April, Nussenzweig’s team began analyzing samples from volunteer survivors who visited The Rockefeller Hospital to donate plasma, which contains the antibodies. The volunteers had all recovered from mild-to-severe cases of COVID-19, showing their first signs of illness about 40 days prior to their first plasma collection.
Not surprisingly, all volunteers had produced antibodies in response to the virus. To test the strength of the antibodies, the researchers used a special assay that shows how effective each one is at blocking the virus from infecting human cells in lab dishes.
Overall, most of the plasma samples—118 of 149—showed at best poor to modest neutralizing activity. In about one-third of individuals, their plasma samples had below detectable levels of neutralizing activity. It’s possible those individuals just resolved the infection quickly, before more potent antibodies were produced.
More intriguing to the researchers were the results from two individuals that showed an unusually strong ability to neutralize SARS-CoV-2. Among these two “elite responders” and four other individuals, the researchers identified 40 different antibodies that could neutralize SARS-CoV-2. But again, not all antibodies are created equal. Three neutralized the virus even when present at extremely low levels, and they now will be studied further as possible monoclonal antibodies.
The team determined that those strongly neutralizing antibodies bind three distinct sites on the receptor-binding domain (RBD) of the coronavirus spike protein. This portion of the virus is important because it allows SARS-CoV-2 to bind and infect human cells. Importantly, when the researchers looked more closely at plasma samples with poor neutralizing ability, they found that they also contained those RBD-binding antibodies, just not in very large numbers.
These findings help not only to understand the immune response to COVID-19, they are also critical for vaccine design, revealing what a strong neutralizing antibody for SARS-CoV-2 should look like to help the immune system win. If a candidate vaccine can generate such strongly neutralizing antibodies, researchers will know that they are on the right track.
While this research showed that there’s a lot of variability in immune responses to SARS-CoV-2, it appears that most of us are inherently capable of producing antibodies to neutralize this devastating virus. That brings more reason for hope that the many vaccines now under study to elicit such neutralizing antibodies in sufficient numbers may afford us with much-needed immune protection.
Reference:
[1] Convergent antibody responses to SARS-CoV-2 in convalescent individuals. Robbiani DF, Gaebler C, Muecksch F, et al. Nature. 2020 Jun 18. [Published online ahead of print].
Links:
Coronavirus (COVID-19) (NIH)
Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV)
Nussenzweig Lab (The Rockefeller University, New York)
Bjorkman Lab (California Institute of Technology, Pasadena)
NIH Support: National Institute of Allergy and Infectious Diseases
Discussing the Need for Reliable Antibody Testing for COVID-19
Posted on by Dr. Francis Collins

There’s been a great deal of discussion about whether people who recover from coronavirus disease 2019 (COVID-19), have neutralizing antibodies in their bloodstream to guard against another infection. Lots of interesting data continue to emerge, including a recent preprint from researchers at Sherman Abrams Laboratory, Brooklyn, NY [1]. They tested 11,092 people for antibodies in May at a local urgent care facility and found nearly half had long-lasting IgG antibodies, a sign of exposure to the novel coronavirus SARS-CoV-2, the cause of COVID-19. The researchers also found a direct correlation between the severity of a person’s symptoms and their levels of IgG antibodies.
This study and others remind us of just how essential antibody tests will be going forward to learn more about this challenging pandemic. These assays must have high sensitivity and specificity, meaning there would be few false negatives and false positives, to tell us more about a person’s exposure to SARS-CoV-2. While there are some good tests out there, not all are equally reliable.
Recently, I had a chance to discuss COVID-19 antibody tests, also called serology tests, with Dr. Norman “Ned” Sharpless, Director of NIH’s National Cancer Institute (NCI). Among his many talents, Dr. Sharpless is an expert on antibody testing for COVID-19. You might wonder how NCI got involved in COVID-19 testing. Well, you’re going to find out. Our conversation took place while videoconferencing, with him connecting from North Carolina and me linking in from my home in Maryland. Here’s a condensed transcript of our chat:
Collins: Ned, thanks for joining me. Maybe we should start with the basics. What are antibodies anyway?
Sharpless: Antibodies are proteins that your body makes as part of the learned immune system. It’s the immunity that responds to a bacterium or a virus. In general, if you draw someone’s blood after an infection and test it for the presence of these antibodies, you can often know whether they’ve been infected. Antibodies can hang around for quite a while. How long exactly is a topic of great interest, especially in terms of the COVID-19 pandemic. But we think most people infected with coronavirus will make antibodies at a reasonably high level, or titer, in their peripheral blood within a couple of weeks of the infection.
Collins: What do antibodies tell us about exposure to a virus?
Sharpless: A lot of people with coronavirus are infected without ever knowing it. You can use these antibody assays to try and tell how many people in an area have been infected, that is, you can do a so-called seroprevalence survey.
You could also potentially use these antibody assays to predict someone’s resistance to future infection. If you cleared the infection and established immunity to it, you might be resistant to future infection. That might be very useful information. Maybe you could make a decision about how to go out in the community. So, that part is of intense interest as well, although less scientifically sound at the moment.
Collins: I have a 3D-printed model of SARS-CoV-2 on my desk. It’s sort of a spherical virus that has spike proteins on its surface. Do the antibodies interact with the virus in some specific ways?
Sharpless: Yes, antibodies are shaped like the letter Y. They have two binding domains at the head of each Y that will recognize something about the virus. We find antibodies in the peripheral blood that recognize either the virus nucleocapsid, which is the structural protein on the inside; or the spikes, which stick out and give coronavirus its name. We know now that about 99 percent of people who get infected with the virus will develop antibodies eventually. Most of those antibodies that you can detect to the spike proteins will be neutralizing, which means they can kill the virus in a laboratory experiment. We know from other viruses that, generally, having neutralizing antibodies is a promising sign if you want to be immune to that virus in the future.
Collins: Are COVID-19 antibodies protective? Are there reports of people who’ve gotten better, but then were re-exposed and got sick again?
Sharpless: It’s controversial. People can shed the virus’s nucleic acid [genetic material], for weeks or even more than a month after they get better. So, if they have another nucleic acid test it could be positive, even though they feel better. Often, those people aren’t making a lot of live virus, so it may be that they never stopped shedding the virus. Or it may be that they got re-infected. It’s hard to understand what that means exactly. If you think about how many people worldwide have had COVID-19, the number of legitimate possible reinfection cases is in the order of a handful. So, it’s a pretty rare event, if it happens at all.
Collins: For somebody who does have the antibodies, who apparently was previously infected, do they need to stop worrying about getting exposed? Can they can do whatever they want and stop worrying about distancing and wearing masks?
Sharpless: No, not yet. To use antibodies to predict who’s likely to be immune, you’ve got to know two things.
First: can the tests actually measure antibodies reliably? I think there are assays available to the public that are sufficiently good for asking this question, with an important caveat. If you’re trying to detect something that’s really rare in a population, then any test is going to have limitations. But if you’re trying to detect something that’s more common, as the virus was during the recent outbreak in Manhattan, I think the tests are up to the task.
Second: does the appearance of an antibody in the peripheral blood mean that you’re actually immune or you’re just less likely to get the virus? We don’t know the answer to that yet.
Collins: Let’s be optimistic, because it sounds like there’s some evidence to support the idea that people who develop these antibodies are protected against infection. It also sounds like the tests, at least some of them, are pretty good. But if there is protection, how long would you expect it to last? Is this one of those things where you’re all set for life? Or is this going to be something where somebody’s had it and might get it again two or three years from now, because the immunity faded away?
Sharpless: Since we have no direct experience with this virus over time, it’s hard to answer. The potential for this cell-based humoral immunity to last for a while is there. For some viruses, you have a long-lasting antibody protection after infection; for other viruses, not so much.
So that’s the unknown thing. Is immunity going to last for a while? Of course, if one were to bring up the topic of vaccines, that’s very important to know, because you would want to know how often one would have to give that vaccine, even under optimal circumstances.
Collins: Yes, our conversation about immunity is really relevant to the vaccines we’re trying to develop right now. Will these vaccines be protective for long periods of time? We sure hope so, but we’ve got to look carefully at the issue. Let’s come back, though, to the actual performance of the tests. The NCI has been right in the middle of trying to do this kind of validation. How did that happen, and how did that experience go?
Sharpless: Yes, I think one might ask: why is the National Cancer Institute testing antibody kits for the FDA? It is unusual, but certainly not unheard of, for NCI to take up problems like this during a time of a national emergency. During the HIV era, NCI scientists, along with others, identified the virus and did one of the first successful compound screens to find the drug AZT, one of the first effective anti-HIV therapies.
NCI’s Frederick National Lab also has a really good serology lab that had been predominantly working on human papillomavirus (HPV). When the need arose for serologic testing a few months ago, we pivoted that lab to a coronavirus serology lab. It took us a little while, but eventually we rounded up everything you needed to create positive and negative reference panels for antibody testing.
At that time, the FDA had about 200 manufacturers making serology tests that hoped for approval to sell. The FDA wanted some performance testing of those assays by a dispassionate third party. The Frederick National Lab seemed like the ideal place, and the manufacturers started sending us kits. I think we’ve probably tested on the order of 20 so far. We give those data back to the FDA for regulatory decision making. They’re putting all the data online.
Collins: How did it look? Are these all good tests or were there some clunkers?
Sharpless: There were some clunkers. But we were pleased to see that some of the tests appear to be really good, both in our hands and those of other groups, and have been used in thousands of patients.
There are a few tests that have sensitivities that are pretty high and specificities well over 99 percent. The Roche assay has a 99.8 percent specificity claimed on thousands of patients, and for the Mt. Sinai assay developed and tested by our academic collaborators in a panel of maybe 4,000 patients, they’re not sure they’ve ever had a false positive. So, there are some assays out there that are good.
Collins: There’s been talk about how there will soon be monoclonal antibodies directed against SARS-CoV-2. How are those derived?
Sharpless: They’re picked, generally, for appearing to have neutralizing activity. When a person makes antibodies, they don’t make one antibody to a pathogen. They make a whole family of them. And those can be individually isolated, so you can know which antibodies made by a convalescent individual really have virus-neutralizing capacity. That portion of the antibody that recognizes the virus can be engineered into a manufacturing platform to make monoclonal antibodies. Monoclonal means one kind of antibody. That approach has worked for other infectious diseases and is an interesting idea here too.
Collins: I can say a bit about that, because we are engaged in a partnership with industry and FDA called Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV). One of the hottest ideas right now is monoclonal antibodies, and we’re in the process of devising a master protocol, one for outpatients and one for inpatients.
Janet Woodcock of Operation Warp Speed tells me 21 companies are developing monoclonal antibodies. While doing these trials, we’d love to do comparisons, which is why it’s good to have an organization like ACTIV to bring everybody together, making sure you’re using the same endpoints and the same laboratory measures. I think that, maybe even by late summer, we might have some results. For people who are looking at what’s the next most-hopeful therapeutic option for people who are really sick with COVID-19, so far we have remdesivir. It helps, but it’s not a home run. Maybe monoclonal antibodies will be the next thing that really gives a big boost in survival. That would be the hope.
Ned, let me ask you one final question about herd, or group, immunity. One hears a bit about that in terms of how we are all going to get past this COVID-19 pandemic. What’s that all about?
Sharpless: Herd immunity is when a significant portion of the population is immune to a pathogen, then that pathogen will die out in the population. There just aren’t enough susceptible people left to infect. What the threshold is for herd immunity depends on how infectious the virus is. For a highly infectious virus, like measles, maybe up to 90 percent of the population must be immune to get herd immunity. Whereas for other less-infectious viruses, it may only be 50 percent of the population that needs to be immune to get herd immunity. It’s a theoretical thing that makes some assumptions, such as that everybody’s health status is the same and the population mixes perfectly every day. Neither of those are true.
How well that actual predictive number will work for coronavirus is unknown. The other thing that’s interesting is a lot of that work has been based on vaccines, such as what percentage do you have to vaccinate to get herd immunity? But if you get to herd immunity by having people get infected, so-called natural herd immunity, that may be different. You would imagine the most susceptible people get infected soonest, and so the heterogeneity of the population might change the threshold calculation.
The short answer is nobody wants to find out. No one wants to get to herd immunity for COVID-19 through natural herd immunity. The way you’d like to get there is with a vaccine that you then could apply to a large portion of the population, and have them acquire immunity in a more safe and controlled manner. Should we have an efficacious vaccine, this question will loom large: how many people do we need to vaccinate to really try and protect vulnerable populations?
Collins: That’s going to be a really critical question for the coming months, as the first large-scale vaccine trials get underway in July, and we start to see how they work and how successful and safe they are. But I’m also worried seeing some reports that 1 out of 5 Americans say they wouldn’t take a vaccine. It would be truly a tragedy if we have a safe and effective vaccine, but we don’t get enough uptake to achieve herd immunity. So, we’ve got some work to do on all fronts, that’s for sure.
Ned, I want to thank you for sharing all this information about antibodies and serologies and other things, as well as thank you for your hard work with all your amazing NCI colleagues.
Sharpless: Thanks for having me.
Reference:
[1] SARS-CoV-2 IgG Antibody Responses in New York City. Reifer J, Hayum N, Heszkel B, Klagsbald I, Streva VA. medRxiv. Preprint posted May 26, 2020.
Links:
Coronavirus (COVID-19) (NIH)
At NCI, A Robust and Rapid Response to the COVID-19 Pandemic. Norman E. Sharpless. Cancer Currents Blog. April 17, 2020 (National Cancer Institute/NIH)
Serological Testing for SARS-CoV-2 Antibodies (American Medical Association, Chicago)
COVID-19 Antibody Testing Primer (Infectious Diseases Society of America, Arlington, VA)
Accelerating COVID-19 Therapeutic Interventions and Vaccines (NIH)
Next Page