Lawrence Tabak, D.D.S., Ph.D.
Reflecting on Two Years of Discovery and Looking Ahead to New NIH Leadership
Posted on by Lawrence Tabak, D.D.S., Ph.D.
As I transition from my role as the Acting NIH Director, I’d like to thank you, the readers, for visiting the NIH Director’s Blog ever since I took the helm 22 months ago. From Long COVID to the opioid overdose epidemic to Alzheimer’s disease—we’ve covered a range of diseases and conditions, scientific advances, and programs. You were able to read about such a broad spectrum of science thanks in large part to the many Institute Directors at NIH who authored guest posts. I hope the blog has helped you learn more about what NIH does and the many ways that biomedical research impacts human health.
A key focus of my career as both a scientific investigator and administrative leader has been supporting trainees and finding new ways to cultivate and expand the next generation of researchers. In my many discussions with young investigators, I’ve often reminded them that they should not be afraid to fail. To the students and early-stage scientists who have visited this site: I hope these stories of discovery—often the result of earlier failures—have provided some insight and inspiration as you move through your scientific career or consider starting one.
I’d also like to thank the many people—employees, government and private partners, patients, scientists, advocates, and other members of the public—who have reached out with messages of support, and sometimes with messages of criticism. Both have helped inform the decisions I needed to make to fulfill the NIH mission.
In closing, I congratulate Dr. Monica Bertagnolli as she takes the helm as the next permanent NIH director. Dr. Bertagnolli—an outstanding physician scientist—is a strong leader who will bring fresh, bold new ideas to NIH and the biomedical research enterprise. I know she’ll be in good hands thanks to the outstanding staff across NIH and the leadership in the Department of Health and Human Services. I look forward to supporting her efforts and continuing to ensure that NIH research optimizes health for all people.
Senator Ben Cardin Visits NIH
Posted on by Lawrence Tabak, D.D.S., Ph.D.
First Lady Dr. Jill Biden Visits NIH
Posted on by Lawrence Tabak, D.D.S., Ph.D.

How Double-Stranded RNA Protects the Brain Against Infection While Making Damaging Neuroinflammation More Likely
Posted on by Lawrence Tabak, D.D.S., Ph.D.

When you get a run-of-the-mill viral infection, after a few days of symptoms your immune system typically fends off the bug, and you’ll make a full recovery. In rare cases, a virus can infect the brain. This can lead to much bigger problems, including cognitive impairments known as “brain fog,” other neuropsychiatric symptoms, potentially irreversible brain damage, or even death. For this reason, the brain, more than other parts of the body, relies heavily on immune responses that can control viral infections immediately.
Now some intriguing findings from an NIH-funded team reported in Science Immunology help to explain how the brain is protected against infections.1 However, the findings also highlight a serious downside: these same mechanisms that protect the brain also leave it especially vulnerable to damaging levels of neuroinflammation.
The new findings may help to explain what goes on in the brains of people with a wide range of neurodegenerative conditions, including amyotrophic lateral sclerosis (ALS) and Alzheimer’s disease. They also point to promising targets for developing treatments that might turn inflammatory immune responses in the brain up or down, as desired, to treat these and other serious conditions.
How does it work? The key is double-stranded RNA (dsRNA).
RNA molecules are readouts of genetic information in DNA that carry instructions for building the proteins that carry out various cell functions. RNA molecules in our cells are most often in single-stranded or short dsRNA form. In contrast, lengthy dsRNAs are a hallmark of viruses. When a virus invades our cells, our immune system’s first line of defense can sense those long viral dsRNAs and trigger a response.
But it turns out that dsRNAs aren’t unique to viruses, as the new study highlights. The researchers, led by Tyler Dorrity and Heegwon Shin, both members of Hachung Chung’s lab at Columbia University Irving Medical Center, New York, found that human neurons—even when they’re normal and healthy—also have exceptionally high levels of long dsRNAs.
Their lab studies in cells and tissues show that these dsRNAs in neurons can trigger an inflammatory immune response just as they do in viruses. By manipulating neurons in a way that cut back on the number of dsRNAs, they found they could lower the innate immune response. However, cells with fewer dsRNAs also showed greater susceptibility to infection with Zika viruses and herpes simplex virus, which can produce a form of viral encephalitis.
The researchers also knew from earlier studies that people with a rare, inherited condition called Aicardi-Goutières syndrome (AGS), which primarily affects the brain and immune system, carry a mutation that causes their cells to lack an enzyme needed to edit dsRNAs. As a result, neurons carrying this mutation have so many dsRNAs that it is toxic.
They went on to show that they could shift this dynamic by altering levels of two other proteins that bind RNA. The proteins normally encourage dsRNA formation in the brain. When the researchers deleted these RNA-binding proteins from the AGS neurons, those neurons made fewer long dsRNAs, which in turn protected them from the inflammatory immune responses and allowed them to survive longer. As expected, however, those cells also were more susceptible to viral infection.
The findings show how this tricky balance between susceptibility to infection and inflammation in the brain works in both health and disease. It also leads to the tantalizing suggestion that treatments targeting these various players or others in the same pathways may offer new ways of treating brain infections or neuroinflammatory conditions, by boosting or dampening dsRNA levels and the associated immune responses. As a next step, the researchers report that they’re pursuing studies to explore the role of dsRNA-triggered immune responses in ALS and Alzheimer’s, as well as in neuropsychiatric symptoms sometimes seen in people with lupus.
References:
[1] TJ Dorrity TJ, et al. Long 3’UTRs predispose neurons to inflammation by promoting immunostimulatory double-stranded RNA formation. Science Immunology DOI: 10.1126/sciimmunol.adg2979 (2023).
NIH Support: National Institute of Neurological Disorders and Stroke, National Institute of Allergy and Infectious Diseases, National Institute of General Medical Sciences
Brain Atlas Paves the Way for New Understanding of How the Brain Functions
Posted on by Lawrence Tabak, D.D.S., Ph.D.

When NIH launched The BRAIN Initiative® a decade ago, one of many ambitious goals was to develop innovative technologies for profiling single cells to create an open-access reference atlas cataloguing the human brain’s many parts. The ultimate goal wasn’t to produce a single, static reference map, but rather to capture a dynamic view of how the brain’s many cells of varied types are wired to work together in the healthy brain and how this picture may shift in those with neurological and mental health disorders.
So I’m now thrilled to report the publication of an impressive collection of work from hundreds of scientists in the BRAIN Initiative Cell Census Network (BICCN), detailed in more than 20 papers in Science, Science Advances, and Science Translational Medicine.1 Among many revelations, this unprecedented, international effort has characterized more than 3,000 human brain cell types. To put this into some perspective, consider that the human lung contains 61 cell types.2 The work has also begun to uncover normal variation in the brains of individual people, some of the features that distinguish various disease states, and distinctions among key parts of the human brain and those of our closely related primate cousins.
Of course, it’s not possible to do justice to this remarkable body of work or its many implications in the space of a single blog post. But to give you an idea of what’s been accomplished, some of these studies detail the primary effort to produce a comprehensive brain atlas, including defining the brain’s many cell types along with their underlying gene activity and the chemical modifications that turn gene activity up or down.3,4,5
Other studies in this collection take a deep dive into more specific brain areas. For instance, to capture normal variations among people, a team including Nelson Johansen, University of California, Davis, profiled cells in the neocortex—the outermost portion of the brain that’s responsible for many complex human behaviors.6 Overall, the work revealed a highly consistent cellular makeup from one person to the next. But it also highlighted considerable variation in gene activity, some of which could be explained by differences in age, sex and health. However, much of the observed variation remains unexplained, opening the door to more investigations to understand the meaning behind such brain differences and their role in making each of us who we are.
Yang Li, now at Washington University in St. Louis, and his colleagues analyzed 1.1 million cells from 42 distinct brain areas in samples from three adults.4 They explored various cell types with potentially important roles in neuropsychiatric disorders and were able to pinpoint specific cell types, genes and genetic switches that may contribute to the development of certain traits and disorders, including bipolar disorder, depression and schizophrenia.
Yet another report by Nikolas Jorstad, Allen Institute, Seattle, and colleagues delves into essential questions about what makes us human as compared to other primates like chimpanzees.7 Their comparisons of gene activity at the single-cell level in a specific area of the brain show that humans and other primates have largely the same brain cell types, but genes are activated differently in specific cell types in humans as compared to other primates. Those differentially expressed genes in humans often were found in portions of the genome that show evidence of rapid change over evolutionary time, suggesting that they play important roles in human brain function in ways that have yet to be fully explained.
All the data represented in this work has been made publicly accessible online for further study. Meanwhile, the effort to build a more finely detailed picture of even more brain cell types and, with it, a more complete understanding of human brain circuitry and how it can go awry continues in the BRAIN Initiative Cell Atlas Network (BICAN). As impressive as this latest installment is—in our quest to understand the human brain, brain disorders, and their treatment—we have much to look forward to in the years ahead.
References:
A list of all the papers part of the brain atlas research is available here: https://www.science.org/collections/brain-cell-census.
[1] M Maroso. A quest into the human brain. Science DOI: 10.1126/science.adl0913 (2023).
[2] L Sikkema, et al. An integrated cell atlas of the lung in health and disease. Nature Medicine DOI: 10.1038/s41591-023-02327-2 (2023).
[3] K Siletti, et al. Transcriptomic diversity of cell types across the adult human brain. Science DOI: 10.1126/science.add7046 (2023).
[4] Y Li, et al. A comparative atlas of single-cell chromatin accessibility in the human brain. Science DOI: 10.1126/science.adf7044 (2023).
[5] W Tian, et al. Single-cell DNA methylation and 3D genome architecture in the human brain. Science DOI: 10.1126/science.adf5357 (2023).
[6] N Johansen, et al. Interindividual variation in human cortical cell type abundance and expression. Science DOI: 10.1126/science.adf2359 (2023).
[7] NL Jorstad, et al. Comparative transcriptomics reveals human-specific cortical features. Science DOI: 10.1126/science.ade9516 (2023).
NIH Support: Projects funded through the NIH BRAIN Initiative Cell Consensus Network
Can Bioprinted Skin Substitutes Replace Traditional Grafts for Treating Burn Injuries and Other Serious Skin Wounds?
Posted on by Lawrence Tabak, D.D.S., Ph.D.
Each year in the U.S., more than 500,000 people receive treatment for burn injuries and other serious skin wounds.1 To close the most severe wounds with less scarring, doctors often must surgically remove skin from one part of a person’s body and use it to patch the injured site. However, this is an intensive process, and some burn patients with extensive skin loss do not have sufficient skin available for grafting. Scientists have been exploring ways to repair these serious skin wounds without skin graft surgery.
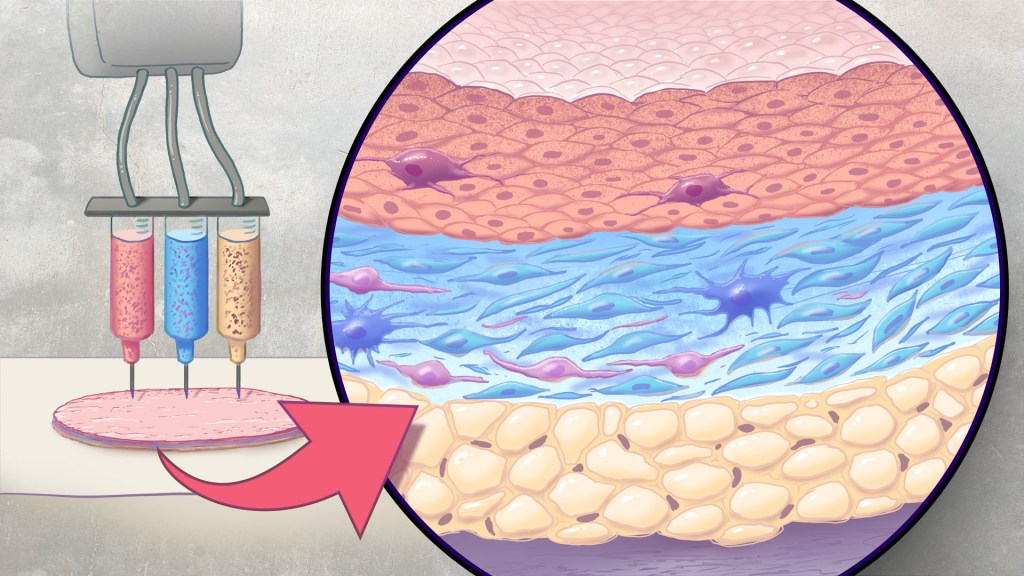
An NIH-funded team recently showed that bioprinted skin substitutes may serve as a promising alternative to traditional skin grafts in preclinical studies reported in Science Translational Medicine.2 The approach involves a portable skin bioprinter system that deposits multiple layers of skin directly into a wound. The recent findings add to evidence that bioprinting technology can successfully regenerate human-like skin to allow healing. While this approach has yet to be tested in people, it confirms that such technologies already can produce skin constructs with the complex structures and multiple cell types present in healthy human skin.
This latest work comes from a team led by Adam Jorgensen and Anthony Atala at Wake Forest School of Medicine’s Wake Forest Institute for Regenerative Medicine, Winston-Salem, NC. Members of the Atala lab and their colleagues had earlier shown it was possible to isolate two major skin cell types found in the skin’s outer (epidermis) and middle (dermis) layers from a small biopsy of healthy skin, expand the number of cells in the lab and then deliver the cells directly into an injury using a specially designed bioprinter.3 Using integrated imaging technology to scan a wound, computer software “prints” cells right into an injury, mimicking two of our skin’s three natural layers.
In the new study, Atala’s team has gone even further to construct skin substitutes that mimic the structure of human skin and that include six primary human skin cell types. They then used their bioprinter to produce skin constructs with all three layers found in healthy human skin: epidermis, dermis, and hypodermis.
To put their skin substitutes to the test, they first transplanted them into mice. Their studies showed that the bioprinted skin encouraged the rapid growth of new blood vessels and had other features of normal-looking, healthy skin. The researchers were able to confirm that their bioprinted skin implants successfully integrated into the animals’ regenerated skin to speed healing.
Studies in a pig model of wound healing added to evidence that such bioprinted implants can successfully repair full-thickness wounds, meaning those that extend through all three layers of skin. The bioprinted skin patches allowed for improved wound healing with less scarring. They also found that the bioprinted grafts encouraged activity in the skin from genes known to play important roles in wound healing.
It’s not yet clear if this approach will work as well in the clinic as it does in the lab. To make it feasible, the researchers note there’s a need for improved approaches to isolating and expanding the needed skin cell types. Nevertheless, these advances come as encouraging evidence that bioprinted skin substitutes could one day offer a promising alternative to traditional skin grafts with the capacity to help even more people with severe burns or other wounds.
References:
[1] Burn Incidence Fact Sheet. American Burn Association
[2] AM Jorgensen, et al. Multicellular bioprinted skin facilitates human-like skin architecture in vivo. Science Translational Medicine DOI: 10.1126/scitranslmed.adf7547 (2023).
[3] M Albanna, et al. In Situ Bioprinting of Autologous Skin Cells Accelerates Wound Healing of Extensive Excisional Full-Thickness Wounds. Scientific Reports DOI: 10.1038/s41598-018-38366-w (2019).
NIH Support: National Institute of Arthritis and Musculoskeletal and Skin Diseases
Persistence Pays Off: Recognizing Katalin Karikó and Drew Weissman, the 2023 Nobel Prize Winners in Physiology or Medicine
Posted on by Lawrence Tabak, D.D.S., Ph.D.
Last week, biochemist Katalin Karikó and immunologist Drew Weissman earned the Nobel Prize in Physiology or Medicine for their discoveries that enabled the development of effective messenger RNA (mRNA) vaccines against COVID-19. On behalf of the NIH community, I’d like to congratulate Karikó and Weissman and thank them for their persistence in pursuing their investigations. NIH is proud to have supported their seminal research, cited by the Nobel Assembly as key publications.1,2,3
While the lifesaving benefits of mRNA vaccines are now clearly realized, Karikó and Weissman’s breakthrough finding in 2005 was not fully appreciated at the time as to why it would be significant. However, their dogged dedication to gaining a better understanding of how RNA interacts with the immune system underscores the often-underappreciated importance of incremental research. Following where the science leads through step-by-step investigations often doesn’t appear to be flashy, but it can end up leading to major advances.
To best describe Karikó and Weissman’s discovery, I’ll first do a quick review of vaccine history. As many of you know, vaccines stimulate our immune systems to protect us from getting infected or from getting very sick from a specific pathogen. Since the late 1700s, scientists have used various approaches to design effective vaccines. Some vaccines introduce a weakened or noninfectious version of a virus to the body, while others present only a small part of the virus, like a protein. The immune system detects the weak or partial virus and develops specialized defenses against it. These defenses work to protect us if we are ever exposed to the real virus.
In the early 1990s, scientists began exploring a different approach to vaccines that involved delivering genetic material, or instructions, so the body’s own cells could make the virus proteins that stimulate an immune response.4,5 Because this approach eliminates the step of growing virus or virus protein in the laboratory—which can be difficult to do in very large quantities and can require a lot of time and money—it had potential, in theory, to be a faster and cheaper way to manufacture vaccines.
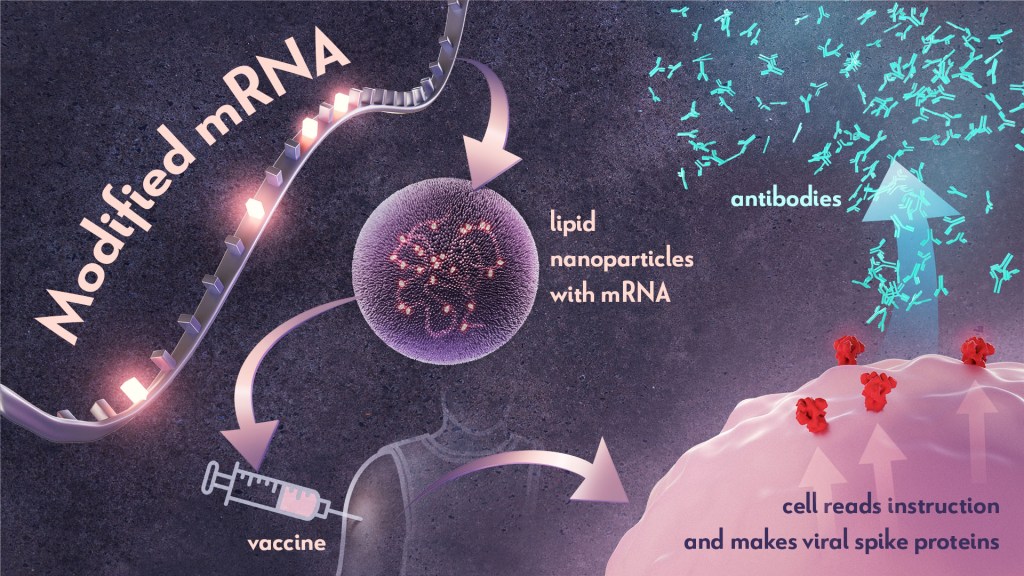
Scientists were exploring two types of vaccines as part of this new approach: DNA vaccines and messenger RNA (mRNA) vaccines. DNA vaccines deliver an encoded protein recipe that the cell first copies or transcribes before it starts making protein. For mRNA vaccines, the transcription process is done in the laboratory, and the vaccine delivers the “readable” instructions to the cell for making protein. However, mRNA was not immediately a practical vaccine approach due to several scientific hurdles, including that it caused inflammatory reactions that could be unhealthy for people.
Unfazed by the challenges, Karikó and Weissman spent years pursuing research on RNA and the immune system. They had a brilliant idea that they turned into a significant discovery in 2005 when they proved that inserting subtle chemical modifications to lab-transcribed mRNA eliminated the unwanted inflammatory response.1 In later studies, the pair showed that these chemical modifications also increased protein production.2,3 Both discoveries would be critical to advancing the use of mRNA-based vaccines and therapies.
Earlier theories that mRNA could enable rapid vaccine development turned out to be true. By March 2020, the first clinical trial of an mRNA vaccine for COVID-19 had begun enrolling volunteers, and by December 2020, health care workers were receiving their first shots. This unprecedented timeline was only possible because of Karikó and Weissman’s decades of work, combined with the tireless efforts of many academic, industry and government scientists, including several from the NIH intramural program. Now, researchers are exploring how mRNA could be used in vaccines for other infectious diseases and in cancer vaccines.
As an investigator myself, I’m fascinated by how science continues to build on itself—a process that is done out of the public eye. Luckily every year, the Nobel Prize briefly illuminates for the larger public this long arc of scientific discovery. The Nobel Assembly’s recognition of Karikó and Weissman is a tribute to all scientists who do the painstaking work of trying to understand how things work. Many of the tools we have today to better prevent and treat diseases would not have been possible without the brilliance, tenacity and grit of researchers like Karikó and Weissman.
References:
- K Karikó, et al. Suppression of RNA Recognition by Toll-like Receptors: The impact of nucleoside modification and the evolutionary origin of RNA. Immunity DOI: 10.1016/j.immuni.2005.06.008 (2005).
- K Karikó, et al. Incorporation of pseudouridine into mRNA yields superior nonimmunogenic vector with increased translational capacity and biological stability. Molecular Therapy DOI: 10.1038/mt.2008.200 (2008).
- BR Anderson, et al. Incorporation of pseudouridine into mRNA enhances translation by diminishing PKR activation. Nucleic Acids Research DOI: 10.1093/nar/gkq347 (2010).
- DC Tang, et al. Genetic immunization is a simple method for eliciting an immune response. Nature DOI: 10.1038/356152a0 (1992).
- F Martinon, et al. Induction of virus-specific cytotoxic T lymphocytes in vivo by liposome-entrapped mRNA. European Journal of Immunology DOI: 10.1002/eji.1830230749 (1993).
NIH Support:
Katalin Karikó: National Heart, Lung, and Blood Institute; National Institute of Neurological Disorders and Stroke
Drew Weissman: National Institute of Allergy and Infectious Diseases; National Institute of Dental and Craniofacial Research; National Heart, Lung, and Blood Institute
Taking a Deep Dive into the Alzheimer’s Brain in Search of Understanding and New Targets
Posted on by Lawrence Tabak, D.D.S., Ph.D.

People living with Alzheimer’s disease experience a gradual erosion of memory and thinking skills until they can no longer carry out daily activities. Hallmarks of the disease include the buildup of plaques that collect between neurons, accumulations of tau protein inside neurons and weakening of neural connections. However, there’s still much to learn about what precisely happens in the Alzheimer’s brain and how the disorder’s devastating march might be slowed or even stopped. Alzheimer’s affects more than six million people in the United States and is the seventh leading cause of death among adults in the U.S., according to the National Institute on Aging.
NIH-supported researchers recently published a trove of data in the journal Cell detailing the molecular drivers of Alzheimer’s disease and which cell types in the brain are most likely to be affected.1,2,3,4 The scientists, led by Li-Huei Tsai and Manolis Kellis, both at the Massachusetts Institute of Technology, Cambridge, MA, characterized gene activity at the single-cell level in more than two million cells from postmortem brain tissue. They also assessed DNA damage and surveyed epigenetic changes in cells, which refers to chemical modifications to DNA that alter gene expression in the cell. The findings could help researchers pinpoint new targets for Alzheimer’s disease treatments.
In the first of four studies, the researchers examined 54 brain cell types in 427 brain samples from a cohort of people with varying levels of cognitive impairment that has been followed since 1994.1 The MIT team generated an atlas of gene activity patterns within the brain’s prefrontal cortex, an important area for memory retrieval.
Their analyses in brain samples taken from people with Alzheimer’s dementia showed altered activity in genes involved in various functions. Additional findings showed that people with normal cognitive abilities with evidence of plaques in their brains had more neurons that inhibit or dampen activity in the prefrontal cortex compared to those with Alzheimer’s dementia. The finding suggests that the workings of inhibitory neurons may play an unexpectedly important role in maintaining cognitive resilience despite age-related changes, including the buildup of plaques. It’s one among many discoveries that now warrant further study.
In another report, the researchers compared brain tissues from 48 people without Alzheimer’s to 44 people with early- or late-stage Alzheimer’s.2 They developed a map of the various elements that regulate function within cells in the prefrontal cortex. By cross-referencing epigenomic and gene activity data, the researchers showed changes in many genes with known links to Alzheimer’s disease development and risk.
Their single-cell analysis also showed that these changes most often occur in microglia, which are immune cells that remove cellular waste products from the brain. At the same time, every cell type they studied showed a breakdown over time in the cells’ normal epigenomic patterning, a process that may cause a cell to behave differently as it loses essential aspects of its original identity and function.
In a third report, the researchers looked even deeper into gene activity within the brain’s waste-clearing microglia.3 Based on the activity of hundreds of genes, they were able to define a dozen distinct microglia “states.” They also showed that more microglia enter an inflammatory state in the Alzheimer’s brain compared to a healthy human brain. Fewer microglia in the Alzheimer’s brain were in a healthy, balanced state as well. The findings suggest that treatments that target microglia to reduce inflammation and promote balance may hold promise for treating Alzheimer’s disease.
The fourth and final report zeroed in on DNA damage, inspired in part by earlier findings suggesting greater damage within neurons even before Alzheimer’s symptoms appear.4 In fact, breaks in DNA occur as part of the normal process of forming new memories. But those breaks in the healthy brain are quickly repaired as the brain makes new connections.
The researchers studied postmortem brain tissue samples and found that, over time in the Alzheimer’s brain, the damage exceeds the brain’s ability to repair it. As a result, attempts to put the DNA back together leads to a patchwork of mistakes, including rearrangements in the DNA and fusions as separate genes are merged. Such changes appear to arise especially in genes that control neural connections, which may contribute to the signs and symptoms of Alzheimer’s.
The researchers say they now plan to apply artificial intelligence and other analytic tools to learn even more about Alzheimer’s disease from this trove of data. To speed progress even more, they’ve made all the data freely available online to the research community, where it promises to yield many more fundamentally important discoveries about the precise underpinnings of Alzheimer’s disease in the brain and new ways to intervene in Alzheimer’s dementia.
References:
[1] Mathys H, et al. Single-cell atlas reveals correlates of high cognitive function, dementia, and resilience to Alzheimer’s disease pathology. Cell. DOI: 10.1016/j.cell.2023.08.039. (2023).
[2] Xiong X, et al. Epigenomic dissection of Alzheimer’s disease pinpoints causal variants and reveals epigenome erosion. Cell. DOI: 10.1016/j.cell.2023.08.040. (2023).
[3] Sun N, et al. Human microglial state dynamics in Alzheimer’s disease progression. Cell. DOIi: 10.1016/j.cell.2023.08.037. (2023).
[4] Dileep V, et al. Neuronal DNA double-strand breaks lead to genome structural variations and 3D genome disruption in neurodegeneration. Cell. 2023 DOI: 10.1016/j.cell.2023.08.038. (2023).
NIH Support: National Institute on Aging, National Institute of Neurological Disorders and Stroke, National Institute of Mental Health, National Institute of General Medical Sciences
Pain Circuit Discovery in the Brain Suggests Promising Alternative to Opioid Painkillers
Posted on by Lawrence Tabak, D.D.S., Ph.D.

Chronic pain is an often-debilitating health condition and serious public health concern, affecting more than 50 million Americans.1 The opioid and overdose crisis, which stems from inadequate pain treatment, continues to have a devastating impact on families and communities across the country. To combat both challenges, we urgently need new ways to treat acute and chronic pain effectively without the many downsides of opioids.
While there are already multiple classes of non-opioid pain medications and other approaches to manage pain, unfortunately none have proved as effective as opioids when it comes to pain relief. So, I’m encouraged to see that an NIH-funded team now has preclinical evidence of a promising alternative target for pain-relieving medicines in the brain.2
Rather than activating opioid receptors, the new approach targets receptors for a nerve messenger known as acetylcholine in a portion of the brain involved in pain control. Based on findings from animal models, it appears that treatments targeting acetylcholine could offer pain relief even in people who have reduced responsiveness to opioids. Their findings suggest that the treatment approach has the potential to remain effective in combatting pain long-term and with limited risk for withdrawal symptoms or addiction.
The researchers, led by Daniel McGehee, University of Chicago, focused their attention on non-opioid pathways in the ventrolateral periaqueductal gray (vlPAG), a brain area involved in pain control. They had previously shown that activating acetylcholine receptors, which are part of the vlPAG’s underlying circuitry, could relieve pain.3 However, they found that when the body is experiencing pain, it unexpectedly suppresses acetylcholine rather than releasing more.
To understand how and why this is happening, McGehee and Shivang Sullere, now a postdoctoral fellow at Harvard Medical School, conducted studies in mice to understand how acetylcholine is released under various pain states. They found that mice treated with a drug that stimulates an acetylcholine receptor known as alpha-7 (⍺7) initially led to more activity in the nervous system. But this activity quickly gave way to a prolonged inactive or quiet state that delivered pain relief. Interestingly, this unexpected inhibitory effect lasted for several hours.
Additional studies in mice that had developed a tolerance to opioids showed the same long-lasting pain relief. This encouraging finding was expected since opioids use a pathway separate from acetylcholine. In more good news, the animals didn’t show any signs of dependence or addiction either. For instance, in the absence of pain, they didn’t prefer spending time in environments where they’d receive the ⍺7-targeted drug.
Imaging studies measuring brain activity revealed greater activity in cells expressing ⍺7 with higher levels of pain. When that activity was blocked, pain levels dropped. The finding suggests to the researchers it may be possible to monitor pain levels through brain imaging. It’s also possible the acetylcholine circuitry in the brain may play a role in the process whereby acute or temporary pain becomes chronic.
Finding treatments to modify acetylcholine levels or target acetylcholine receptors may therefore offer a means to treat pain and prevent it from becoming chronic. Encouragingly, drugs acting on these receptors already have been tested for use in people for treating other health conditions. It will now be important to learn whether these existing therapeutics or others like them may act as highly effective, non-addictive painkillers, with important implications for alleviating chronic pain.
References:
[1] NIH HEAL Initiative Research Plan. NIH HEAL Initiative.
[2] Sullere S et al. A cholinergic circuit that relieves pain despite opioid tolerance. Neuron. DOI: 10.1016/j.neuron.2023.08.017 (2023).
[3] Umana IC et al. Nicotinic modulation of descending pain control circuitry. Pain. PMID: 28817416; PMCID: PMC5873975 (2017).
Links:
The Helping to End Addiction Long-term® (HEAL) Initiative (NIH)
Pain (National Institute of Neurological Disorders and Stroke/NIH)
Opioids (National Institute on Drug Abuse/NIH)
Daniel McGehee (University of Chicago, Illinois)
NIH Support: National Institute of Neurological Disorders and Stroke, National Institute on Drug Abuse
Words Matter, Actions Have Impact: Updating the NIH Mission Statement
Posted on by Lawrence Tabak, D.D.S., Ph.D.

I’ve previously written and spoken about how diverse perspectives are essential to innovation and scientific advancement.1 Scientists and experts with different backgrounds and lived experiences can offer diverse and creative solutions to solve complex problems. We’re taking steps to create a culture within the biomedical and behavioral research enterprise of inclusion, equity, and respect for every member of society. We are also working to strengthen our efforts to include populations in research that have not been historically included or equitably treated.
As part of our effort to ensure that all people are included in NIH research, we’re updating our mission statement to reflect better the spirit of the agency’s work to optimize health for all people. The proposed, new statement is as follows:
“To seek fundamental knowledge about the nature and behavior of living systems and to apply that knowledge to optimize health and prevent or reduce illness for all people.”
Recently, we asked a team of subject matter experts to form a subgroup of the Advisory Committee to the Director’s Working Group on Diversity to advise NIH on how we can support the inclusion of people with disabilities in the scientific workforce and in the research enterprise. One of the subgroup’s recommendations was to update the current NIH mission statement to remove “reducing disability.” The subgroup explained that this language could be interpreted as perpetuating ableist beliefs that people with disabilities are flawed and need to be “fixed.”
Disability is often viewed solely as a medical problem requiring a cure or correction. However, this view can be stigmatizing as it focuses only on a perceived flaw in the individual. It does not account for how people identify and view themselves. It also does not account for the ways that society can be unaccommodating for people with disabilities.2,3 It’s important that we recognize the varied, nuanced and complex lived experiences among people with disabilities, many of whom may also face additional barriers as members of racial, ethnic, sexual and gender minority groups, people with lower incomes, and people who live in rural communities that are medically underserved.
Some of you may recall that we updated our mission statement in 2013 to remove phrasing that implied disability was a burden, since many people do not find their disabilities to be burdensome. As we re-examine our mission statement again in 2023, I’m reminded that strengthening diversity, equity, inclusion and accessibility (DEIA) is an ongoing process requiring our sustained engagement.
The input we’ve received has made it clear that words matter—language can perpetuate prejudices and implicit attitudes, which in turn can affect people’s behavior. We also acknowledge that it is time for the agency to review and consider how the words of our mission statement may affect the direction of our science.
In response, we are seeking the public’s input on the proposed, revised statement to ensure that it reflects the NIH mission as accurately as possible. The NIH mission should be inclusive of those who conduct research, those who participate in research, and those we serve—the American public. Anyone interested in providing feedback can send it to this submission website through Nov. 24, 2023.
We are grateful for the subgroup’s work and appreciate their time examining this issue in depth. I also want to recognize the helpful feedback that we’ve received from the disability community within NIH through the years, including recent listening sessions that helped guide the development of NIH’s DEIA Strategic Plan.
Going beyond the scientific workforce, both the Strategic Plan and the subgroup’s report recognize the importance of research on health disparities. People with disabilities often experience health conditions leading to poorer health and face discrimination, inequality and structural barriers that inhibit access to health care, resulting in poorer health outcomes. NIH recently designated people with disabilities as a population with health disparities to encourage research specific to the health issues and unmet health needs of the disability community. NIH also issued a funding opportunity calling for research applications that address the intersecting impact of disability, race, ethnicity, and socioeconomic status on healthcare access and health outcomes.
The subgroup provided additional recommendations that we’re in the process of reviewing. We know one of our key challenges is data gathering that would give us a better snapshot of the workforce and the research we support. According to the CDC, 1 in 4 adults in the United States have a disability. However, in 2022 only 1.3% of principal investigators on NIH research grant applications and awards self-reported a disability. In 2022, 8.6% of the NIH workforce reported having a disability; however, I recognize that this is likely not reflective of the true percentage. We know that some people do not want to self-disclose for numerous reasons, including the fear of discrimination.
We hope that, in part, changing the mission statement would be a step in the right direction of changing the culture at NIH and the larger biomedical and behavioral research enterprise. I know that our efforts have sometimes fallen short, but we will continually work to foster a culture of inclusive excellence where people with disabilities and all people feel like they truly belong and are embraced as an asset to the NIH mission.
References:
[1] MA Bernard et al. The US National Institutes of Health approach to inclusive excellence. Nature Medicine DOI:10.1038/s41591-021-01532-1 (2021)
[2] DS Dunn & EE Andrews. Person-first and identity-first language: Developing psychologists’ cultural competence using disability language The American Psychologist DOI: 10.1037/a0038636 (2015)
[3] International Classification of Functioning, Disability and Health (2002) Towards a Common Language for Functioning, Disability and Health. World Health Organization https://cdn.who.int/media/docs/default-source/classification/icf/icfbeginnersguide.pdf
Links:
ACD Working Group on Diversity, Subgroup on Individuals with Disabilities, NIH
Request for Information: Inviting Comments and Suggestions on Updating the NIH Mission Statement, NIH
NIH designates people with disabilities as a population with health disparities, Sept. 26, 2023, NIH News Releases
NIH-Wide Strategic Plan for Diversity, Equity, Inclusion, and Accessibility (DEIA), NIH
Disability and Health Overview, CDC
Data on Researchers’ Self-Reported Disability Status, NIH Office Of Extramural Research
Total NIH Workforce Demographics for Fiscal Year 2022 Fourth Quarter, NIH Office of Equity, Diversity, and Inclusion
Next Page