mRNA
Persistence Pays Off: Recognizing Katalin Karikó and Drew Weissman, the 2023 Nobel Prize Winners in Physiology or Medicine
Posted on by Lawrence Tabak, D.D.S., Ph.D.
Last week, biochemist Katalin Karikó and immunologist Drew Weissman earned the Nobel Prize in Physiology or Medicine for their discoveries that enabled the development of effective messenger RNA (mRNA) vaccines against COVID-19. On behalf of the NIH community, I’d like to congratulate Karikó and Weissman and thank them for their persistence in pursuing their investigations. NIH is proud to have supported their seminal research, cited by the Nobel Assembly as key publications.1,2,3
While the lifesaving benefits of mRNA vaccines are now clearly realized, Karikó and Weissman’s breakthrough finding in 2005 was not fully appreciated at the time as to why it would be significant. However, their dogged dedication to gaining a better understanding of how RNA interacts with the immune system underscores the often-underappreciated importance of incremental research. Following where the science leads through step-by-step investigations often doesn’t appear to be flashy, but it can end up leading to major advances.
To best describe Karikó and Weissman’s discovery, I’ll first do a quick review of vaccine history. As many of you know, vaccines stimulate our immune systems to protect us from getting infected or from getting very sick from a specific pathogen. Since the late 1700s, scientists have used various approaches to design effective vaccines. Some vaccines introduce a weakened or noninfectious version of a virus to the body, while others present only a small part of the virus, like a protein. The immune system detects the weak or partial virus and develops specialized defenses against it. These defenses work to protect us if we are ever exposed to the real virus.
In the early 1990s, scientists began exploring a different approach to vaccines that involved delivering genetic material, or instructions, so the body’s own cells could make the virus proteins that stimulate an immune response.4,5 Because this approach eliminates the step of growing virus or virus protein in the laboratory—which can be difficult to do in very large quantities and can require a lot of time and money—it had potential, in theory, to be a faster and cheaper way to manufacture vaccines.
Scientists were exploring two types of vaccines as part of this new approach: DNA vaccines and messenger RNA (mRNA) vaccines. DNA vaccines deliver an encoded protein recipe that the cell first copies or transcribes before it starts making protein. For mRNA vaccines, the transcription process is done in the laboratory, and the vaccine delivers the “readable” instructions to the cell for making protein. However, mRNA was not immediately a practical vaccine approach due to several scientific hurdles, including that it caused inflammatory reactions that could be unhealthy for people.
Unfazed by the challenges, Karikó and Weissman spent years pursuing research on RNA and the immune system. They had a brilliant idea that they turned into a significant discovery in 2005 when they proved that inserting subtle chemical modifications to lab-transcribed mRNA eliminated the unwanted inflammatory response.1 In later studies, the pair showed that these chemical modifications also increased protein production.2,3 Both discoveries would be critical to advancing the use of mRNA-based vaccines and therapies.
Earlier theories that mRNA could enable rapid vaccine development turned out to be true. By March 2020, the first clinical trial of an mRNA vaccine for COVID-19 had begun enrolling volunteers, and by December 2020, health care workers were receiving their first shots. This unprecedented timeline was only possible because of Karikó and Weissman’s decades of work, combined with the tireless efforts of many academic, industry and government scientists, including several from the NIH intramural program. Now, researchers are exploring how mRNA could be used in vaccines for other infectious diseases and in cancer vaccines.
As an investigator myself, I’m fascinated by how science continues to build on itself—a process that is done out of the public eye. Luckily every year, the Nobel Prize briefly illuminates for the larger public this long arc of scientific discovery. The Nobel Assembly’s recognition of Karikó and Weissman is a tribute to all scientists who do the painstaking work of trying to understand how things work. Many of the tools we have today to better prevent and treat diseases would not have been possible without the brilliance, tenacity and grit of researchers like Karikó and Weissman.
References:
- K Karikó, et al. Suppression of RNA Recognition by Toll-like Receptors: The impact of nucleoside modification and the evolutionary origin of RNA. Immunity DOI: 10.1016/j.immuni.2005.06.008 (2005).
- K Karikó, et al. Incorporation of pseudouridine into mRNA yields superior nonimmunogenic vector with increased translational capacity and biological stability. Molecular Therapy DOI: 10.1038/mt.2008.200 (2008).
- BR Anderson, et al. Incorporation of pseudouridine into mRNA enhances translation by diminishing PKR activation. Nucleic Acids Research DOI: 10.1093/nar/gkq347 (2010).
- DC Tang, et al. Genetic immunization is a simple method for eliciting an immune response. Nature DOI: 10.1038/356152a0 (1992).
- F Martinon, et al. Induction of virus-specific cytotoxic T lymphocytes in vivo by liposome-entrapped mRNA. European Journal of Immunology DOI: 10.1002/eji.1830230749 (1993).
NIH Support:
Katalin Karikó: National Heart, Lung, and Blood Institute; National Institute of Neurological Disorders and Stroke
Drew Weissman: National Institute of Allergy and Infectious Diseases; National Institute of Dental and Craniofacial Research; National Heart, Lung, and Blood Institute
Experimental mRNA Vaccine May Protect Against All 20 Influenza Virus Subtypes
Posted on by Lawrence Tabak, D.D.S., Ph.D.

Flu season is now upon us, and protecting yourself and loved ones is still as easy as heading to the nearest pharmacy for your annual flu shot. These vaccines are formulated each year to protect against up to four circulating strains of influenza virus, and they generally do a good job of this. What they can’t do is prevent future outbreaks of more novel flu viruses that occasionally spill over from other species into humans, thereby avoiding a future influenza pandemic.
On this latter and more-challenging front, there’s some encouraging news that was published recently in the journal Science [1]. An NIH-funded team has developed a unique “universal flu vaccine” that, with one seasonal shot, that has the potential to build immune protection against any of the 20 known subtypes of influenza virus and protect against future outbreaks.
While this experimental flu vaccine hasn’t yet been tested in people, the concept has shown great promise in advanced pre-clinical studies. Human clinical trials will hopefully start in the coming year. The researchers don’t expect that this universal flu vaccine will prevent influenza infection altogether. But, like COVID-19 vaccines, the new flu vaccine should help to reduce severe influenza illnesses and deaths when a person does get sick.
So, how does one develop a 20-in-1“multivalent” flu vaccine? It turns out that the key is the same messenger RNA (mRNA) technology that’s enabled two of the safe and effective vaccines against COVID-19, which have been so instrumental in fighting the pandemic. This includes the latest boosters from both Pfizer and Moderna, which now offer updated protection against currently circulating Omicron variants.
While this isn’t the first attempt to develop a universal flu vaccine, past attempts had primarily focused on a limited number of conserved antigens. An antigen is a protein or other substance that produces an immune response. Conserved antigens are those that tend to stay the same over time.
Because conserved antigens will look similar in many different influenza viruses, the hope was that vaccines targeting a small number of them would afford some broad influenza protection. But the focus on a strategy involving few antigens was driven largely by practical limitations. Using traditional methods to produce vaccines by growing flu viruses in eggs and isolating proteins, it simply isn’t feasible to include more than about four targets.
That’s where recent advances in mRNA technology come in. What makes mRNA so nifty for vaccines is that all you need to know is the letters, or sequence, that encodes the genetic material of a virus, including the sequences that get translated into proteins.
A research team led by Scott Hensley, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, recognized that the ease of designing and manufacturing mRNA vaccines opened the door to an alternate approach to developing a universal flu vaccine. Rather than limiting themselves to a few antigens, the researchers could make an all-in-one influenza vaccine, encoding antigens from every known influenza virus subtype.
Influenza vaccines generally target portions of a plentiful protein on the viral surface known as hemagglutinin (H). In earlier work, Hensley’s team, in collaboration with Perelman’s mRNA vaccine pioneer Drew Weissman, showed they could use mRNA technology to produce vaccines with H antigens from single influenza viruses [2, 3]. To protect the fragile mRNA molecules that encode a selected H antigen, researchers deliver them to cells inside well-tolerated microscopic lipid shells, or nanoparticles. The same is true of mRNA COVID-19 vaccines. In their earlier studies, the researchers found that when an mRNA vaccine aimed at one flu virus subtype was given to mice and ferrets in the lab, their cells made the encoded H antigen, eliciting protective antibodies.
In this latest study, they threw antigens from all 20 known flu viruses into the mix. This included H antigens from 18 known types of influenza A and two lineages of influenza B. The goal was to develop a vaccine that could teach the immune system to recognize and respond to any of them.
More study is needed, of course, but early indications are encouraging. The vaccine generated strong and broad antibody responses in animals. Importantly, it worked both in animals with no previous immunity to the flu and in those previously infected with flu viruses. That came as good news because past infections and resulting antibodies sometimes can interfere with the development of new antibodies against related viral subtypes.
In more good news, the researchers found that vaccinated mice and ferrets were protected against severe illness when later challenged with flu viruses. Those viruses included some that were closely matched to antigens in the vaccine, along with some that weren’t.
The findings offer proof-of-principle that mRNA vaccines containing a wide range of antigens can offer broad protection against influenza and likely other viruses as well, including the coronavirus strains responsible for COVID-19. The researchers report that they’re moving toward clinical trials in people, with the goal of beginning an early phase 1 trial in the coming year. The hope is that these developments—driven in part by technological advances and lessons learned over the course of the COVID-19 pandemic—will help to mitigate or perhaps even prevent future pandemics.
References:
[1] A multivalent nucleoside-modified mRNA vaccine against all known influenza virus subtypes. Arevalo CP, Bolton MJ, Le Sage V, Ye N, Furey C, Muramatsu H, Alameh MG, Pardi N, Drapeau EM, Parkhouse K, Garretson T, Morris JS, Moncla LH, Tam YK, Fan SHY, Lakdawala SS, Weissman D, Hensley SE. Science. 2022 Nov 25;378(6622):899-904.
[2] Nucleoside-modified mRNA vaccination partially overcomes maternal antibody inhibition of de novo immune responses in mice. Willis E, Pardi N, Parkhouse K, Mui BL, Tam YK, Weissman D, Hensley SE. Sci Transl Med. 2020 Jan 8;12(525):eaav5701.
[3] Nucleoside-modified mRNA immunization elicits influenza virus hemagglutinin stalk-specific antibodies. Pardi N, Parkhouse K, Kirkpatrick E, McMahon M, Zost SJ, Mui BL, Tam YK, Karikó K, Barbosa CJ, Madden TD, Hope MJ, Krammer F, Hensley SE, Weissman D. Nat Commun. 2018 Aug 22;9(1):3361.
Links:
Understanding Flu Viruses (Centers for Disease Control and Prevention, Atlanta)
COVID Research (NIH)
Decades in the Making: mRNA COVID-19 Vaccines (NIH)
Video: mRNA Flu Vaccines: Preventing the Next Pandemic (Penn Medicine, Philadelphia)
Scott Hensley (Perelman School of Medicine at the University of Pennsylvania, Philadelphia)
Weissman Lab (Perelman School of Medicine)
Video: The Story Behind mRNA COVID Vaccines: Katalin Karikó and Drew Weissman (Penn Medicine, Philadelphia)
NIH Support: National Institute for Allergy and Infectious Diseases
Millions of Single-Cell Analyses Yield Most Comprehensive Human Cell Atlas Yet
Posted on by Lawrence Tabak, D.D.S., Ph.D.

There are 37 trillion or so cells in our bodies that work together to give us life. But it may surprise you that we still haven’t put a good number on how many distinct cell types there are within those trillions of cells.
That’s why in 2016, a team of researchers from around the globe launched a historic project called the Human Cell Atlas (HCA) consortium to identify and define the hundreds of presumed distinct cell types in our bodies. Knowing where each cell type resides in the body, and which genes each one turns on or off to create its own unique molecular identity, will revolutionize our studies of human biology and medicine across the board.
Since its launch, the HCA has progressed rapidly. In fact, it has already reached an important milestone with the recent publication in the journal Science of four studies that, together, comprise the first multi-tissue drafts of the human cell atlas. This draft, based on analyses of millions of cells, defines more than 500 different cell types in more than 30 human tissues. A second draft, with even finer definition, is already in the works.
Making the HCA possible are recent technological advances in RNA sequencing. RNA sequencing is a topic that’s been mentioned frequently on this blog in a range of research areas, from neuroscience to skin rashes. Researchers use it to detect and analyze all the messenger RNA (mRNA) molecules in a biological sample, in this case individual human cells from a wide range of tissues, organs, and individuals who voluntarily donated their tissues.
By quantifying these RNA messages, researchers can capture the thousands of genes that any given cell actively expresses at any one time. These precise gene expression profiles can be used to catalogue cells from throughout the body and understand the important similarities and differences among them.
In one of the published studies, funded in part by the NIH, a team co-led by Aviv Regev, a founding co-chair of the consortium at the Broad Institute of MIT and Harvard, Cambridge, MA, established a framework for multi-tissue human cell atlases [1]. (Regev is now on leave from the Broad Institute and MIT and has recently moved to Genentech Research and Early Development, South San Francisco, CA.)
Among its many advances, Regev’s team optimized single-cell RNA sequencing for use on cell nuclei isolated from frozen tissue. This technological advance paved the way for single-cell analyses of the vast numbers of samples that are stored in research collections and freezers all around the world.
Using their new pipeline, Regev and team built an atlas including more than 200,000 single-cell RNA sequence profiles from eight tissue types collected from 16 individuals. These samples were archived earlier by NIH’s Genotype-Tissue Expression (GTEx) project. The team’s data revealed unexpected differences among cell types but surprising similarities, too.
For example, they found that genetic profiles seen in muscle cells were also present in connective tissue cells in the lungs. Using novel machine learning approaches to help make sense of their data, they’ve linked the cells in their atlases with thousands of genetic diseases and traits to identify cell types and genetic profiles that may contribute to a wide range of human conditions.
By cross-referencing 6,000 genes previously implicated in causing specific genetic disorders with their single-cell genetic profiles, they identified new cell types that may play unexpected roles. For instance, they found some non-muscle cells that may play a role in muscular dystrophy, a group of conditions in which muscles progressively weaken. More research will be needed to make sense of these fascinating, but vital, discoveries.
The team also compared genes that are more active in specific cell types to genes with previously identified links to more complex conditions. Again, their data surprised them. They identified new cell types that may play a role in conditions such as heart disease and inflammatory bowel disease.
Two of the other papers, one of which was funded in part by NIH, explored the immune system, especially the similarities and differences among immune cells that reside in specific tissues, such as scavenging macrophages [2,3] This is a critical area of study. Most of our understanding of the immune system comes from immune cells that circulate in the bloodstream, not these resident macrophages and other immune cells.
These immune cell atlases, which are still first drafts, already provide an invaluable resource toward designing new treatments to bolster immune responses, such as vaccines and anti-cancer treatments. They also may have implications for understanding what goes wrong in various autoimmune conditions.
Scientists have been working for more than 150 years to characterize the trillions of cells in our bodies. Thanks to this timely effort and its advances in describing and cataloguing cell types, we now have a much better foundation for understanding these fundamental units of the human body.
But the latest data are just the tip of the iceberg, with vast flows of biological information from throughout the human body surely to be released in the years ahead. And while consortium members continue making history, their hard work to date is freely available to the scientific community to explore critical biological questions with far-reaching implications for human health and disease.
References:
[1] Single-nucleus cross-tissue molecular reference maps toward understanding disease gene function. Eraslan G, Drokhlyansky E, Anand S, Fiskin E, Subramanian A, Segrè AV, Aguet F, Rozenblatt-Rosen O, Ardlie KG, Regev A, et al. Science. 2022 May 13;376(6594):eabl4290.
[2] Cross-tissue immune cell analysis reveals tissue-specific features in humans. Domínguez Conde C, Xu C, Jarvis LB, Rainbow DB, Farber DL, Saeb-Parsy K, Jones JL,Teichmann SA, et al. Science. 2022 May 13;376(6594):eabl5197.
[3] Mapping the developing human immune system across organs. Suo C, Dann E, Goh I, Jardine L, Marioni JC, Clatworthy MR, Haniffa M, Teichmann SA, et al. Science. 2022 May 12:eabo0510.
Links:
Ribonucleic acid (RNA) (National Human Genome Research Institute/NIH)
Studying Cells (National Institute of General Medical Sciences/NIH)
Regev Lab (Broad Institute of MIT and Harvard, Cambridge, MA)
NIH Support: Common Fund; National Cancer Institute; National Human Genome Research Institute; National Heart, Lung, and Blood Institute; National Institute on Drug Abuse; National Institute of Mental Health; National Institute on Aging; National Institute of Allergy and Infectious Diseases; National Institute of Neurological Disorders and Stroke; National Eye Institute
Teaching the Immune System to Attack Cancer with Greater Precision
Posted on by Dr. Francis Collins

To protect humans from COVID-19, the Pfizer and Moderna mRNA vaccines program human cells to translate the injected synthetic messenger RNA into the coronavirus spike protein, which then primes the immune system to arm itself against future appearances of that protein. It turns out that the immune system can also be trained to spot and attack distinctive proteins on cancer cells, killing them and leaving healthy cells potentially untouched.
While these precision cancer vaccines remain experimental, researchers continue to make basic discoveries that move the field forward. That includes a recent NIH-funded study in mice that helps to refine the selection of protein targets on tumors as a way to boost the immune response [1]. To enable this boost, the researchers first had to discover a possible solution to a longstanding challenge in developing precision cancer vaccines: T cell exhaustion.
The term refers to the immune system’s complement of T cells and their capacity to learn to recognize foreign proteins, also known as neoantigens, and attack them on cancer cells to shrink tumors. But these responding T cells can exhaust themselves attacking tumors, limiting the immune response and making its benefits short-lived.
In this latest study, published in the journal Cell, Tyler Jacks and Megan Burger, Massachusetts Institute of Technology, Cambridge, help to explain this phenomenon of T cell exhaustion. The researchers found in mice with lung tumors that the immune system initially responds as it should. It produces lots of T cells that target many different cancer-specific proteins.
Yet there’s a problem: various subsets of T cells get in each other’s way. They compete until, eventually, one of those subsets becomes the dominant T cell type. Even when those dominant T cells grow exhausted, they still remain in the tumor and keep out other T cells, which might otherwise attack different neoantigens in the cancer.
Building on this basic discovery, the researchers came up with a strategy for developing cancer vaccines that can “awaken” T cells and reinvigorate the body’s natural cancer-fighting abilities. The strategy might seem counterintuitive. The researchers vaccinated mice with neoantigens that provide a weak but encouraging signal to the immune cells responsible for presenting the distinctive cancer protein target, or antigen, to T cells. It’s those T cells that tend to get suppressed in competition with other T cells.
When the researchers vaccinated the mice with one of those neoantigens, the otherwise suppressed T cells grew in numbers and better targeted the tumor. What’s more, the tumors shrank by more than 25 percent on average.
Research on this new strategy remains in its early stages. The researchers hope to learn if this approach to cancer vaccines might work even better when used in combination with immunotherapy drugs, which unleash the immune system against cancer in other ways.
It’s also possible that the recent and revolutionary success of mRNA vaccines for preventing COVID-19 actually could help. An important advantage of mRNA is that it’s easy for researchers to synthesize once they know the specific nucleic acid sequence of a protein target, and they can even combine different mRNA sequences to make a multiplex vaccine that primes the immune system to recognize multiple neoantigens. Now that we’ve seen how well mRNA vaccines work to prompt a desired immune response against COVID-19, this same technology can be used to speed the development and testing of future vaccines, including those designed precisely to fight cancer.
Reference:
[1] Antigen dominance hierarchies shape TCF1+ progenitor CD8 T cell phenotypes in tumors. Burger ML, Cruz AM, Crossland GE, Gaglia G, Ritch CC, Blatt SE, Bhutkar A, Canner D, Kienka T, Tavana SZ, Barandiaran AL, Garmilla A, Schenkel JM, Hillman M, de Los Rios Kobara I, Li A, Jaeger AM, Hwang WL, Westcott PMK, Manos MP, Holovatska MM, Hodi FS, Regev A, Santagata S, Jacks T. Cell. 2021 Sep 16;184(19):4996-5014.e26.
Links:
Cancer Treatment Vaccines (National Cancer Institute/NIH)
The Jacks Lab (Massachusetts Institute of Technology, Cambridge)
NIH Support: National Cancer Institute; National Heart, Lung, and Blood Institute
Meet an Inspiring Researcher Who Helped Create COVID-19 mRNA Vaccines
Posted on by Dr. Francis Collins
More than 170 million Americans already have received COVID-19 vaccines. As this number continues to grow and expand to younger age groups, I’m filled with overwhelming gratitude for all of the researchers who worked so diligently, over the course of decades, to build the scientific foundation for these life-saving vaccines. One of them is Dr. Kizzmekia Corbett, who played a central role in the fact that, in the span of less than a year, we were able to develop safe and effective mRNA-based vaccines to protect against this devastating infectious disease.
As leader of the immunopathogenesis team at NIH’s Dale and Betty Bumpers Vaccine Research Center in Bethesda, MD, Dr. Corbett was ready, willing, and able when the COVID-19 pandemic emerged to take the critical first steps in developing what would become the Moderna and Pfizer/BioNTech mRNA vaccines. Recently, she accepted a position at Harvard University T.H. Chan School of Public Health, Boston, where she will soon open her own viral immunology lab to help inform future vaccine development for coronaviruses and other respiratory viruses.
While she was preparing for her move to Harvard, I had a chance to speak with Dr. Corbett about her COVID-19 research experience and what it was like to get immunized with the vaccine that she helped to create. Our conversation was part of an NIH Facebook Live event in which we connected virtually from our homes in Maryland. Here is a condensed version of our chat.
Collins: You’ve studied SARS, MERS, and other coronaviruses for many years. Then, in early January 2020, like all of us, you heard that something was going on that sounded worrisome in Wuhan, China. What did you think?
Corbett: Well, the story actually began for me on December 31, 2019. My boss Dr. Barney Graham sent me an email at 6 a.m. that said: “Get ready for 2020.” There had been some news of a respiratory virus outbreak in the Wuhan district of China. I honestly wrote it off as probably a strain of the flu. Then, we got back to NIH after the holidays, and it was determined around January 6 that the virus was for certain a coronavirus. That meant our team would be responding to it.
We sat down and planned to monitor the situation very closely. We knew exactly what to do, based on our past work. We would go into full force to make a vaccine—the one now known as “the Moderna vaccine” —as quickly as possible for testing in a clinical trial. The goal was to make the vaccine in 100 days. And so when the genetic sequence of this new virus came out on January 10, I sprung out of bed and so did everyone on the team. It’s been kind of a whirlwind ever since.
Collins: Tell us a little bit more about that. The sequence got posted on the internet by a Chinese scientist. So you have this sequence, and everyone gathers in NIH’s Vaccine Research Center. Then what happens?
Corbett: The cool thing about this type of technology is you don’t even need the lab to design the vaccine. All you need are the letters, or sequence, that encodes the virus’ genetic material displayed on your computer screen. We could actually do the work from our homes, obviously in close conversation with each other.
This sequence is the virus’s genetic code. Just like humans have families—brothers, sisters, cousins—viruses also have families. So, we could see when looking at the sequence of letters, how similar this particular virus was to viruses that we’ve worked with before in the coronavirus family. It was almost like “A-ha! This is the part of the sequence that represents the protein on the surface of the virus.”
We knew that we could take the sequence of that surface protein and use all of the knowledge that we had from previous years to design a vaccine. And that’s what we did. We took that sequence on our computer screen and said we said this is exactly how we want this vaccine to look. The process was as straightforward as that.
Collins: In other words, you already knew that these coronaviruses have spike proteins on their surface and that’s the thing that’s going to be really useful for making an antibody. You’d already taken this approach in developing a vaccine for MERS, right?
Corbett: Exactly, we’d done that for MERS. Vaccines are basically a way to teach your body how to see a pathogen. Over the years, as vaccinology and technology have progressed, different scientists have figured out that you don’t really need the whole virus as a part of the vaccine. You can just take a small portion of that virus to alert your body.
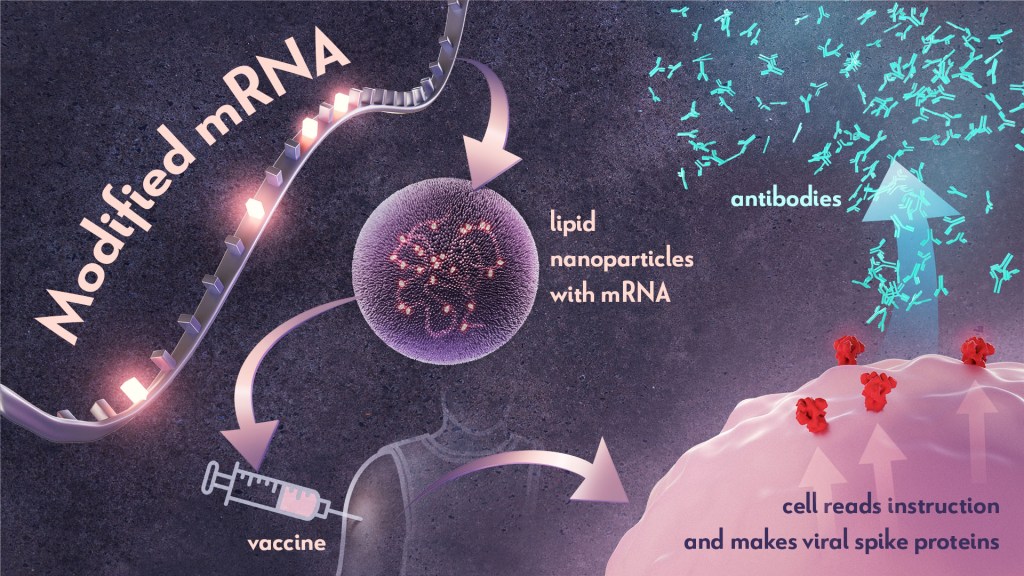
In this case, taking the spike protein and teaching your immune system how to specifically spot and attack it, you can now protect yourself from COVID-19. So, we used the sequence of that spike protein, with some modifications to make it much better as a vaccine. We then deliver that to you as a message—messenger RNA (mRNA) —to get your muscle cells briefly to make the spike protein. Then, your body sees that spike protein hanging out on your cells and makes a really specific immune response to it. That way the next time your body sees the spike protein, if you ever come into contact with the virus, your immune system is armed and ready to attack.
Collins: Say more about this messenger RNA approach. It’s been so revolutionary and one of the reasons that we got vaccines into people’s arms in just 11 months. Had this approach ever been used before?
Corbett: Yes, messenger RNA technologies have been in development from a basic science perspective for over 15 years. A lot of that work was funded by NIH. Soon after I got to NIH, I attended a meeting in London called Transforming Vaccinology. At the time, Moderna was a smaller company that was working to make messenger RNA technologies, mostly centered around cancer therapies. But they had started to test some flu vaccines that used messenger RNA. My question to the presenter was: “Every single time I see you guys present, it looks like mRNA technology has always worked. Can you tell me a time that it hasn’t?” And he said, “I can’t.”
So, our understanding of how this technology works to make really good vaccines predates this pandemic. I think one of the worries that many people have is how fast and how new this technology is. But all science is compounded knowledge—everything builds on itself.
Collins: Right! We only learned about messenger RNA, because back in the 1950s and 1960s, some researchers decided to figure out how the information in our genetic instruction book, our DNA, can ultimately turn into proteins. It turned out that the message that carries that information is made of RNA.
So, you knew which kinds of letters to program into the messenger RNA vaccine. Would you explain how this vaccine, its messenger RNA, produces a spike protein. Where does that step happen?
Corbett: Your cells are machines built for this kind of thing. I like to remind people that, on a day-in, day-out basis, our cells make proteins—all of the hormones and other things our bodies needs to survive. So, we’re not teaching the cells to do anything different than they would normally do. That’s important to understand.
The way that cells do this is by reading the mRNA sequence. As they’re reading that sequence, they chew it up, like eating it, and say, “Okay, this sequence is for this very specific protein.” Then, they make that protein and push it to the surface of your cells. That’s how it happens.
Collins: And for mRNA vaccines, that’s the point when your immune system says “Wait a minute! I don’t recognize that as part of me, so I’ve got to make an antibody to it.” Then you’re off to the races and develop your immunity. Now that this mRNA vaccine strategy has succeeded for COVID-19, could it be applied to other infectious diseases or even non-infectious conditions?
Corbett: Yes, I heard that about 60 new companies have sprouted up in the last year around messenger RNA technology. They have ideas for different types of infectious disease vaccines and cancer therapies. I expect that this technology will be transformative to medicine in general.
Collins: Here’s a question from social media: “Why does it take two shots for the Pfizer and the Moderna mRNA vaccines? Why isn’t one good enough?”
Corbett: The way that these vaccines work is much like an alarm clock. Imagine your immune system is in bed and the first shot is the alarm clock going off to say, “Hey, wake up and get ready.” And just like I did this morning, the immune system pressed snooze and took a little nap. But when you hear the alarm clock the second time, it’s like someone rushing into your room and pouring a cold bucket of water on you. You have no choice but to get out of bed.
That’s what the second dose of the vaccine does. It pushes your immune response to the next level. That’s why you need two shots to get the type of efficacy that you want and be fully protected for the optimal immune response.
Collins: You were a co-leader of the team that created what became the Moderna vaccine—and you ended up getting immunized with the Moderna vaccine. What did that feel like?
Corbett: It was pretty surreal. I cried. At the end of it, I felt a lot of relief after getting my vaccine, particularly after getting the second dose. There was this breath of fresh air. It was also a birthday present. I got my second dose the day before my 35th birthday, as a birthday present to myself.
Collins: I have to admit, I cried a little bit too after my second dose. It’s just the sense of relief and incredible gratitude that we’ve reached this point. Here we are with vaccines that have 95 percent effectiveness and an incredibly good safety record, which is almost better than we could have hoped for. I’m a person of faith, so there were a lot of my prayers that went into this and it sure felt like they got answered.
Corbett: Yes, same.
Collins: You are out there a lot talking to people about the vaccines. There are still about 100 million Americans that have not yet received their first dose. Many of them still unsure about getting vaccinated. What do you say to those who are on the fence?
Corbett: In this past year, I’ve spent a lot of time talking about the vaccine with people in the community. One thing that I realized, is that I don’t need to say anything unless I’m asked. I think it’s important that I listen first, instead of just speaking.
So I do that, and I try to answer people’s inquiries as specifically as possible. But people have some very broad questions. One thing that is happening is people are seeing vaccines being developed right before their eyes. That can be a little confusing. I try to explain the process, how we went from the preclinical stage all the way to the point of getting the vaccine to hundreds of millions of people. I explain how each step along the way is very highly vetted by regulatory agencies and data safety monitoring committees. I also tell them that the monitoring continues. People from the clinical trials are still being evaluated, and there’s monitoring in the real world as the vaccine is being rolled out. I think that all of those things are really important for people to know.
Collins: Another question from social media: “As a successful scientist, what advice would you give to people who are thinking about a career in science?”
Corbett: If you think you’re interested, you just have to start. There are internship programs, there are scholarship programs, there are shadowing programs all over this country and even globally that can help you get your feet wet. I think the first thing that you want to do with any career is to figure out whether or not you like it. The only way that you can do that is to just explore, explore, explore.
Collins: Didn’t you kind of roll up your sleeves and take the plunge at a young age?
Corbett: Yes, at age 16, I went off and did summer internships at the University of North Carolina. I was able to see first-hand the day-to-day life of science and what being a scientist would look like. That was really important for me. That’s what I mean by exploring.
Collins: And a follow-up question: “Is the biomedical research community welcoming to women of color?”
Corbett: Not always, frankly. I was very fortunate to have been under the wings of a lot of mentors and advocates, who have helped to advance my career to where it is now. I had great mentors at NIH. My graduate school mentor was amazing, and my main collaborator in the coronavirus field was on my dissertation committee. Even prior to this pandemic, when I was doing work that was very obscure, he checked on me very often and made sure that he had a sense of where I wanted to go and how he could help me get there, including collaborating with me.
That kind of thing is very important, particularly for women of color or anyone from a marginalized community. That’s because there will be a point where there might be a glass ceiling. Unfortunately, we don’t necessarily have the tools to break those just yet. So, someone else is going to have to break those down, and most often than not, that person is going to have to be a white man. Finding those people who are allies with you and joining in your fight for your career trajectory is very helpful.
I remember when I was choosing a college, it was a very difficult decision for me. I got accepted into Ivy League schools, and I’d gone to all of the scholarship weekends all over the country. When I was making the decision, my dad said, “Kizzy, just always go where there is love.”
That really sticks to me with every single choice that I make around my career. You want to be at a place that’s welcoming, a place that understands you, and a place that fosters the next version of who you are destined to be. You need to make sure to step back outside of the day-to-day stuff and say, “Okay, does this place love me and people like me?” It’s important to remember that’s how you thrive: when you are comfortable in and in love with your environment.
Collins: Yes, we have to move our scientific workforce into a place where it is not necessary for a white man to advocate for a talented Black woman. There’s something very wrong with that particular circumstance. As NIH Director, I want to assure you, we are motivated more than ever to change that, including through a new initiative called UNITE. We’re missing out on welcoming the talents of so many folks who currently don’t see our research agenda as theirs, and we need to change that.
Kizzmekia, this has been a lot of fun. Thank you for giving us a half-hour of your time when you’re in the midst of this crazy two-week period of moving from Bethesda to Boston. We wish you the very best for this next chapter, which I know is going to be just amazing.
Corbett: Thank you so much.
Links:
Video: COVID-19 mRNA Vaccine Q & A – Kizzmekia Corbett and Francis Collins (NIH)
Video: Lead COVID-19 scientist Kizzmekia Corbett to join Harvard Chan School faculty (Harvard University, Boston)
COVID-19 Research (NIH)
Dale and Betty Bumpers Vaccine Research Center (National Institute of Allergy and Infectious Diseases/NIH)
UNITE Initiative (NIH)
CRISPR-Based Anti-Viral Therapy Could One Day Foil the Flu—and COVID-19
Posted on by Dr. Francis Collins

CRISPR gene-editing technology has tremendous potential for making non-heritable DNA changes that can treat or even cure a wide range of devastating disorders, from HIV to muscular dystrophy Now, a recent animal study shows that another CRISPR system—targeting viral RNA instead of human DNA—could work as an inhaled anti-viral therapeutic that can be preprogrammed to seek out and foil potentially almost any flu strain and many other respiratory viruses, including SARS-CoV-2, the coronavirus that causes COVID-19.
How can that be? Other CRISPR gene-editing systems rely on a sequence-specific guide RNA to direct a scissor-like, bacterial enzyme (Cas9) to just the right spot in the genome to cut out, replace, or repair disease-causing mutations. This new anti-viral CRISPR system also relies on guide RNA. But the guide instead directs a different bacterial enzyme, called Cas13a, to the right spot in the viral genome to bind and cleave viral RNA and stop viruses from replicating in lung cells.
The findings, recently published in the journal Nature Biotechnology [1], come from the lab of Philip Santangelo, Georgia Institute of Technology and Emory University, Atlanta. Earlier studies by other groups had shown the potential of Cas13 for degrading the RNA of influenza viruses in a lab dish [2,3]. In this latest work, Santangelo and colleagues turned to mice and hamsters to see whether this enzyme could actually work in the lung tissue of a living animal.
What’s interesting is how Santangelo’s team did it. Rather than delivering the Cas13a protein itself to the lungs, the CRISPR system works by supplying a messenger RNA (mRNA) with the instructions to make the anti-viral Cas13a protein. This is the same idea as the Pfizer and Moderna mRNA-based COVID-19 vaccines, which temporarily direct your muscle cells to produce viral spike proteins that launch an immune response. In this case, the lung cells translate the Cas13a mRNA to produce the protein. Directed by the guide RNA that was also delivered to the same cells, Cas13a degrades the viral RNA and stops the infection. Because mRNA doesn’t enter the cell’s nucleus, it doesn’t interact with DNA and raise potential concerns about causing unwanted genetic changes.
The researchers designed guide RNAs that were specific to a shared, highly conserved portion of influenza viruses involved in replicating their genome and infecting other cells. They also designed another set directed to key portions of SARS-CoV-2.
Next, they delivered the Cas13a mRNA and guides straight to the lungs of animals using an adapted nebulizer, just like those used to deliver medicines to the lungs of people. In mice with influenza, Cas13a degraded influenza RNA in the lungs and the animals recovered without any apparent side effects. In SARS-CoV-2-infected hamsters, the same approach limited the virus’s ability to replicate in cells as the animals COVID-19-like symptoms improved.
The findings are the first to show that mRNA can be used to express the Cas13a protein in living lung tissue, not just in cells in a dish. It’s also the first to show that the bacterial Cas13a protein is effective at slowing or stopping replication of SARS-CoV-2. The latter raises hope that this CRISPR system could be quickly adapted to fight any future novel coronaviruses that develop the ability to infect humans.
The researchers report that this approach has potential to work against the vast majority—99 percent—of the flu strains that have circulated around the world over the last century. It also should be equally effective against the new and more contagious variants of SARS-CoV-2 now circulating around the globe. While more study is needed to understand the safety of such an anti-viral approach before trying it in humans, what’s clear is basic research advances like this one hold great potential for helping us to fight life-threatening respiratory viruses of the past, present, and future.
References:
[1] Treatment of influenza and SARS-CoV-2 infections via mRNA-encoded Cas13a in rodents. Blanchard EL, Vanover D, Bawage SS, Tiwari PM, Rotolo L, Beyersdorf J, Peck HE, Bruno NC, Hincapie R, Michel F, Murray J, Sadhwani H, Vanderheyden B, Finn MG, Brinton MA, Lafontaine ER, Hogan RJ, Zurla C, Santangelo PJ. Nat Biotechnol. 2021 Feb 3. [Published online ahead of print.]
[2] Programmable inhibition and detection of RNA viruses using Cas13. Freije CA, Myhrvold C, Boehm CK, Lin AE, Welch NL, Carter A, Metsky HC, Luo CY, Abudayyeh OO, Gootenberg JS, Yozwiak NL, Zhang F, Sabeti PC. Mol Cell. 2019 Dec 5;76(5):826-837.e11.
[3] Development of CRISPR as an antiviral strategy to combat SARS-CoV-2 and influenza. Abbott TR, Dhamdhere G, Liu Y, Lin X, Goudy L, Zeng L, Chemparathy A, Chmura S, Heaton NS, Debs R, Pande T, Endy D, La Russa MF, Lewis DB, Qi LS. Cell. 2020 May 14;181(4):865-876.e12.
Links:
COVID-19 Research (NIH)
Influenza (National Institute of Allergy and Infectious Diseases/NIH)
Santangelo Lab (Georgia Institute of Technology, Atlanta)
On-the-Spot Gene Readouts Offer Clues to How Cells Work
Posted on by Dr. Francis Collins

Just as two companies can merge to expand their capabilities, two technologies can become more powerful when integrated into one. That’s why researchers recently merged two breakthrough technologies into one super powerful new method called ExSeq. The two-in-one technology enables researchers for the first time to study an intact tissue sample and track genetic activity on the spot within a cell’s tiniest recesses, or microenvironments—areas that have been largely out of reach until now.
ExSeq, which is described in a paper in the journal Science [1], will unleash many new experimental applications. Beyond enabling more precise analysis of the basic building blocks of life, these applications include analyzing tumor biopsies more comprehensively and even unlocking mysteries of how the brain works. The latter use is on display in this colorful cross-section of a mouse’s hippocampus, a region of the brain involved in the memory of facts and events.
Here you can see in precise and unprecedented detail the areas where genes are activated (magenta) in the brain’s neurons (green). In this particular example, the genes are working within subregions of the hippocampus called the CA1 and dentate gyrus regions (white, bottom and top left).
ExSeq is a joint effort from NIH grantees Ed Boyden, Massachusetts Institute of Technology (MIT), Cambridge, and George Church, Harvard Medical School, Boston. The new method combines a technology called tissue expansion with an in situ sequencing approach.
Tissue expansion swells the contents of tissue sections up to 100 times their normal size but retains their same physical structure [2]. It’s sort of like increasing the font size and line spacing on a hard-to-read document. It makes cellular details that were outside the resolution range of the light microscope suddenly accessible.
With the information inside cells now easier to see, the next step involves a technique called FISSEQ (fluorescent in situ sequencing), which generates readouts of thousands of mRNA molecules in cells [3]. FISSEQ works by detecting individual RNA molecules where they are inside cells and amplifying them into “nanoballs,” or rolled-up copies of themselves. Each nanoball can be read using standard sequencing methods and a fluorescence microscope.
Using the combined ExSeq approach, the team can analyze precisely where gene activity changes within tiny cellular microenvironments. Or, it can compile a more-comprehensive readout of gene activity within cells by analyzing as many gene readouts as detectable. When used in the hippocampus, this untargeted, “agnostic” approach led to some surprises—revealing unusual forms of RNA and, by association, genes for proteins not previously linked with communication between neurons.
Like many technology developments, the scientists envision that ExSeq can be used in many ways, including for more precise analysis of tumor biopsies. To illustrate this point, the researchers analyzed breast cancer metastases, which are cells from breast tumors that have spread to other areas in the body. Metastases contain many different cell types, including cancer cells and immune cells.
Using ExSeq, Boyden and Church learned that these distinct cell types can behave differently depending on where they are inside a tumor. They discovered, for example, that immune B cells near tumor cells expressed certain inflammatory genes at a higher level than immune B cells that were further away. Precise information about a tumor’s composition and activity may lead to development of more targeted approaches to attack it.
Many discoveries come on the heels of transformative new technologies. ExSeq shines a much brighter light on the world of the very small. And that should help us better understand how different parts of cells work together, as well as how cells work with each other in the brain, in cancer, and throughout the body.
References:
[1] Expansion sequencing: Spatially precise in situ transcriptomics in intact biological systems. Alon S, Goodwin DR, Sinha A, Wassie AT, et al. Science. 2021 Jan 29;37:eaax2656.
[2] Expansion microscopy. Chen F, Tillberg PW, Boyden ES. Science. 2015;347:543-548.
[3]. Highly multiplexed subcellular RNA sequencing in situ. Lee JH, Daugharthy ER, Scheiman J, Kalhor R, et al. Science. 2014;343:1360-1363.
Links:
Ribonucleic Acid (RNA) (National Human Genome Research Institute/NIH)
Synthetic Neurobiology Group (Massachusetts Institute of Technology, Cambridge)
George Church (Harvard Medical School, Boston)
NIH Support: National Human Genome Research Institute; National Cancer Institute; National Institute of Biomedical Imaging and Bioengineering; National Institute of Mental Health; National Institute of Neurological Disorders and Stroke
Nanoparticle Technology Holds Promise for Protecting Against Many Coronavirus Strains at Once
Posted on by Dr. Francis Collins

It’s truly encouraging to witness people all across our nation rolling up their sleeves to get their COVID-19 vaccines. That is our best chance to end this pandemic. But this is the third coronavirus to emerge and cause serious human illness in the last 20 years, and it’s probably not the last. So, this is also an opportunity to step up our efforts to develop vaccines to combat future strains of disease-causing coronavirus. With this in mind, I’m heartened by a new NIH-funded study showing the potential of a remarkably adaptable, nanoparticle-based approach to coronavirus vaccine development [1].
Both COVID-19 vaccines currently authorized for human use by the Food and Drug Administration (FDA) work by using mRNA to instruct our cells to make an essential portion of the spike protein of SARS-CoV-2, which is the novel coronavirus that causes COVID-19. As our immune system learns to recognize this protein fragment as foreign, it produces antibodies to attack SARS-CoV-2 and prevent COVID-19. What makes the new vaccine technology so powerful is that it raises the possibility of training the immune system to recognize not just one strain of coronavirus—but up to eight—with a single shot.
This approach has not yet been tested in people, but when a research team, led by Pamela Bjorkman, California Institute of Technology, Pasadena, injected this new type of vaccine into mice, it spurred the production of antibodies that react to a variety of different coronaviruses. In fact, some of the mouse antibodies proved to be reactive to related strains of coronavirus that weren’t even represented in the vaccine. These findings suggest that if presented with multiple different fragments of the spike protein’s receptor binding domain (RBD), which is what SARS-like coronaviruses use to infect human cells, the immune system may learn to recognize common features that might protect against as-yet unknown, newly emerging coronaviruses.
This new work, published in the journal Science, utilizes a technology called a mosaic nanoparticle vaccine platform [1]. Originally developed by collaborators at the University of Oxford, United Kingdom, the nanoparticle component of the platform is a “cage” made up of 60 identical proteins. Each of those proteins has a small protein tag that functions much like a piece of Velcro®. In their SARS-CoV-2 work, Bjorkman and her colleagues, including graduate student Alex A. Cohen, engineered multiple different fragments of the spike protein so each had its own Velcro-like tag. When mixed with the nanoparticle, the spike protein fragments stuck to the cage, resulting in a vaccine nanoparticle with spikes representing four to eight distinct coronavirus strains on its surface. In this instance, the researchers chose spike protein fragments from several different strains of SARS-CoV-2, as well as from other related bat coronaviruses thought to pose a threat to humans.
The researchers then injected the vaccine nanoparticles into mice and the results were encouraging. After inoculation, the mice began producing antibodies that could neutralize many different strains of coronavirus. In fact, while more study is needed to understand the mechanisms, the antibodies responded to coronavirus strains that weren’t even represented on the mosaic nanoparticle. Importantly, this broad antibody response came without apparent loss in the antibodies’ ability to respond to any one particular coronavirus strain.
The findings raise the exciting possibility that this new vaccine technology could provide protection against many coronavirus strains with a single shot. Of course, far more study is needed to explore how well such vaccines work to protect animals against infection, and whether they will prove to be safe and effective in people. There will also be significant challenges in scaling up manufacturing. Our goal is not to replace the mRNA COVID-19 vaccines that scientists developed at such a remarkable pace over the last year, but to provide much-needed vaccine strategies and tools to respond swiftly to the emerging coronavirus strains of the future.
As we double down on efforts to combat COVID-19, we must also come to grips with the fact that SARS-CoV-2 isn’t the first—and surely won’t be the last—novel coronavirus to cause disease in humans. With continued research and development of new technologies such as this one, the hope is that we will come out of this terrible pandemic better prepared for future infectious disease threats.
References:
[1] Mosaic RBD nanoparticles elicit neutralizing antibodies against SARS-CoV-2 and zoonotic coronaviruses. Cohen AA, Gnanapragasam PNP, Lee YE, Hoffman PR, Ou S, Kakutani LM, Keeffe JR, Barnes CO, Nussenzweig MC, Bjorkman PJ. Science. 2021 Jan 12.
Links:
COVID-19 Research (NIH)
Bjorkman Lab (California Institute of Technology, Pasadena)
NIH Support: National Institute of Allergy and Infectious Diseases
Celebrating the Gift of COVID-19 Vaccines
Posted on by Dr. Francis Collins

The winter holidays are traditionally a time of gift-giving. As fatiguing as 2020 and the COVID-19 pandemic have been, science has stepped up this year to provide humankind with a pair of truly hopeful gifts: the first two COVID-19 vaccines.
Two weeks ago, the U.S. Food and Drug Administration (FDA) granted emergency use authorization (EUA) to a COVID-19 vaccine from Pfizer/BioNTech, enabling distribution to begin to certain high-risk groups just three days later. More recently, the FDA granted an EUA to a COVID-19 vaccine from the biotechnology company Moderna, Cambridge, MA. This messenger RNA (mRNA) vaccine, which is part of a new approach to vaccination, was co-developed by NIH’s National Institute of Allergy and Infectious Diseases (NIAID). The EUA is based on data showing the vaccine is safe and 94.5 percent effective at protecting people from infection with SARS-CoV-2, the coronavirus that causes COVID-19.
Those data on the Moderna vaccine come from a clinical trial of 30,000 individuals, who generously participated to help others. We can’t thank those trial participants enough for this gift. The distribution of millions of Moderna vaccine doses is expected to begin this week.
It’s hard to put into words just how remarkable these accomplishments are in the history of science. A vaccine development process that used to take many years, often decades, has been condensed to about 11 months. Just last January, researchers started out with a previously unknown virus and we now have not just one, but two, vaccines that will be administered to millions of Americans before year’s end. And the accomplishments don’t end there—several other types of COVID-19 vaccines are also on the way.
It’s important to recognize that this couldn’t have happened without the efforts of many scientists working tirelessly behind the scenes for many years prior to the pandemic. Among those who deserve tremendous credit are Kizzmekia Corbett, Barney Graham, John Mascola, and other members of the amazing team at the Dale and Betty Bumpers Vaccine Research Center at NIH’s National Institute of Allergy and Infectious Diseases (NIAID).
When word of SARS-CoV-2 emerged, Corbett, Graham, and other NIAID researchers had already been studying other coronaviruses for years, including those responsible for earlier outbreaks of respiratory disease. So, when word came that this was a new coronavirus outbreak, they were ready to take action. It helped that they had paid special attention to the spike proteins on the surface of coronaviruses, which have turned out to be the main focus the COVID-19 vaccines now under development.
The two vaccines currently authorized for administration in the United States work in a unique way. Their centerpiece is a small, non-infectious snippet of mRNA. Our cells constantly produce thousands of mRNAs, which provide the instructions needed to make proteins. When someone receives an mRNA vaccine for COVID-19, it tells the person’s own cells to make the SARS-CoV-2 spike protein. The person’s immune system then recognizes the viral spike protein as foreign and produces antibodies to eliminate it.
This vaccine-spurred encounter trains the human immune system to remember the spike protein. So, if an actual SARS-CoV-2 virus tries to infect a vaccinated person weeks or months later, his or her immune system will be ready to fend it off. To produce the most vigorous and durable immunity against the virus, people will need to get two shots of mRNA vaccine, which are spaced several weeks to a month apart, depending on the vaccine.
Some have raised concerns on social media that mRNA vaccines might alter the DNA genome of someone being vaccinated. But that’s not possible, since this mRNA doesn’t enter the nucleus of the cell where DNA is located. Instead, the vaccine mRNAs stay in the outer part of the cell (the cytoplasm). What’s more, after being transcribed into protein just one time, the mRNA quickly degrades. Others have expressed concerns about whether the vaccine could cause COVID-19. That is not a risk because there’s no whole virus involved, just the coding instructions for the non-infectious spike protein.
An important advantage of mRNA is that it’s easy for researchers to synthesize once they know the nucleic acid sequence of a target viral protein. So, the gift of mRNA vaccines is one that will surely keep on giving. This new technology can now be used to speed the development of future vaccines. After the emergence of the disease-causing SARS, MERS, and now SARS-CoV-2 viruses, it would not be surprising if there are other coronavirus health threats in our future. Corbett and her colleagues are hoping to design a universal vaccine that can battle all of them. In addition, mRNA vaccines may prove effective for fighting future pandemics caused by other infectious agents and for preventing many other conditions, such as cancer and HIV.
Though vaccines are unquestionably our best hope for getting past the COVID-19 pandemic, public surveys indicate that some people are uneasy about accepting this disease-preventing gift. Some have even indicated they will refuse to take the vaccine. Healthy skepticism is a good thing, but decisions like this ought to be based on weighing the evidence of benefit versus risk. The results of the Pfizer and Moderna trials, all released for complete public scrutiny, indicate the potential benefits are high and the risks, low. Despite the impressive speed at which the new COVID-19 vaccines were developed, they have undergone and continue to undergo a rigorous process to generate all the data needed by the FDA to determine their long-term safety and effectiveness.
Unfortunately, the gift of COVID-19 vaccines comes too late for the more than 313,000 Americans who have died from complications of COVID-19, and many others who’ve had their lives disrupted and may have to contend with long-term health consequences related to COVID-19. The vaccines did arrive in record time, but all of us wish they could somehow have arrived even sooner to avert such widespread suffering and heartbreak.
It will be many months before all Americans who are willing to get a vaccine can be immunized. We need 75-80 percent of Americans to receive vaccines in order to attain the so-called “herd immunity” needed to drive SARS-CoV-2 away and allow us all to get back to a semblance of normal life.
Meanwhile, we all have a responsibility to do everything possible to block the ongoing transmission of this dangerous virus. Each of us needs to follow the three W’s: Wear a mask, Watch your distance, Wash your hands often.
When your chance for immunization comes, please roll up your sleeve and accept the potentially life-saving gift of a COVID-19 vaccine. In fact, I just got my first shot of the Moderna vaccine today along with NIAID Director Anthony Fauci, HHS Secretary Alex Azar, and some front-line healthcare workers at the NIH Clinical Center. Accepting this gift is our best chance to put this pandemic behind us, as we look forward to a better new year.
Links:
Coronavirus (COVID-19) (NIH)
Combat COVID (U.S. Department of Health and Human Services, Washington, D.C.)
Dale and Betty Bumpers Vaccine Research Center (National Institute of Allergy and Infectious Diseases/NIH)
Moderna (Cambridge, MA)
Pfizer (New York, NY)
BioNTech (Mainz, Germany)
Researchers Publish Encouraging Early Data on COVID-19 Vaccine
Posted on by Dr. Francis Collins

People all around the globe are anxiously awaiting development of a safe, effective vaccine to protect against the deadly threat of coronavirus disease 2019 (COVID-19). Evidence is growing that biomedical research is on track to provide such help, and to do so in record time.
Just two days ago, in a paper in the New England Journal of Medicine [1], researchers presented encouraging results from the vaccine that’s furthest along in U.S. human testing: an innovative approach from NIH’s Vaccine Research Center (VRC), in partnership with Moderna Inc., Cambridge, MA [1]. The centerpiece of this vaccine is a small, non-infectious snippet of messenger RNA (mRNA). Injecting this mRNA into muscle will spur a person’s own body to make a key viral protein, which, in turn, will encourage the production of protective antibodies against SARS-CoV-2—the novel coronavirus that causes COVID-19.
While it generally takes five to 10 years to develop a vaccine against a new infectious agent, we simply don’t have that time with a pandemic as devastating as COVID-19. Upon learning of the COVID-19 outbreak in China early this year, and seeing the genome sequence of SARS-CoV-2 appear on the internet, researchers with NIH’s National Institute of Allergy and Infectious Diseases (NIAID) carefully studied the viral instructions, focusing on the portion that codes for a spike protein that the virus uses to bind to and infect human cells.
Because of their experience with the original SARS virus back in the 2000s, they thought a similar approach to vaccine development would work and modified an existing design to reflect the different sequence of the SARS-CoV-2 spike protein. Literally within days, they had created a vaccine in the lab. They then went on to work with Moderna, a biotech firm that’s produced personalized cancer vaccines. All told, it took just 66 days from the time the genome sequence was made available in January to the start of the first-in-human study described in the new peer-reviewed paper.
In the NIH-supported phase 1 human clinical trial, researchers found the vaccine, called mRNA-1273, to be safe and generally well tolerated. Importantly, human volunteers also developed significant quantities of neutralizing antibodies that target the virus in the right place to block it from infecting their cells.
Conducted at Kaiser Permanente Washington Health Research Institute, Seattle; and Emory University School of Medicine, Atlanta, the trial led by Kaiser Permanente’s Lisa Jackson involved healthy adult volunteers. Each volunteer received two vaccinations in the upper arm at one of three doses, given approximately one month apart.
The volunteers will be tracked for a full year, allowing researchers to monitor their health and antibody production. However, the recently published paper provides interim data on the phase 1 trial’s first 45 participants, ages 18 to 55, for the first 57 days after their second vaccination. The data revealed:
• No volunteers suffered serious adverse events.
• Optimal dose to elicit high levels of neutralizing antibody activity, while also protecting patient safety, appears to be 100 micrograms. Doses administered in the phase 1 trial were either 25, 100, or 250 micrograms.
• More than half of the volunteers reported fatigue, headache, chills, muscle aches, or pain at the injection site. Those symptoms were most common after the second vaccination and in volunteers who received the highest vaccine dose. That dose will not be used in larger trials.
• Two doses of 100 micrograms of the vaccine prompted a robust immune response, which was last measured 43 days after the second dose. These responses were actually above the average levels seen in blood samples from people who had recovered from COVID-19.
These encouraging results are being used to inform the next rounds of human testing of the mRNA-1273 vaccine. A phase 2 clinical trial is already well on its way to recruiting 600 healthy adults.This study will continue to profile the vaccine’s safety, as well as its ability to trigger an immune response.
Meanwhile, later this month, a phase 3 clinical trial will begin enrolling 30,000 volunteers, with particular focus on recruitment in regions and populations that have been particularly hard hit by the virus.
The design of that trial, referred to as a “master protocol,” had major contributions from the Accelerating COVID-19 Therapeutic Interventions and Vaccine (ACTIV) initiative, a remarkable public-private partnership involving 20 biopharmaceutical companies, academic experts, and multiple federal agencies. Now, a coordinated effort across the U.S. government, called Operation Warp Speed, is supporting rapid conduct of these clinical trials and making sure that millions of doses of any successful vaccine will be ready if the vaccine proves save and effective.
Results of this first phase 3 trial are expected in a few months. If you are interested in volunteering for these or other prevention trials, please check out NIH’s new COVID-19 clinical trials network.
There’s still a lot of work that remains to be done, and anything can happen en route to the finish line. But by pulling together, and leaning on the very best science, I am confident that we will be able rise to the challenge of ending this pandemic that has devastated so many lives.
Reference:
[1] A SARS-CoV-2 mRNA Vaccine—Preliminary Report. Jackson LA, Anderson EJ, Rouphael NG, Ledgerwood JE, Graham BS, Beigel JH, et al. NEJM. 2020 July 14. [Publication ahead of print]
Links:
Coronavirus (COVID-19) (NIH)
Dale and Betty Bumpers Vaccine Research Center (National Institute of Allergy and Infectious Diseases/NIH)
Moderna, Inc. (Cambridge, MA)
Safety and Immunogenicity Study of 2019-nCoV Vaccine (mRNA-1273) for Prophylaxis of SARS-CoV-2 Infection (COVID-19) (ClinicalTrials.gov)
“NIH Launches Clinical Trials Network to Test COVID-19 Vaccines and Other Prevention Tools,” NIAID News Release, NIH, July 8, 2020.
Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) (NIH)
Explaining Operation Warp Speed (U.S. Department of Health and Human Services, Washington, DC)
NIH Support: National Institute of Allergy and Infectious Diseases
Next Page