South Africa
This Is Why NIH Invests in Global Health Research
Posted on by Roger I. Glass, M.D., Ph.D., Fogarty International Center

Efforts over the past few years to end the COVID-19 pandemic clearly reveal how global health impacts individual wellbeing and national security. At NIH, the Fogarty International Center helps the other institutes become engaged with global health research, which investigates the dual burden of infectious disease and non-communicable disease.
Global health research also encompasses data science, economics, genetics, climate change science, and many other disciplines. For more than 50 years, Fogarty has been building partnerships among institutions in the U.S. and abroad, while training the next generation of scientists focused on universal health needs.
America’s investment in Fogarty has paid rich dividends
During the pandemic, in particular, we’ve seen researchers trained by our programs make scientific discoveries that contributed to international security. Take Jessica Manning, a former Fogarty fellow who now conducts malaria research in Phnom Penh, Cambodia. Her team at the Ministry of Health sequenced the viral strain of SARS-CoV-2, the cause of COVID-19, infecting the first Cambodian patient and documented early the spread of this novel coronavirus outside of China.
Similarly, Christian Happi, director of the African Centre of Excellence for the Genomics of Infectious Disease, Ede, Nigeria, sequenced the first SARS-CoV-2 genome in Africa. Happi was able to do it by adapting the sequencing and analytical pipelines that he’d created back when he was a Fogarty grantee studying Ebola.
In Botswana, Sikhulile Moyo leveraged the skills he’d acquired while supported by a Fogarty HIV research training grant with Max Essex, Harvard School of Public Health, Cambridge, MA, to track COVID-19 mutations for his country’s Ministry of Health. Last November, he alerted the world of a new Omicron variant. Within six weeks, Omicron became the dominant global strain, challenging the ability of COVID vaccines to control its spread. In the Dominican Republic, William Duke, a national commission member, used what he’d learned as a Fogarty trainee to help create a national COVID-19 intervention plan to prevent and control the disease.
Fogarty’s fostering of global health leaders is one way we advance scientific expertise while ensuring our nation’s biosecurity. Another is by finding effective ways to study abroad the same health conditions that affect our own population.
Research conducted in Colombia, for example, may provide clues for preventing Alzheimer’s disease in the U.S. Fogarty support brought together neuroscientists Kenneth Kosik, University of California, Santa Barbara, and Francisco Lopera, University of Antioquia, Colombia, to study members of the largest-known family with an early-onset, rapidly progressive form of the disease. Over the years, Kosik and Lopera have trained local scientists, explored gene therapy targets, investigated biomarkers to monitor disease progression, and conducted drug trials in search of a cure for Alzheimer’s.
Researchers in other fields also discover unique opportunities to investigate populations with high rates of disease. Siana Nkya, a Fogarty grantee based in Tanzania, has devoted her career to studying the genetic determinants of sickle cell disease, which affects many people around the world, including in the U.S. We hope that US-African partnerships might develop improved, affordable treatments and a cure for all patients with this devastating disease. Similarly, people in the U.S. have access to state-of-the-art HIV treatment studies in places around the globe where incidence rates are higher.
Fogarty has supported many milestone achievements in HIV research over the years. Among them is a study that took place in nine countries. The research, led by Myron Cohen of the University of North Carolina at Chapel Hill, established that antiretroviral therapy can prevent sexual transmission of HIV-1 among couples in which one person is infected and the other is not. In fact, this research informs current HIV treatment recommendations worldwide, including in the U.S.
Americans will also undoubtedly benefit from projects funded by Fogarty’s Global Brain and Nervous System Disorders Research across the Lifespan program. For example, psychologist Tatiana Balachova, University of Oklahoma, Oklahoma City, has designed an intervention for women in Russia to prevent fetal alcohol spectrum disorders. In another project in South Africa, Sandra and Joseph Jacobson, Wayne State University, Detroit, conducted the first-ever prospective longitudinal study of the syndrome. Findings from both projects are ripe for translation within an American context.
Other examples of Global Brain program investigations with broad implications in our own country include studying early psychosis in China; capacity building for schizophrenia research in Macedonia; exploring family consequences from the Zika virus in Brazil; and studying dementia and related health and social challenges in Lebanon.
These are just a few examples of Fogarty’s work and its unique mission. What is most remarkable about Fogarty is that just under 90 percent of our grants are co-funded by at least one other NIH institute, center, or office. Collaboration, both within borders and across them, is Fogarty’s formula for success.
Links:
Fogarty International Center (NIH)
Overview of Brain Disorders: Research Across the Lifespan (Fogarty)
Former Fogarty Scholar Dr Jessica Manning Helps Cambodia Respond to COVID (Fogarty)
Christian Happi: Former Fogarty Grantee Leads COVID-19 Genomics Work in Africa (Fogarty)
Sikhulile Moyo: Fogarty Fellow Recognized for Omicron Discovery (Fogarty)
William Duke: Former Fogarty HIV Trainee Helps Lead Dominican Republic’s COVID Response (Fogarty)
Kenneth Kosic and Francisco Lopera: NIH Support Spurs Alzheimer’s Research in Colombia (Fogarty)
Former Fogarty fellow Siana Nkya Tackles Sickle Cell Disease in Tanzania (Fogarty)
Tatiana Balachova: Researchers Tackle Fetal Alcohol Syndrome in Russia (Fogarty)
Sandra and Joseph Jacobson: Fetal Alcohol Exposure Research Supported by NIAAA in South Africa, Ukraine and Russia Improves Prevention, Outcomes (Fogarty)
Note: Dr. Lawrence Tabak, who performs the duties of the NIH Director, has asked the heads of NIH’s Institutes and Centers (ICs) to contribute occasional guest posts to the blog to highlight some of the interesting science that they support and conduct. This is the 22nd in the series of NIH IC guest posts that will run until a new permanent NIH director is in place.
Latest on Omicron Variant and COVID-19 Vaccine Protection
Posted on by Dr. Francis Collins
There’s been great concern about the new Omicron variant of SARS-CoV-2, the coronavirus that causes COVID-19. A major reason is Omicron has accumulated over 50 mutations, including about 30 in the spike protein, the part of the coronavirus that mRNA vaccines teach our immune systems to attack. All of these genetic changes raise the possibility that Omicron could cause breakthrough infections in people who’ve already received a Pfizer or Moderna mRNA vaccine.
So, what does the science show? The first data to emerge present somewhat encouraging results. While our existing mRNA vaccines still offer some protection against Omicron, there appears to be a significant decline in neutralizing antibodies against this variant in people who have received two shots of an mRNA vaccine.
However, initial results of studies conducted both in the lab and in the real world show that people who get a booster shot, or third dose of vaccine, may be better protected. Though these data are preliminary, they suggest that getting a booster will help protect people already vaccinated from breakthrough or possible severe infections with Omicron during the winter months.
Though Omicron was discovered in South Africa only last month, researchers have been working around the clock to learn more about this variant. Last week brought the first wave of scientific data on Omicron, including interesting work from a research team led by Alex Sigal, Africa Health Research Institute, Durban, South Africa [1].
In lab studies working with live Omicron virus, the researchers showed that this variant still relies on the ACE2 receptor to infect human lung cells. That’s really good news. It means that the therapeutic tools already developed, including vaccines, should generally remain useful for combatting this new variant.
Sigal and colleagues also tested the ability of antibodies in the plasma from 12 fully vaccinated individuals to neutralize Omicron. Six of the individuals had no history of COVID-19. The other six had been infected with the original variant in the first wave of infections in South Africa.
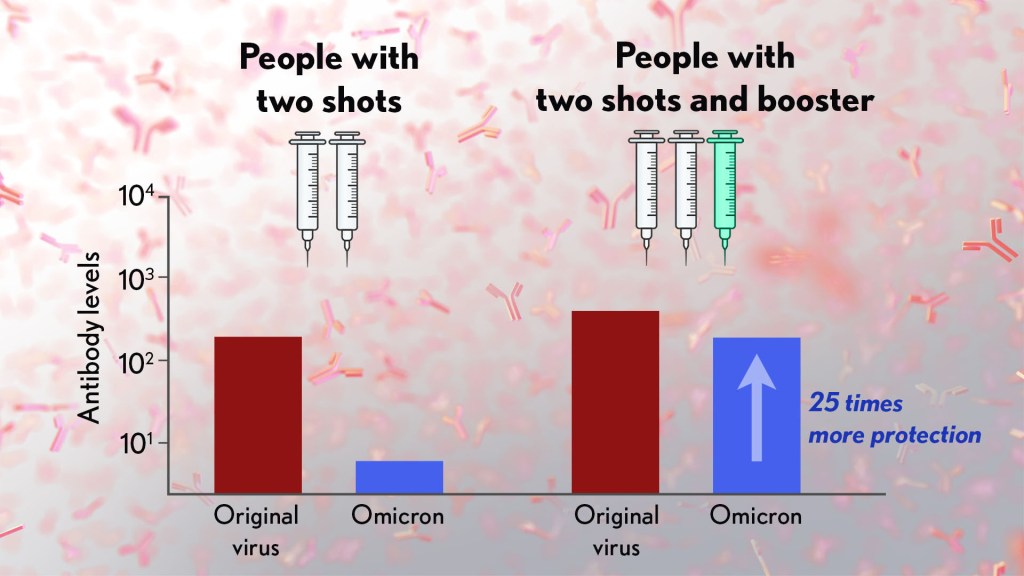
As expected, the samples showed very strong neutralization against the original SARS-CoV-2 variant. However, antibodies from people who’d been previously vaccinated with the two-dose Pfizer vaccine took a significant hit against Omicron, showing about a 40-fold decline in neutralizing ability.
This escape from immunity wasn’t complete. Indeed, blood samples from five individuals showed relatively good antibody levels against Omicron. All five had previously been infected with SARS-CoV-2 in addition to being vaccinated. These findings add to evidence on the value of full vaccination for protecting against reinfections in people who’ve had COVID-19 previously.
Also of great interest were the first results of the Pfizer study, which the company made available in a news release [2]. Pfizer researchers also conducted laboratory studies to test the neutralizing ability of blood samples from 19 individuals one month after a second shot compared to 20 others one month after a booster shot.
These studies showed that the neutralizing ability of samples from those who’d received two shots had a more than 25-fold decline relative to the original virus. Together with the South Africa data, it suggests that the two-dose series may not be enough to protect against breakthrough infections with the Omicron variant.
In much more encouraging news, their studies went on to show that a booster dose of the Pfizer vaccine raised antibody levels against Omicron to a level comparable to the two-dose regimen against the original variant (as shown in the figure above). While efforts already are underway to develop an Omicron-specific COVID-19 vaccine, these findings suggest that it’s already possible to get good protection against this new variant by getting a booster shot.
Very recently, real-world data from the United Kingdom, where Omicron cases are rising rapidly, are providing additional evidence for how boosters can help. In a preprint [3], Andrews et. al showed the effectiveness of two shots of Pfizer mRNA vaccine trended down after four months to about 40 percent. That’s not great, but note that 40 percent is far better than zero. So, clearly there is some protection provided.
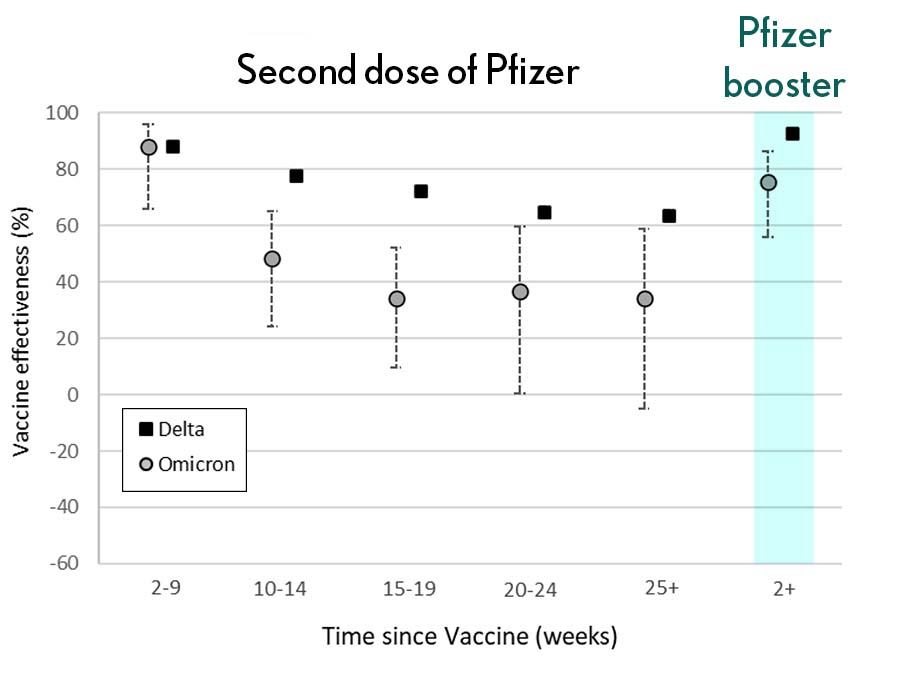
Most impressively (as shown in the figure from Andrews N, et al.) a booster substantially raised that vaccine effectiveness to about 80 percent. That’s not quite as high as for Delta, but certainly an encouraging result. Once again, these data show that boosting the immune system after a pause produces enhanced immunity against new viral variants, even though the booster was designed from the original virus. Your immune system is awfully clever. You get both quantitative and qualitative benefits.
It’s also worth noting that the Omicron variant mostly doesn’t have mutations in portions of its genome that are the targets of other aspects of vaccine-induced immunity, including T cells. These cells are part of the body’s second line of defense and are generally harder for viruses to escape. While T cells can’t prevent infection, they help protect against more severe illness and death.
It’s important to note that scientists around the world are also closely monitoring Omicron’s severity While this variant appears to be highly transmissible, and it is still early for rigorous conclusions, the initial research indicates this variant may actually produce milder illness than Delta, which is currently the dominant strain in the United States.
But there’s still a tremendous amount of research to be done that could change how we view Omicron. This research will take time and patience.
What won’t change, though, is that vaccines are the best way to protect yourself and others against COVID-19. (And these recent data provide an even-stronger reason to get a booster now if you are eligible.) Wearing a mask, especially in public indoor settings, offers good protection against the spread of all SARS-CoV-2 variants. If you’ve got symptoms or think you may have been exposed, get tested and stay home if you get a positive result. As we await more answers, it’s as important as ever to use all the tools available to keep yourself, your loved ones, and your community happy and healthy this holiday season.
References:
[1] SARS-CoV-2 Omicron has extensive but incomplete escape of Pfizer BNT162b2 elicited neutralization and requires ACE2 for infection. Sandile C, et al. Sandile C, et al. medRxiv preprint. December 9, 2021.
[2] Pfizer and BioNTech provide update on Omicron variant. Pfizer. December 8, 2021.
[3] Effectiveness of COVID-19 vaccines against the Omicron (B.1.1.529) variant of concern. Andrews N, et al. KHub.net preprint. December 10, 2021.
Links:
COVID-19 Research (NIH)
Sigal Lab (Africa Health Research Institute, Durban, South Africa)
Tracking the Evolution of a ‘Variant of Concern’ in Brazil
Posted on by Dr. Francis Collins
By last October, about three out of every four residents of Manaus, Brazil already had been infected with SARS-CoV-2, the virus that causes COVID-19 [1]. And yet, despite hopes of achieving “herd immunity” in this city of 2.2 million in the Amazon region, the virus came roaring back in late 2020 and early 2021 to cause a second wave of illness and death [2]. How is this possible?
The answer offers a lesson in viral evolution, especially when an infectious virus such as SARS-CoV-2 replicates and spreads through a population largely unchecked. In a recent study in the journal Science, researchers tied the city’s resurgence of SARS-CoV-2 to the emergence and rapid spread of a new SARS-CoV-2 “variant of concern” known as P.1 [3]. This variant carries a unique constellation of mutations that allow it not only to sneak past the human immune system and re-infect people, but also to be about twice as transmissible as earlier variants.
To understand how this is possible, consider that each time the coronavirus SARS-CoV-2 makes copies of itself in an infected person, there’s a chance a mistake will be made. Each mistake can produce a new variant that may go on to make more copies of itself. In most cases, those random errors are of little to no consequence. This is evolution in action.
But sometimes a spelling change can occur that benefits the virus. In the special case of patients with suppressed immune systems, the virus can have ample opportunity to accrue an unusually high number of mutations. Variants carrying beneficial mutations can make more copies of themselves than other variants, allowing them to build their numbers and spread to cause more infection.
At this advanced stage of the COVID-19 pandemic, such rapidly spreading new variants remain cause for serious concern. That includes variants such as B.1.351, which originated in South Africa; B.1.1.7 which emerged in the United Kingdom; and now P.1 from Manaus, Brazil.
In the new study, Nuno Faria and Samir Bhatt, Imperial College London, U.K., and Ester Cerdeira Sabino, Universidade de Sao Paulo, Brazil, and their colleagues sequenced SARS-CoV-2 genomes from 184 patient samples collected in Manaus in November and December 2020. The research was conducted under the auspices of the Brazil-UK Centre for Arbovirus Discovery, Diagnosis, Genomics and Epidemiology (CADDE), a project focused on viral genomics and epidemiology for public health.
Those genomic data revealed the P.1 variant had acquired 17 new mutations. Ten were in the spike protein, which is the segment of the virus that binds onto human cells and the target of current COVID-19 vaccines. In fact, the new work reveals that three of these spike protein mutations make it easier for the P.1 spike to bind the human ACE2 receptor, which is SARS-CoV-2’s preferred entry point.
The first P.1 variant case was detected by genomic surveillance on December 6, 2020, after which it spread rapidly. Through further evolutionary analysis, the team estimates that P.1 must have emerged, undetected for a brief time, in mid-November 2020.
To understand better how the P.1 variant led to such an explosion of new COVID-19 cases, the researchers developed a mathematical model that integrated the genomic data with mortality data. The model suggests that P.1 may be 1.7 to 2.4 times more transmissible than earlier variants. They also estimate that a person previously infected with a variant other than P.1 will have only 54 percent to 79 percent protection against a subsequent infection with P.1.
The researchers also observed an increase in mortality following the emergence of the P.1 variant. However, it’s not yet clear if that’s an indication P.1 is inherently more deadly than earlier variants. It’s possible the increased mortality is related primarily to the extra stress on the healthcare system in Manaus from treating so many people with COVID-19.
These findings are yet another reminder of the importance of genomic surveillance and international data sharing for detecting and characterizing emerging SARS-CoV-2 variants quickly. It’s worth noting that at about the same time this variant was detected in Brazil, it also was reported in four individuals who had traveled to Brazil from Japan. The P.1 variant continues to spread rapidly across Brazil. It has also been detected in more than 37 countries [4], including the United States, where it now accounts for more than 1 percent of new cases [5].
No doubt you are wondering what this means for vaccines, such as the Pfizer and Moderna mRNA vaccines, that have been used to immunize (at least one dose) over 140 million people in the United States. Here the news is encouraging. Serum from individuals who received the Pfizer vaccine had titers of neutralizing antibodies that were only slightly reduced for P.1 compared to the original SARS-CoV-2 virus [6]. Therefore, the vaccine is predicted to be highly protective. This is another example of a vaccine providing more protection than a natural infection.
The United States has made truly remarkable progress in combating COVID-19, but we must heed this lesson from Manaus: this terrible pandemic isn’t over just yet. While the P.1 variant remains at low levels here for now, the “U.K. variant” B.1.1.7 continues to spread rapidly and now is the most prevalent variant circulating in the U.S., accounting for 44 percent of new cases [6]. Fortunately, the mRNA vaccines also work well against B.1.1.7.
We must continue to do absolutely everything possible, individually and collectively, to prevent these new SARS-CoV-2 variants from slowing or even canceling the progress made over the last year. We need to remain vigilant for just a while longer, while encouraging our friends, neighbors, and loved ones to get vaccinated.
References:
[1] Three-quarters attack rate of SARS-CoV-2 in the Brazilian Amazon during a largely unmitigated epidemic. Buss, L. F., C. A. Prete, Jr., C. M. M. Abrahim, A. C. Dye, V. H. Nascimento, N. R. Faria and E. C. Sabino et al. (2021). Science 371(6526): 288-292.
[2] Resurgence of COVID-19 in Manaus, Brazil, despite high seroprevalence. Sabino EC, Buss LF, Carvalho MPS, Prete Jr CCA, Crispim MAE, Fraiji NA, Pereira RHM, Paraga KV, Peixoto PS, Kraemer MUG, Oikawa MJ, Salomon T, Cucunuba ZM, Castro MC, Santos AAAS, Nascimento VH, Pereira HS, Ferguson NM, Pybus OG, Kucharski A, Busch MP, Dye C, Faria NR Lancet. 2021 Feb 6;397(10273):452-455.
[3] Genomics and epidemiology of the P.1 SARS-CoV-2 lineage in Manaus, Brazil. Faria NR, Mellan TA, Whittaker C, Claro IM, Fraiji NA, Carvalho MDPSS, Pybus OG, Flaxman S, Bhatt S, Sabino EC et al. Science. 2021 Apr 14:eabh2644.
[4] GRINCH Global Report Investigating novel coronavirus haplotypes. PANGO Lineages.
[5] COVID Data Tracker. Variant Proportions. Centers for Disease Control and Prevention.
[6] Antibody evasion by the P.1 strain of SARS-CoV-2. Dejnirattisai W, Zhou D, Supasa P, Liu C, Mongkolsapaya J, Ren J, Stuart DI, Screaton GR, et al. Cell. 2021 Mar 30:S0092-8674(21)00428-1.
Links:
COVID-19 Research (NIH)
Brazil-UK Centre for Arbovirus Discovery, Diagnosis, Genomics and Epidemiology (CADDE)
Nuno Faria (Imperial College, London, U.K.)
Samir Bhatt (Imperial College)
Ester Cerdeira Sabino (Universidade de Sao Paulo, Brazil)
NIH Support: National Institute of Allergy and Infectious Diseases
South Africa Study Shows Power of Genomic Surveillance Amid COVID-19 Pandemic
Posted on by Dr. Francis Collins

Considerable research is underway around the world to monitor the spread of new variants of SARS-CoV-2, the coronavirus that causes COVID-19. That includes the variant B.1.351 (also known as 501Y.V2), which emerged in South Africa towards the end of 2020 [1, 2]. Public health officials in South Africa have been busy tracing the spread of this genomic variant and others across their country. And a new analysis of such data reveals that dozens of distinct coronavirus variants were already circulating in South Africa well before the appearance of B.1.351.
A study of more than 1,300 near-whole genome sequences of SARS-CoV-2, published recently in the journal Nature Medicine, shows there were in fact at least 42 SARS-CoV-2 variants spreading in South Africa within the pandemic’s first six months in that country [3]. Among them were 16 variants that had never before been described. Most of the single-letter changes carried by these variants didn’t change the virus in important ways and didn’t rise to significant frequency. But the findings come as another critical reminder of the value of genomic surveillance to track the spread of SARS-CoV-2 to identify any potentially worrisome new variants and to inform measures to get this devastating pandemic under control.
SARS-CoV-2 was first detected in South Africa on March 5, 2020, in a traveler returning from Italy. By November 2020, despite considerable efforts to slow the spread, more than 785,000 people in South Africa were infected, accounting for about half of all reported COVID-19 cases on the African continent.
Recognizing the importance of genomic surveillance, researchers led by Houriiyah Tegally and Tulio de Oliveira, University of KwaZulu-Natal, Durban, South Africa, wasted no time in producing 1,365 near-complete SARS-CoV-2 genomes by mid-September, near the end of the coronavirus’s first peak in the country. Those samples had been collected in hundreds of clinics over the course of the pandemic in eight of South Africa’s nine provinces, offering a broad picture of the spread and emergence of new variants across the country.
The data revealed three main variants, dubbed B.1.1.54, B.1.1.56, and C.1, that were responsible for 42 percent of all the infections in South Africa’s first wave. Of the 16 newly described variants, most carried single-letter changes that haven’t been identified in other countries.
The majority of changes were what scientists refer to as “synonymous,” meaning that they don’t change the structure or function of any of the virus’s essential proteins. The exception is the newly identified C.1, which includes 16 single-letter changes compared to the original sequence from Wuhan, China. One of those 16 changes swaps a single amino acid for another on SARS-CoV-2’s spike protein. That’s notable because the spike protein is a key target of antibodies and also is essential to the virus’s ability to infect human cells.
In fact, four of the most prevalent variants in South Africa all carry this same mutation. The researchers also saw three other changes that would alter the spike protein in different ways, although the significance of these for viral spread and our efforts to stop it isn’t yet clear.
Importantly, the data show that the bulk of introductions to South Africa happened early on, before lockdown and travel restrictions were implemented in late March. Subsequently, much of the spread within South Africa stemmed from hospital outbreaks. For example, an outbreak of the C.1 variant in the North West Province in April ultimately led this variant to become the most geographically widespread in South Africa by the end of August. Meanwhile, an earlier identified South African-specific variant, B.1.106, first identified in April, vanished altogether after outbreaks were controlled in KwaZulu-Natal Province, where the researchers reside.
Genomic surveillance has remarkable power for understanding the evolution of SARS-CoV-2 and tracking the dynamics of its transmission. Tegally and de Oliveira’s team notes that this type of intensive genomic surveillance now can be used on a large scale across Africa and around the world to identify new variants of SARS-CoV-2 and to develop timely measures to control the spread of the virus. They’re now working with the African CDC to expand genomic surveillance across Africa [4].
Such genomic surveillance was crucial in the subsequent identification of the B.1.351 variant in South Africa that we’ve been hearing so much about, with its potential to evade our current treatments and vaccines. By picking up on such concerning mutations early through genomic surveillance and understanding how the virus is spreading over time and space, the hope is we’ll be better informed and more adept in our efforts to get this pandemic under control.
References:
[1] Emerging SARS-CoV-2 variants. Centers for Disease Control and Prevention.
[2] Emergence and rapid spread of a new severe acute respiratory syndrome-related coronavirus 2 (SARS-CoV-2) lineage with multiple spike mutations in South Africa. Tegally H, Wilkinson E, Giovanetti M, Iranzadeh A, Bhiman J, Williamson C, de Oliveira T, et al. medRxiv 2020 Dec 22.
[3] Sixteen novel lineages of SARS-CoV-2 in South Africa. Tegally H, Wilkinson E, Lessells RJ, Giandhari J, Pillay S, Msomi N, Mlisana K, Bhiman JN, von Gottberg A, Walaza S, Fonseca V, Allam M, Ismail A, Glass AJ, Engelbrecht S, Van Zyl G, Preiser W, Williamson C, Petruccione F, Sigal A, Gazy I, Hardie D, Hsiao NY, Martin D, York D, Goedhals D, San EJ, Giovanetti M, Lourenço J, Alcantara LCJ, de Oliveira T. Nat Med. 2021 Feb 2.
[4] Accelerating genomics-based surveillance for COVID-19 response in Africa. Tessema SK, Inzaule SC, Christoffels A, Kebede Y, de Oliveira T, Ouma AEO, Happi CT, Nkengasong JN.Lancet Microbe. 2020 Aug 18.
Links:
COVID-19 Research (NIH)
Houriiyah Tegally (University of KwaZulu-Natal, Durban, South Africa)
Tulio de Oliveira (University of KwaZulu-Natal)
Global Effort to End AIDS Would Save Millions of Lives
Posted on by Dr. Francis Collins

Scanning electromicrograph of an HIV-infected T cell/NIAID
Almost 37 million people around the world are now infected with human immunodeficiency virus (HIV), the virus that causes AIDS [1]. But many don’t know they are infected or lack access to medical care. Even though major strides have been made in treating the infection, less than half receive antiretroviral therapy (ART) that could prevent full-blown AIDS and reduce the likelihood of the virus being transmitted to other people. Now, a new report restores hope that an end to this very serious public health challenge could be within reach—but that will require a major boost in commitment and resources.
The study conducted by an NIH-funded research team evaluated the costs and expected life-saving returns associated with ambitious goals for HIV testing and treatment, the so-called 90-90-90 program, issued by the Joint United Nations Programme on HIV/AIDS (UNAIDS) in 2014 [2]. The new analysis, based on HIV disease progression and treatment data in South Africa, finds that those goals, though expensive to implement, can be achieved cost-effectively, potentially containing the AIDS epidemic and saving many millions of lives around the globe.
Creative Minds: Harnessing Technologies to Study Air Pollution’s Health Risks
Posted on by Dr. Francis Collins

Perry Hystad
Credit: Hannah O’Leary, Oregon State University
After college, Perry Hystad took a trip to India and, while touring several large cities, noticed the vast clouds of exhaust from vehicles, smoke from factories, and soot from biomass-burning cook stoves. As he watched the rapid urban expansion all around him, Hystad remembers thinking: What effect does breathing such pollution day in and day out have upon these people’s health?
This question stuck with Hystad, and he soon developed a profound interest in environmental health. In 2013, Hystad completed his Ph.D. in his native Canada, studying the environmental risk factors for lung cancer [1, 2, 3]. Now, with the support of an NIH Director’s Early Independence Award, Hystad has launched his own lab at Oregon State University, Corvallis, to investigate further the health impacts of air pollution, which one recent analysis indicates may contribute to as many as several million deaths worldwide each year [4].