monoclonal antibody
Lessons Learned About Substance Use Disorders During the COVID-19 Pandemic
Posted on by Dr. Francis Collins

Every spring, I and my colleague Dr. Nora Volkow, Director of NIH’s National Institute on Drug Abuse (NIDA), join with leaders across the country in the Rx Drug Abuse and Heroin Summit. Our role is to discuss NIH’s continued progress in tackling our nation’s opioid crisis. Because of the continued threat of COVID-19 pandemic, we joined in virtually for the second year in a row.
While the demands of the pandemic have been challenging for everyone, biomedical researchers have remained hard at work to address the opioid crisis. Among the many ways that NIH is supporting these efforts is through its Helping to End Addiction Long-Term (HEAL) Initiative, which is directing more than $1.5 billion to researchers and communities across the country.
Here’s a condensed transcript of our April 6th video dialogue, which focused on the impact of the COVID-19 pandemic on people struggling with substance use disorders and those who are trying to help them.

Collins: What have we learned so far through HEAL? Well, one thing HEAL is doing is tackling the need for pain treatments that help people avoid the risks of opioids. This research has uncovered new targets and therapeutics for different types of pain, including neuropathic, post-surgical, osteoarthritic, and chemotherapy induced. We’re testing implanted devices, such as electrodes and non-invasive nerve stimulation; and looking at complementary and integrative approaches, such as phone-based physical therapy for low back pain.
Through HEAL, we’ve launched a first-in-human test of a vaccine to protect against the harmful effects of opioids, including relapse and overdose. We’re also testing a tool that provides pharmacists with a validated opioid use disorder risk measure. The goal is to identify better who’s at high risk for opioid addiction and to determine what kind of early intervention could be put in place.
Despite COVID, many clinical studies are now recruiting participants. This includes family-based prevention programs, culturally tailored interventions for hard-hit American Indian populations, and interventions that address social inequities, such as lack of housing.
We are also making progress on the truly heart-breaking problem of babies born dependent on opioids. HEAL has launched a study to test the effectiveness of a new approach to care that measures the severity of a baby’s withdrawal, based on their ability to eat, sleep, and be consoled. This approach helps provide appropriate treatment for these infants, without the use of medication when possible. We’re also developing novel technologies to help treat neonatal opioid withdrawal syndrome, including a gently vibrating hospital bassinet pad that’s received breakthrough device designation from the FDA.
2020 was an extraordinary year that was tragic in so many ways, including lives lost and economic disasters that have fallen upon families. The resilience and ingenuity of the scientific community has been impressive. Quick pivoting has resulted in some gains through research, maybe you could even call them silver linings in the midst of this terrible storm.
Nora, what’s been at the forefront of your mind as we’ve watched things unfold?
Volkow: When we did this one year ago, we didn’t know what to expect. Obviously, we were concerned that the stressors associated with a pandemic, with unknowns, are factors that have been recognized for many years to increase drug use. Unfortunately, what we’ve seen is an increase in drug use of all types across the country.
We have seen an exacerbation of the opioid epidemic, as evidenced by the number of people who have died. Already, in the 12 months ending in July 2020, there was a 24 percent increase in mortality from overdoses. Within those numbers, there was close to a 50 percent increase in mortality associated with fentanyl. We’re also seeing an increase, not just in deaths from fentanyl and other synthetic opioids, but in deaths from stimulant drugs, like cocaine and methamphetamine. And the largest increases have been very much driven by drug combinations.
So, we have the perfect storm. We have people stressed to their limits by decreases in the economy, the loss of jobs, the death of loved ones. On the other hand, we see dealers taking the opportunity to bring in drugs such as synthetic opioids and synthetic stimulants and distribute them to a much wider extent than previously seen.

Collins: On top of that, people are at risk of getting sick from COVID-19. What have we learned about the risks of coronavirus illness for people who use drugs?
Volkow: It is a double whammy. When you look at the electronic health records about the outcomes of people diagnosed with substance use disorders, you consistently see an increased risk for getting infected with COVID-19. And if you look at those who get infected, you observe a significantly increased risk of dying from COVID.
What’s driving this vulnerability? One factor is the pharmacological effects of these drugs. Basically, all of the drugs of abuse that result in addiction, notably opioids, damage the cardiopulmonary system. Some also damage the immune system. And we know that individuals who have any disruption of cardiovascular health, pulmonary health, immune function, or metabolism are at higher risk of getting infected with COVID-19 and having adverse outcomes.
But there’s another factor that’s as important—one that’s very tractable. It is the way in which our society has dealt with substance use disorders: not actually treating them as a disease that requires intervention and support for recovery. The stigmatization of individuals with addiction, the lack of access to treatment, the social isolation, have all created havoc by making these individuals so much more vulnerable to get infected with COVID-19.
They will not go to a doctor. They don’t want to be stigmatized. They need to go out into the streets to get access to the drugs. Many times, they don’t have a choice of what drugs to take because they cannot afford anything except what’s offered to them. So, many, especially those who are minorities, end up homeless or in jails or prison. Even before COVID, we knew that prisons and jails are places where infections can transmit extraordinary rapidly. You could see this was going to result in very negative outcomes for this group of individuals.
Collins: Nora, tell us more about the trends contributing to the current crisis. Maybe three or four years ago, what was going straight up was opioid use, especially heroin. Then, fentanyl started coming up very fast and that has continued. Now, we are seeing more stimulants and mixing of different types of drugs. What is the basis for this?
Volkow: At the beginning of the opiate pandemic, mortality was mainly associated with white Americans, many in rural or semi-suburban areas of the Appalachian states and in New Mexico and Arizona. That has shifted. The highest increase in mortality from opioids, predominantly driven by fentanyl, is now among Black Americans. They’ve had very, very high rates of mortality during the COVID pandemic. And when you look at mortality from methamphetamine, it’s chilling to realize that the risk of dying from methamphetamine overdose is 12-fold higher among American Indians and Alaskan Natives than other groups. This should make us pause to think about what’s driving these terrible racial disparities.
As for drug combinations, many deaths from methamphetamine or cocaine—an estimated 50 percent—are linked to these stimulant drugs being combined with fentanyl or heroin. Dealers are lacing these non-opioid drugs with cheaper, yet potent, opioids to make a larger profit. Someone who’s addicted to a stimulant drug like cocaine or methamphetamine is not tolerant to opioids, which means they are going to be at high risk of overdose if they get a stimulant drug that’s laced with an opioid like fentanyl. That’s been contributing to the sharp rise in mortality from non-opioid drugs.
Collins: I’m glad you raised the issue of health disparities. 2020 will go down as a year in which our nation had to focus on three public health crises at once. The first is the crisis of opioid use disorder and rising mortality from use of other drugs. The second is COVID-19. And the third is the realization, although the problem has been there all along, that health disparities continue to shorten the lives of far too many people.
The latter crisis has little to do with biology, but everything to do with the way in which our society still is afflicted by structural racism. We at NIH are looking at this circumstance, realizing that our own health disparities research agenda needs to be rethought. We have not fully incorporated all the factors that play out in health inequities and racial inequities in our country.
You were also talking about how stimulants have become more widespread. What about treatments for people with stimulant use disorders?
Volkow: For opioid addiction, we’re lucky because we have very effective medications: methadone, buprenorphine, naltrexone. On top of that, we have naloxone, Narcan, that if administered on time, can save the life of a person who has overdosed.
We don’t have any FDA-approved medication for methamphetamine addiction, and we don’t have any overdose reversal for methamphetamine. At the beginning of this year, we funded a large clinical trial aimed at investigating the benefits of the combination of two medications that were already approved as anti-depressants and for the treatment of smoking cessation and alcoholism. It found this combination significantly inhibits the urge to take drugs and therefore helps people stay away from use of methamphetamine. Now, we want to replicate these findings, and to tie that replication study in with guidelines from the FDA on what is needed to approve our new indication for these medications. Why? Because then insurance can cover it, and that will increase the likelihood that people will get treated.
Another exciting possibility is a monoclonal antibody against methamphetamine that’s in Phase 2 clinical trials. If someone comes into the emergency room with an overdose of a combination of opioid and methamphetamine, naloxone often will not work. But this monoclonal antibody with naloxone may offer a greater likelihood of success.
Another thing that’s promising is that investigators have been able to modify monoclonal antibodies so they stay in the bloodstream for a longer time. That means we may someday be able to use this passive immunization approach as a treatment for methamphetamine addiction.
Collins: That’s good to hear. Speaking of progress, is there any you want to point to within HEAL?
Volkow: There’s a lot of excitement surrounding medication development. We’re interested in developing antidotes that will be more effective in reversing overdose deaths from fentanyl. We’re also interested in providing longer lasting medications for treatment of opioid use disorders, which would improve the likelihood of patients being protected from overdoses.
The Justice Community Opioid Innovation Network (JCOIN) is another HEAL landmark project. It involves a network of researchers that is working with judges and with the workers in jail and prison systems responsible for taking care of individuals with substance use disorders. Through this network, we’ve been able to start to harmonize practices. One thing that’s been transformative in the jail and prison system has been the embracing of telehealth. In the past, telehealth was not much of a reality in jails and prisons because of the fear of it could lead to communications that could perhaps be considered dangerous. That’s changed due to COVID-19. Now, telehealth is providing access to treatment for individuals in jail and prison, many of them with substance use disorders.
Also, because of COVID, many nonviolent individuals in jails and prisons were released. This gives us an opportunity to evaluate how best to help such individuals achieve recovery from substance use disorders. Hopefully we can generate data to show that there are much more effective strategies than incarceration for dealing with substance use disorders.
The HEALing Communities Study, involves Massachusetts, New York, Ohio, and Kentucky—four of the states with the highest rates of mortality from overdoses from the inception of the opioid epidemic. By implementing a battery of interventions for which there is evidence of benefit, this ambitious study set out to decrease overdose mortality by 40 percent in two years. Then, came COVID and turned everything upside down. Still, because we consolidated interactions between agencies, we’ve been able to apply support systems more efficiently in those communities in ways that have been very, very reinforcing. Obviously, there’ve been delays in implementation of interventions that require in-person interactions or that involve hospital emergency departments, which have been saturated with COVID patients.
We’ve learned a lot in the process. I may be too optimistic, but I do believe that we can stay on goal.
Collins: Now, I’d like to transition to a few questions from people who subscribe to the HEAL website. Announced at this meeting three years ago, the HEAL Initiative involves research participants and patients and stakeholders—especially people who have lived experience with pain, addiction, or both.
Let’s get to the first question: “What is NIH doing through HEAL to address the stigma that prevents people who need opioid medications for treatment from getting them?”
Volkow: A crucial question. As we look at the issue of stigma, we need to recognize that there are structural issues in how our society is prioritizing the importance of substance use disorders and the investments devoted to them. And we need to recognize that substance use disorder doesn’t exist in isolation; it is frequently comorbid with mental illness.
We need to listen. Some of the issues that we believe are most problematic are not. We need to empower these communities to speak up and help them do so. This is probably one of the most important things that we can do in terms of addressing stigma for addiction.
Collins: Absolutely. The HEAL Initiative has a number of projects that are focusing on stigma and coming up with tools to help reduce this. And here’s our second question: “In small communities, how can we provide more access to medications for opioid use disorder?”
Volkow: One project funded through HEAL was to evaluate the effectiveness of community pharmacies for delivering buprenorphine to individuals with opioid use disorder. The results show that patients receiving buprenorphine through community pharmacies in rural areas had as good outcomes as patients being treated by specialized clinicians on site.
Another change that’s made things easier is that in March 2020, the DEA relaxed its rules on how a physician can prescribe buprenorphine. In the past, you needed to go physically to see a doctor. Now, the DEA allows a patient to be initiated on buprenorphine through telehealth, and that’s opened the possibility of greater access to treatment in rural communities.
My perspective is let’s look at innovative ways of solving problems. Because the technology is changing in so many ways and so rapidly, let’s take advantage of it.
Collins: Totally with you on that. If there’s a silver lining to COVID-19, it’s that we’ve been forced to take stock of the ways we’ve been doing things. We will learn from this pandemic and change the way we approach so many things in health and medicine as a result. Certainly, opioid use disorder ought to be very high on that list. Let’s move on to another question: “What is the HEAL initiative doing to promote prevention of opioid use?”
Volkow: This is where the HEAL initiative is aiming to provide alternative treatments for the management of pain that reduce the risk of addiction.
Then there’s the issue of prevention in people who start to take opioids because they either want to get high or escape. With the COVID pandemic, we’ve seen increases in anxiety and in depression. Those are factors that can put a teenager or young adult on a trajectory for higher risk of substance use disorders.
So, what is HEAL doing? There is prevention research specifically targeted, for example, at the transition from adolescence to young adulthood. That is the period of greatest vulnerability of uptake of opioids, or drugs of misuse. We’re also targeting minority groups that may be at very, very high risk. We want to be able to understand the factors that make them more vulnerable to tailor prevention interventions more effectively.
Collins: Today, we’ve shared some of the issues that NIH is wrestling with in its efforts to address the crisis of opioid misuse and overdose, as well as other drugs that are now very much part of the challenge. To learn more, go to the HEAL website. You can also send us your thoughts through the HEAL Idea Exchange.
These developments give me hope in the wake of a very difficult year. Clearly, we still have the capacity to work together, we are resilient, and we are determined to put an end to our nation’s opioid crisis.
Volkow: Francis, I want to thank you for your incredible leadership and your support. I hope the COVID pandemic will bring forth a more equitable system, in which all people are given the chance for resilience that maximizes their life, happiness, and productivity. I think science is an extraordinary tool to help us do that.
Links:
Video: The 2021 Rx Drug Abuse & Heroin Summit: Francis Collins with Nora Volkow (NIH)
COVID-19 Research (NIH)
Helping to End Addiction Long-term (HEAL) Initiative (NIH)
HEAL Idea Exchange (NIH)
National Institute on Drug Abuse (NIH)
Finding New Ways to Fight Coronavirus … From Studying Bats
Posted on by Dr. Francis Collins

David Veesler has spent nearly 20 years imaging in near-atomic detail the parts of various viruses, including coronaviruses, that enable them to infect Homo sapiens. In fact, his lab at the University of Washington, Seattle, was the first to elucidate the 3D architecture of the now infamous spike protein, which coronaviruses use to gain entry into human cells [1]. He uses these fundamental insights to guide the design of vaccines and therapeutics, including promising monoclonal antibodies.
Now, Veesler and his lab are turning to another mammal in their search for new leads for the next generation of antiviral treatments, including ones aimed at the coronavirus that causes COVID-19, SARS-CoV-2. With support from a 2020 NIH Director’s Pioneer Award, Veesler will study members of the order Chiroptera. Or, more colloquially, bats.
Why bats? Veesler says bats are remarkable creatures. They are the only mammals capable of sustained flight. They rarely get cancer and live unusually long lives for such small creatures. More importantly for Veesler’s research, bats host a wide range of viruses—more than any other mammal species. Despite carrying all of these viruses, bats rarely show symptoms of being sick. Yet they are the source for many of the viruses that have spilled over into humans with devastating effect, including rabies, Ebola virus, Nipah and Hendra viruses, severe acute respiratory syndrome coronavirus (SARS-CoV), and, likely, SARS-CoV-2.
Beyond what is already known about bats’ intriguing qualities, Veesler says humans still have much to discover about these flying mammals, including how their immune systems cope with such an onslaught of viral invaders. For example, it turns out that a bat’s learned, or adaptive, immune system is, for the most part, uncharted territory. As such, it offers an untapped source of potentially promising viral inhibitors just waiting to be unearthed, fully characterized, and then used to guide the development of new kinds of anti-viral therapeutics.
In his studies, Veesler will work with collaborators studying bats around the world to characterize their antibody production. He wants to learn how these antibodies contribute to bats’ impressive ability to tolerate viruses and other pathogens. What is it about the structure of bat antibodies that make them different from human antibodies? And, how can those structural differences serve as blueprints for promising new treatments to combat many potentially deadly viruses?
Interestingly, Veesler’s original grant proposal makes no mention of SARS-CoV-2 or COVID-19. That’s because he submitted it just months before the first reports of the novel coronavirus in Wuhan, China. But Veesler doesn’t consider himself a visionary by expanding his research to bats. He and others had been working on closely related coronaviruses for years, inspired by earlier outbreaks, including SARS in 2002 and Middle East respiratory syndrome (MERS) in 2012 (although MERS apparently came from camels). The researcher didn’t see SARS-CoV-2 coming, but he recognized the potential for some kind of novel coronavirus outbreak in the future.
These days, the Veesler lab has been hard at work to understand SARS-CoV-2 and the human immune response to the virus. His team showed that SARS-CoV-2 uses the human receptor ACE2 to gain entry into our cells [2]. He’s also a member of the international research team that identified a human antibody, called S309, from a person who’d been infected with SARS in 2003. This antibody is showing promise for treating COVID-19 [3], now in a phase 3 clinical trial in the United States.
In another recent study, reported as a pre-print in bioRxiv, Veesler’s team mapped dozens of distinct human antibodies capable of neutralizing SARS-CoV-2 by their ability to hit viral targets outside of the well-known spike protein [4]. Such discoveries may form the basis for new and promising combinations of antibodies to treat COVID-19 that won’t be disabled by concerning new variations in the SARS-CoV-2 spike protein. Perhaps, in the future, such therapeutic cocktails may include modified bat-inspired antibodies too.
References:
[1] Cryo-electron microscopy structure of a coronavirus spike glycoprotein trimer. Walls AC, Tortorici MA, Bosch BJ, Frenz B, Rottier PJM, DiMaio F, Rey FA, Veesler D. Nature. 2016 Mar 3;531(7592):114-117.
[2] Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Cell. 2020 Apr 16;181(2):281-292.e6.
[3] Cross-neutralization of SARS-CoV-2 by a human monoclonal SARS-CoV antibody. Pinto D, Park YJ, Beltramello M, Veesler D, Cortil D, et al. Nature.18 May 2020 [Epub ahead of print]
[4] N-terminal domain antigenic mapping reveals a site of vulnerability for SARS-CoV-2. McCallum M, Marco A, Lempp F, Tortorici MA, Pinto D, Walls AC, Whelan SPJ, Virgin HW, Corti D, Pizzuto MS, Veesler D, et al. bioRxiv. 2021 Jan 14.
Links:
COVID-19 Research (NIH)
Veesler Lab (University of Washington, Seattle)
Veesler Project Information (NIH RePORTER)
NIH Director’s Pioneer Award Program (Common Fund)
NIH Support: Common Fund; National Institute of Allergy and Infectious Diseases
ACTIV Update: Making Major Strides in COVID-19 Therapeutic Development
Posted on by Dr. Francis Collins

Right now, many U.S. hospitals are stretched to the limit trying to help people battling serious cases of COVID-19. But as traumatic as this experience still is for patients and their loved ones, the chances of surviving COVID-19 have in fact significantly improved in the year since the start of the pandemic.
This improvement stems from several factors, including the FDA’s emergency use authorization (EUA) of a number of therapies found to be safe and effective for COVID-19. These include drugs that you may have heard about on the news: remdesivir (an antiviral), dexamethasone (a steroid), and monoclonal antibodies from the companies Eli Lilly and Regeneron.
Yet the quest to save more lives from COVID-19 isn’t even close to being finished, and researchers continue to work intensively to develop new and better treatments. A leader in this critical effort is NIH’s Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) initiative, a public-private partnership involving 20 biopharmaceutical companies, academic experts, and multiple federal agencies.
ACTIV was founded last April to accelerate drug research that typically requires more than a decade of clinical ups and downs to develop a safe, effective therapy. And ACTIV has indeed moved at unprecedented speed since its launch. Cutting through the usual red tape and working with an intense sense of purpose, the partnership took a mere matter of weeks to set up its first four clinical trials. Beyond the agents mentioned above that have already been granted an EUA, ACTIV is testing 15 additional potential agents, with several of these already demonstrating promising results.
Here’s how ACTIV works. The program relies on four expert “working groups” with specific charges:
Preclinical Working Group: Shares standardized preclinical evaluation resources and accelerate testing of candidate therapies and vaccines for clinical trials.
Therapeutics Clinical Working Group: Prioritizes therapeutic agents for testing within an adaptive master protocol strategy for clinical research.
Clinical Trial Capacity Working Group: Has developed and organized an inventory of clinical trial capacity that can serve as potential settings in which to implement effective COVID-19 clinical trials.
Vaccines Working Group: Accelerates the evaluation of vaccine candidates.
To give you just one example of how much these expert bodies have accomplished in record time, the Therapeutics Clinical Working Group got to work immediately evaluating some 400 candidate therapeutics using multiple publicly available information sources. These candidates included antivirals, host-targeted immune modulators, monoclonal antibodies (mAb), and symptomatic/supportive agents including anticoagulants. To follow up on even more new leads, the working group launched a COVID-19 Clinical & Preclinical Candidate Compound Portal, which remains open for submissions of therapeutic ideas and data.
All the candidate agents have been prioritized using rigorous scoring and assessment criteria. What’s more, the working group simultaneously developed master protocols appropriate for each of the drug classes selected and patient populations: outpatient, inpatient, or convalescent.
Through the coordinated efforts of all the working groups, here’s where we stand with the ACTIV trials:
ACTIV-1: A large-scale Phase 3 trial is enrolling hospitalized adults to test the safety and effectiveness of three medicines (cenicriviroc, abatacept, and infliximab). They are called immune modulators because they help to minimize the effects of an overactive immune response in some COVID-19 patients. This response, called a “cytokine storm,” can lead to acute respiratory distress syndrome, multiple organ failure, and other life-threatening complications.
ACTIV-2: A Phase 2/3 trial is enrolling adults with COVID-19 who are not hospitalized to evaluate the safety of multiple monoclonal antibodies (Lilly’s LY-CoV555, Brii Biosciences’s BRII-196 and BRII-198, and AstraZeneca’s AZD7442) used to block or neutralize the SARS-CoV-2 virus. The Lilly monoclonal antibody LY-CoV555 received an EUA for high risk non-hospitalized patients on November 9, 2020 and ACTIV-2 continued to test the agent in an open label study to further determine safety and efficacy in outpatients. Another arm of this trial has just started, testing inhaled, easy-to-administer interferon beta-1a treatment in adults with mild-to-moderate COVID-19 who are not hospitalized. An additional arm will test the drug camostat mesilate, a protease inhibitor that can block the TMPRSS2 host protein that is necessary for viral entry into human cells.
ACTIV-3: This Phase 3 trial is enrolling hospitalized adults with COVID-19. This study primarily aims to evaluate safety and to understand if monoclonal antibodies (AstraZeneca’s AZD7442, BRII-196 and BRII-198, and the VIR-7831 from GSK/Vir Biotechnology) and potentially other types of therapeutics can reduce time to recovery. It also aims to understand a treatment’s effect on extrapulmonary complications and respiratory dysfunction. Lilly’s monoclonal antibody LY-CoV555 was one of the first agents to be tested in this clinical trial and it was determined to not show the same benefits seen in outpatients. [Update: NIH-Sponsored ACTIV-3 Clinical Trial Closes Enrollment into Two Sub-Studies, March 4, 2021]
ACTIV-4: This trial aims to determine if various types of blood thinners, including apixaban, aspirin, and both unfractionated (UF) and low molecular weight (LMW) heparin, can treat adults diagnosed with COVID-19 and prevent life-threatening blood clots from forming. There are actually three Phase 3 trials included in ACTIV-4. One is enrolling people diagnosed with COVID-19 but who are not hospitalized; a second is enrolling patients who are hospitalized; and a third is enrolling people who are recovering from COVID-19. ACTIV-4 has already shown that full doses of heparin blood thinners are safe and effective for moderately ill hospitalized patients.
ACTIV-5: This is a Phase 2 trial testing newly identified agents that might have a major benefit to hospitalized patients with COVID-19, but that need further “proof of concept” testing before they move into a registrational Phase 3 trial. (In fact, another name for this trial is the “Big Effect Trial”.) It is testing medicines previously developed for other conditions that might be beneficial in treatment of COVID-19. The first two agents being tested are risankizumab (the result of a collaboration between Boehringer-Ingelheim), which is already FDA-approved to treat plaque psoriasis, and lenzilumab, which is under development by Humanigen to treat patients experiencing cytokine storm as part of cancer therapy.
In addition to trials conducted under the ACTIV partnership, NIH has prioritized and tested additional therapeutics in “ACTIV-associated trials.” These are NIH-funded, randomized, placebo-controlled clinical trials with one or more industry partners. Here’s a table with a comprehensive list.
Looking a bit further down the road, we also seek to develop orally administered drugs that would potentially block the replication ability of SARS-CoV-2, the coronavirus that causes COVID-19, in the earliest stages of infection. One goal would be to develop an antiviral medication for SARS-CoV-2 that acts similarly to oseltamivir phosphate (Tamiflu®), a drug used to shorten the course of the flu in people who’ve had symptoms for less than two days and to prevent the flu in asymptomatic people who may have been exposed to the influenza virus. Yet another major long-term effort of NIH and its partners will be to develop safe and effective antiviral medications that work against all coronaviruses, even those with variant genomes. (And, yes, such drugs might even cure the common cold!)
So, while our ACTIV partners and many other researchers around the globe continue to harness the power of science to end the devastating COVID-19 pandemic as soon as possible, we must also consider the lessons learned this past year, in order to prepare ourselves to respond more swiftly to future outbreaks of coronaviruses and other infectious disease threats. Our work is clearly a marathon, not a sprint.
Links:
Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) (NIH)
COVID-19 Research (NIH)
Combat COVID (U.S. Department of Health and Human Services, Washington, D.C.)
Pull Up a Chair with Dr. Freire: The COVID Conversations (Foundation for the National Institutes of Health, Bethesda, MD)
SARS-COV-2 Antiviral Therapeutics Summit Report, November 2020 (NIH)
Mapping Which Coronavirus Variants Will Resist Antibody Treatments
Posted on by Dr. Francis Collins

You may have heard about the new variants of SARS-CoV-2—the coronavirus that causes COVID-19—that have appeared in other parts of the world and have now been detected in the United States. These variants, particularly one called B.1.351 that was first identified in South Africa, have raised growing concerns about the extent to which their mutations might help them evade current antibody treatments and highly effective vaccines.
While researchers take a closer look, it’s already possible in the laboratory to predict which mutations will help SARS-CoV-2 evade our therapies and vaccines, and even to prepare for the emergence of new mutations before they occur. In fact, an NIH-funded study, which originally appeared as a bioRxiv pre-print in November and was recently peer-reviewed and published in Science, has done exactly that. In the study, researchers mapped all possible mutations that would allow SARS-CoV-2 to resist treatment with three different monoclonal antibodies developed for treatment of COVID-19 [1].
The work, led by Jesse Bloom, Allison Greaney, and Tyler Starr, Fred Hutchinson Cancer Center, Seattle, focused on the receptor binding domain (RBD), a key region of the spike protein that studs SARS-CoV-2’s outer surface. The virus uses RBD to anchor itself to the ACE2 receptor of human cells before infecting them. That makes the RBD a prime target for the antibodies that our bodies generate to defend against the virus.
In the new study, researchers used a method called deep mutational scanning to find out which mutations positively or negatively influence the RBD from being able to bind to ACE2 and/or thwart antibodies from striking their target. Here’s how it works: Rather than waiting for new mutations to arise, the researchers created a library of RBD fragments, each of which contained a change in a single nucleotide “letter” that would alter the spike protein’s shape and/or function by swapping one amino acid for another. It turns out that there are more than 3,800 such possible mutations, and Bloom’s team managed to make all but a handful of those versions of the RBD fragment.
The team then used a standard laboratory approach to measure systematically how each of those single-letter typos altered RBD’s ability to bind ACE2 and infect human cells. They also measured how those changes affected three different therapeutic antibodies from recognizing and binding to the viral RBD. Those antibodies include two developed by Regeneron (REGN10933 and REGN10987), which have been granted emergency use authorization for treatment of COVID-19 together as a cocktail called REGN-COV2. They also looked at an antibody developed by Eli Lilly (LY-CoV016), which is now in phase 3 clinical trials for treating COVID-19.
Based on the data, the researchers created four mutational maps for SARS-CoV-2 to escape each of the three therapeutic antibodies, as well as for the REGN-COV2 cocktail. Their studies show most of the mutations that would allow SARS-CoV-2 to escape treatment differed between the two Regeneron antibodies. That’s encouraging because it indicates that the virus likely needs more than one mutation to become resistant to the REGN-COV2 cocktail. However, it appears there’s one spot where a single mutation could allow the virus to resist REGN-COV2 treatment.
The escape map for LY-CoV016 similarly showed a number of mutations that could allow the virus to escape. Importantly, while some of those changes might impair the virus’s ability to cause infection, most of them appeared to come at little to no cost to the virus to reproduce.
How do these laboratory data relate to the real world? To begin to explore this question, the researchers teamed up with Jonathan Li, Brigham and Women’s Hospital, Boston. They looked at an immunocompromised patient who’d had COVID-19 for an unusually long time and who was treated with the Regeneron cocktail for 145 days, giving the virus time to replicate and acquire new mutations.
Viral genome data from the infected patient showed that these maps can indeed be used to predict likely paths of viral evolution. Over the course of the antibody treatment, SARS-CoV-2 showed changes in the frequency of five mutations that would change the makeup of the spike protein and its RBD. Based on the newly drawn escape maps, three of those five are expected to reduce the efficacy of REGN10933. One of the others is expected to limit binding by the other antibody, REGN10987.
The researchers also looked to data from all known circulating SARS-CoV-2 variants as of Jan. 11, 2021, for evidence of escape mutations. They found that a substantial number of mutations with potential to allow escape from antibody treatment already are present, particularly in parts of Europe and South Africa.
However, it’s important to note that these maps reflect just three important antibody treatments. Bloom says they’ll continue to produce maps for other promising therapeutic antibodies. They’ll also continue to explore where changes in the virus could allow for escape from the more diverse set of antibodies produced by our immune system after a COVID-19 infection or vaccination.
While it’s possible some COVID-19 vaccines may offer less protection against some of these new variants—and recent results have suggested the AstraZeneca vaccine may not provide much protection against the South African variant, there’s still enough protection in most other current vaccines to prevent serious illness, hospitalization, and death. And the best way to keep SARS-CoV-2 from finding new ways to escape our ongoing efforts to end this terrible pandemic is to double down on whatever we can do to prevent the virus from multiplying and spreading in the first place.
For now, emergence of these new variants should encourage all of us to take steps to slow the spread of SARS-CoV-2. That means following the three W’s: Wear a mask, Watch your distance, Wash your hands often. It also means rolling up our sleeves to get vaccinated as soon as the opportunity arises.
Reference:
[1] Prospective mapping of viral mutations that escape antibodies used to treat COVID-19.
Starr TN, Greaney AJ, Addetia A, Hannon WW, Choudhary MC, Dingens AS, Li JZ, Bloom JD.
Science. 2021 Jan 25:eabf9302.
Links:
COVID-19 Research (NIH)
Bloom Lab (Fred Hutchinson Cancer Center, Seattle)
NIH Support: National Institute of Allergy and Infectious Diseases
Reasons for Gratitude Amid the COVID-19 Pandemic
Posted on by Dr. Francis Collins

For many of us, Thanksgiving will feel really different this year. Less will need to be more, as we celebrate alone or with our immediate household members to stay safe and help combat the surge in COVID-19 cases across most of the land. And yet, times of trouble can also help us to focus on what’s really important in our lives. So, even as we face these challenges and the range of emotions that arise with them, it’s worth remembering that this Thanksgiving, there remain many reasons to be grateful.
I’m certainly grateful for a loving family and friends that provide depth and meaning to life, even though most of us can’t be physically together and hug each other right now. My faith is also a source of comfort and reassurance at this time. I also feel a deep sense of gratitude for everyone who has sacrificed for the common good over the last several months, especially those who’ve masked up and physically distanced to provide essential services in our communities to keep everything going. You will no doubt have your own list of heroes, but here are just a few of mine:
• Healthcare workers, thanks for all you do under such difficult and dangerous conditions.
• Essential workers, thanks for clocking in every day. That includes bus drivers, grocery store cashiers, waste collectors, tradespeople, firefighters, law enforcement officers, and all those who deliver packages to my door.
• Teachers, working remotely or in person. Thanks for your commitment to our students and continuing to bring out the best in them.
• Parents, including so many now working with kids at home. Thanks for juggling responsibilities and making everything work.
• Clinical trials participants. Your participation is critical for developing treatments and vaccines. Thanks to you all, including the fine examples of many public figures, including the trial participation of Senator Rob Portman and financial contribution of legendary performer Dolly Parton.
• Everyone following the 3 W’s: Wear a mask, Watch your distance, and Wash your hands. Thank you for doing your part every day to keep yourself, your loved ones, and your community safe. You are our front lines in the battle.
• Researchers, from both the public and private sectors, who are working in partnership all around the world. Our shared goal is to learn all we can about COVID-19 and to develop better tests, new treatments, and safe and effective vaccines.
On that note, you may have heard about the very promising interim clinical trial results of an investigational COVID-19 vaccine known as mRNA-1273, co-developed by the biotechnology company Moderna, Cambridge, MA, and NIH’s National Institute of Allergy and Infectious Diseases. That mRNA vaccine was found to be 94.5 percent effective in preventing symptomatic COVID-19. Another mRNA vaccine, developed by Pfizer and BioNTech, also recently was shown to be 95 percent effective and has now submitted an application for emergency use authorization (EUA) to the Food and Drug Administration (FDA). In addition, AstraZeneca announced that, in a late-stage clinical trial, the vaccine it developed in partnership with the University of Oxford reduced the risk of COVID-19 infection by an average of 70 percent, with up to 90 percent efficacy in one dosing regimen.
Other promising vaccine candidates continue to work their way through clinical trials, and we’ll no doubt be hearing more about those soon. It is truly remarkable to accomplish in 10 months what normally takes about 8 years. Therapeutic progress is also moving forward rapidly, with a second monoclonal antibody treatment for high-risk outpatients receiving emergency use authorization from the FDA just a few days ago.
For all of these advances, I am immensely grateful. Of course, it will take time and continued study to get a COVID-19 vaccine fully approved and distributed to all those who need it. The success of any vaccine also will hinge on people across the country—including you and all those whom I’ve recognized here—making the choice to protect themselves and others by getting vaccinated against COVID-19.
As we look ahead to that day when the COVID-19 pandemic is under control, I encourage you to take some time to jot down your own list of reasons to be grateful. Encourage family members to do the same and take some time to share them with one another, whether it’s around the table or by email, phone, or videoconferencing. The holidays are a time for making memories and—as different as it may look—this year is no different. So, while you’re enjoying your Thanksgiving meal around a smaller table, remember that you’re doing it from a place of love and gratitude. I wish for you a safe and happy Thanksgiving.
Links:
Coronavirus (COVID) (NIH)
Your Health: Holiday Celebrations and Small Gatherings (Centers for Disease Control and Prevention, Atlanta)
Charting a Rapid Course Toward Better COVID-19 Tests and Treatments
Posted on by Dr. Francis Collins

It is becoming apparent that our country is entering a new and troubling phase of the pandemic as SARS-CoV-2, the novel coronavirus that causes COVID-19, continues to spread across many states and reaches into both urban and rural communities. This growing community spread is hard to track because up to 40 percent of infected people seem to have no symptoms. They can pass the virus quickly and unsuspectingly to friends and family members who might be more vulnerable to becoming seriously ill. That’s why we should all be wearing masks when we go out of the house—none of us can be sure we’re not that asymptomatic carrier of the virus.
This new phase makes fast, accessible, affordable diagnostic testing a critical first step in helping people and communities. In recognition of this need, NIH’s Rapid Acceleration of Diagnostics (RADx) initiative, just initiated in late April, has issued an urgent call to the nation’s inventors and innovators to develop fast, easy-to-use tests for SARS-CoV-2, the novel coronavirus that causes COVID-19. It brought a tremendous response, and NIH selected about 100 of the best concepts for an intense one-week “shark-tank” technology evaluation process.
Moving ahead at an unprecedented pace, NIH last week announced the first RADx projects to come through the deep dive with flying colors and enter the scale-up process necessary to provide additional rapid testing capacity to the U.S. public. As part of the RADx initiative, seven biomedical technology companies will receive a total of $248.7 million in federal stimulus funding to accelerate their efforts to scale up new lab-based and point-of-care technologies.
Four of these projects will aim to bolster the nation’s lab-based COVID-19 diagnostics capacity by tens of thousands of tests per day as soon as September and by millions by the end of the year. The other three will expand point-of-care testing for COVID-19, making results more rapidly and readily available in doctor’s offices, urgent care clinics, long-term care facilities, schools, child care centers, or even at home.
This is only a start, and we expect that more RADx projects will advance in the coming months and begin scaling up for wide-scale use. In the meantime, here’s an overview of the first seven projects developed through the initiative, which NIH is carrying out in partnership with the Office of the Assistant Secretary of Health, the Biomedical Advanced Research and Development Authority, and the Department of Defense:
Point-of-Care Testing Approaches
Mesa Biotech. Hand-held testing device detects the genetic material of SARS-CoV-2. Results are read from a removable, single-use cartridge in 30 minutes.
Quidel. Test kit detects protein (viral antigen) from SARS-CoV-2. Electronic analyzers provide results within 15 minutes. The U.S. Department of Health and Human Service has identified this technology for possible use in nursing homes.
Talis Biomedical. Compact testing instrument uses a multiplexed cartridge to detect the genetic material of SARS-CoV-2 through isothermal amplification. Optical detection system delivers results in under 30 minutes.
Lab-based Testing Approaches
Ginkgo Bioworks. Automated system uses next-generation sequencing to scan patient samples for SARS-CoV-2’s genetic material. This system will be scaled up to make it possible to process tens of thousands of tests simultaneously and deliver results within one to two days. The company’s goal is to scale up to 50,000 tests per day in September and 100,000 per day by the end of 2020.
Helix OpCo. By combining bulk shipping of test kits and patient samples, automation, and next-generation sequencing of genetic material, the company’s goal is to process up to 50,000 samples per day by the end of September and 100,000 per day by the end of 2020.
Fluidigm. Microfluidics platform with the capacity to process thousands of polymerase chain reaction (PCR) tests for SARS-CoV-2 genetic material per day. The company’s goal is to scale up this platform and deploy advanced integrated fluidic chips to provide tens to hundreds of thousands of new tests per day in the fall of 2020. Most tests will use saliva.
Mammoth Biosciences. System uses innovative CRISPR gene-editing technology to detect key pieces of SARS-CoV-2 genetic material in patient samples. The company’s goal is to provide a multi-fold increase in testing capacity in commercial laboratories.
At the same time, on the treatment front, significant strides continue to be made by a remarkable public-private partnership called Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV). Since its formation in May, the partnership, which involves 20 biopharmaceutical companies, academic experts, and multiple federal agencies, has evaluated hundreds of therapeutic agents with potential application for COVID-19 and prioritized the most promising candidates.
Among the most exciting approaches are monoclonal antibodies (mAbs), which are biologic drugs derived from neutralizing antibodies isolated from people who’ve survived COVID-19. This week, the partnership launched two trials (one for COVID-19 inpatients, the other for COVID-19 outpatients) of a mAB called LY-CoV555, which was developed by Eli Lilly and Company, Indianapolis, IN. It was discovered by Lilly’s development partner AbCellera Biologics Inc. Vancouver, Canada, in collaboration with the NIH’s National Institute of Allergy and Infectious Diseases (NIAID). In addition to the support from ACTIV, both of the newly launched studies also receive support for Operation Warp Speed, the government’s multi-agency effort against COVID-19.
LY-CoV555 was derived from the immune cells of one of the very first survivors of COVID-19 in the United States. It targets the spike protein on the surface of SARS-CoV-2, blocking it from attaching to human cells.
The first trial, which will look at both the safety and efficacy of the mAb for treating COVID-19, will involve about 300 individuals with mild to moderate COVID-19 who are hospitalized at facilities that are part of existing clinical trial networks. These volunteers will receive either an intravenous infusion of LY-CoV555 or a placebo solution. Five days later, their condition will be evaluated. If the initial data indicate that LY-CoV555 is safe and effective, the trial will transition immediately—and seamlessly—to enrolling an additional 700 participants with COVID-19, including some who are severely ill.
The second trial, which will evaluate how LY-CoV555 affects the early course of COVID-19, will involve 220 individuals with mild to moderate COVID-19 who don’t need to be hospitalized. In this study, participants will randomly receive either an intravenous infusion of LY-CoV555 or a placebo solution, and will be carefully monitored over the next 28 days. If the data indicate that LY-CoV555 is safe and shortens the course of COVID-19, the trial will then enroll an additional 1,780 outpatient volunteers and transition to a study that will more broadly evaluate its effectiveness.
Both trials are later expected to expand to include other experimental therapies under the same master study protocol. Master protocols allow coordinated and efficient evaluation of multiple investigational agents at multiple sites as the agents become available. These protocols are designed with a flexible, rapidly responsive framework to identify interventions that work, while reducing administrative burden and cost.
In addition, Lilly this week started a separate large-scale safety and efficacy trial to see if LY-CoV555 can be used to prevent COVID-19 in high-risk residents and staff at long-term care facilities. The study isn’t part of ACTIV.
NIH-funded researchers have been extremely busy over the past seven months, pursuing every avenue we can to detect, treat, and, ultimately, end this devasting pandemic. Far more work remains to be done, but as RADx and ACTIV exemplify, we’re making rapid progress through collaboration and a strong, sustained investment in scientific innovation.
Links:
Coronavirus (COVID-19) (NIH)
Rapid Acceleration of Diagnostics (RADx)
Video: NIH RADx Delivering New COVID-19 Testing Technologies to Meet U.S. Demand (YouTube)
Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV)
Explaining Operation Warp Speed (U.S. Department of Health and Human Resources/Washington, D.C.)
“NIH delivering new COVID-19 testing technologies to meet U.S. demand,” NIH news release,” July 31, 2020.
“NIH launches clinical trial to test antibody treatment in hospitalized COVID-19 patients,” NIH new release, August 4, 2020.
“NIH clinical trial to test antibodies and other experimental therapeutics for mild and moderate COVID-19,” NIH news release, August 4, 2020.
Finding Antibodies that Neutralize SARS-CoV-2
Posted on by Dr. Francis Collins

It’s now clear that nearly everyone who recovers from coronavirus disease 2019 (COVID-19) produces antibodies that specifically target SARS-CoV-2, the novel coronavirus that causes the infection. Yet many critical questions remain. A major one is: just how well do those particular antibodies neutralize the virus to fight off the infection and help someone recover from COVID-19? Fortunately, most people get better—but should the typical antibody response take the credit?
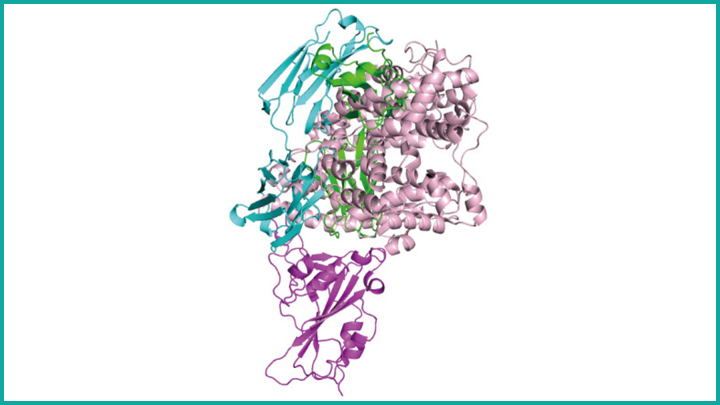
A new NIH-funded study of nearly 150 people who recovered from COVID-19 offers some essential insight. The study, published in the journal Nature, shows that most people, in fact, do produce antibodies that can effectively neutralize SARS-CoV-2. But there is a catch: 99 percent of the study’s participants didn’t make enough neutralizing antibodies to mount an ideal immune response.
The good news is that when researchers looked at individuals who mounted a strong immune response, they were able to identify three antibodies (depicted above) that were extremely effective at neutralizing SARS-CoV-2. By mass-producing copies of these antibodies as so-called monoclonal antibodies, the researchers can now better evaluate their potential as treatments to help people who don’t make strongly neutralizing antibodies, or not enough of them.
These findings come from a team led by Michel Nussenzweig, Paul Bieniasz, and Charles Rice at The Rockefeller University, New York, and Pamela Bjorkman at the California Institute of Technology, Pasadena. In the Nussenzweig lab, the team has spent years searching for broadly neutralizing antibodies against the human immunodeficiency virus (HIV). In response to the COVID-19 pandemic and its great urgency, Nussenzweig and team shifted their focus recently to look for promising antibodies against SARS-CoV-2.
Antibodies are blood proteins that the immune system makes to neutralize viruses or other foreign invaders. The immune system doesn’t make just one antibody to thwart an invader; it makes a whole family of antibodies. But not all antibodies in that family are created equal. They can vary widely in where they latch onto a virus like SARS-CoV-2, and that determines how effective each will be at blocking it from infecting human cells. That’s one reason why people respond differently to infections such as COVID-19.
In early April, Nussenzweig’s team began analyzing samples from volunteer survivors who visited The Rockefeller Hospital to donate plasma, which contains the antibodies. The volunteers had all recovered from mild-to-severe cases of COVID-19, showing their first signs of illness about 40 days prior to their first plasma collection.
Not surprisingly, all volunteers had produced antibodies in response to the virus. To test the strength of the antibodies, the researchers used a special assay that shows how effective each one is at blocking the virus from infecting human cells in lab dishes.
Overall, most of the plasma samples—118 of 149—showed at best poor to modest neutralizing activity. In about one-third of individuals, their plasma samples had below detectable levels of neutralizing activity. It’s possible those individuals just resolved the infection quickly, before more potent antibodies were produced.
More intriguing to the researchers were the results from two individuals that showed an unusually strong ability to neutralize SARS-CoV-2. Among these two “elite responders” and four other individuals, the researchers identified 40 different antibodies that could neutralize SARS-CoV-2. But again, not all antibodies are created equal. Three neutralized the virus even when present at extremely low levels, and they now will be studied further as possible monoclonal antibodies.
The team determined that those strongly neutralizing antibodies bind three distinct sites on the receptor-binding domain (RBD) of the coronavirus spike protein. This portion of the virus is important because it allows SARS-CoV-2 to bind and infect human cells. Importantly, when the researchers looked more closely at plasma samples with poor neutralizing ability, they found that they also contained those RBD-binding antibodies, just not in very large numbers.
These findings help not only to understand the immune response to COVID-19, they are also critical for vaccine design, revealing what a strong neutralizing antibody for SARS-CoV-2 should look like to help the immune system win. If a candidate vaccine can generate such strongly neutralizing antibodies, researchers will know that they are on the right track.
While this research showed that there’s a lot of variability in immune responses to SARS-CoV-2, it appears that most of us are inherently capable of producing antibodies to neutralize this devastating virus. That brings more reason for hope that the many vaccines now under study to elicit such neutralizing antibodies in sufficient numbers may afford us with much-needed immune protection.
Reference:
[1] Convergent antibody responses to SARS-CoV-2 in convalescent individuals. Robbiani DF, Gaebler C, Muecksch F, et al. Nature. 2020 Jun 18. [Published online ahead of print].
Links:
Coronavirus (COVID-19) (NIH)
Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV)
Nussenzweig Lab (The Rockefeller University, New York)
Bjorkman Lab (California Institute of Technology, Pasadena)
NIH Support: National Institute of Allergy and Infectious Diseases
Discussing the Need for Reliable Antibody Testing for COVID-19
Posted on by Dr. Francis Collins

There’s been a great deal of discussion about whether people who recover from coronavirus disease 2019 (COVID-19), have neutralizing antibodies in their bloodstream to guard against another infection. Lots of interesting data continue to emerge, including a recent preprint from researchers at Sherman Abrams Laboratory, Brooklyn, NY [1]. They tested 11,092 people for antibodies in May at a local urgent care facility and found nearly half had long-lasting IgG antibodies, a sign of exposure to the novel coronavirus SARS-CoV-2, the cause of COVID-19. The researchers also found a direct correlation between the severity of a person’s symptoms and their levels of IgG antibodies.
This study and others remind us of just how essential antibody tests will be going forward to learn more about this challenging pandemic. These assays must have high sensitivity and specificity, meaning there would be few false negatives and false positives, to tell us more about a person’s exposure to SARS-CoV-2. While there are some good tests out there, not all are equally reliable.
Recently, I had a chance to discuss COVID-19 antibody tests, also called serology tests, with Dr. Norman “Ned” Sharpless, Director of NIH’s National Cancer Institute (NCI). Among his many talents, Dr. Sharpless is an expert on antibody testing for COVID-19. You might wonder how NCI got involved in COVID-19 testing. Well, you’re going to find out. Our conversation took place while videoconferencing, with him connecting from North Carolina and me linking in from my home in Maryland. Here’s a condensed transcript of our chat:
Collins: Ned, thanks for joining me. Maybe we should start with the basics. What are antibodies anyway?
Sharpless: Antibodies are proteins that your body makes as part of the learned immune system. It’s the immunity that responds to a bacterium or a virus. In general, if you draw someone’s blood after an infection and test it for the presence of these antibodies, you can often know whether they’ve been infected. Antibodies can hang around for quite a while. How long exactly is a topic of great interest, especially in terms of the COVID-19 pandemic. But we think most people infected with coronavirus will make antibodies at a reasonably high level, or titer, in their peripheral blood within a couple of weeks of the infection.
Collins: What do antibodies tell us about exposure to a virus?
Sharpless: A lot of people with coronavirus are infected without ever knowing it. You can use these antibody assays to try and tell how many people in an area have been infected, that is, you can do a so-called seroprevalence survey.
You could also potentially use these antibody assays to predict someone’s resistance to future infection. If you cleared the infection and established immunity to it, you might be resistant to future infection. That might be very useful information. Maybe you could make a decision about how to go out in the community. So, that part is of intense interest as well, although less scientifically sound at the moment.
Collins: I have a 3D-printed model of SARS-CoV-2 on my desk. It’s sort of a spherical virus that has spike proteins on its surface. Do the antibodies interact with the virus in some specific ways?
Sharpless: Yes, antibodies are shaped like the letter Y. They have two binding domains at the head of each Y that will recognize something about the virus. We find antibodies in the peripheral blood that recognize either the virus nucleocapsid, which is the structural protein on the inside; or the spikes, which stick out and give coronavirus its name. We know now that about 99 percent of people who get infected with the virus will develop antibodies eventually. Most of those antibodies that you can detect to the spike proteins will be neutralizing, which means they can kill the virus in a laboratory experiment. We know from other viruses that, generally, having neutralizing antibodies is a promising sign if you want to be immune to that virus in the future.
Collins: Are COVID-19 antibodies protective? Are there reports of people who’ve gotten better, but then were re-exposed and got sick again?
Sharpless: It’s controversial. People can shed the virus’s nucleic acid [genetic material], for weeks or even more than a month after they get better. So, if they have another nucleic acid test it could be positive, even though they feel better. Often, those people aren’t making a lot of live virus, so it may be that they never stopped shedding the virus. Or it may be that they got re-infected. It’s hard to understand what that means exactly. If you think about how many people worldwide have had COVID-19, the number of legitimate possible reinfection cases is in the order of a handful. So, it’s a pretty rare event, if it happens at all.
Collins: For somebody who does have the antibodies, who apparently was previously infected, do they need to stop worrying about getting exposed? Can they can do whatever they want and stop worrying about distancing and wearing masks?
Sharpless: No, not yet. To use antibodies to predict who’s likely to be immune, you’ve got to know two things.
First: can the tests actually measure antibodies reliably? I think there are assays available to the public that are sufficiently good for asking this question, with an important caveat. If you’re trying to detect something that’s really rare in a population, then any test is going to have limitations. But if you’re trying to detect something that’s more common, as the virus was during the recent outbreak in Manhattan, I think the tests are up to the task.
Second: does the appearance of an antibody in the peripheral blood mean that you’re actually immune or you’re just less likely to get the virus? We don’t know the answer to that yet.
Collins: Let’s be optimistic, because it sounds like there’s some evidence to support the idea that people who develop these antibodies are protected against infection. It also sounds like the tests, at least some of them, are pretty good. But if there is protection, how long would you expect it to last? Is this one of those things where you’re all set for life? Or is this going to be something where somebody’s had it and might get it again two or three years from now, because the immunity faded away?
Sharpless: Since we have no direct experience with this virus over time, it’s hard to answer. The potential for this cell-based humoral immunity to last for a while is there. For some viruses, you have a long-lasting antibody protection after infection; for other viruses, not so much.
So that’s the unknown thing. Is immunity going to last for a while? Of course, if one were to bring up the topic of vaccines, that’s very important to know, because you would want to know how often one would have to give that vaccine, even under optimal circumstances.
Collins: Yes, our conversation about immunity is really relevant to the vaccines we’re trying to develop right now. Will these vaccines be protective for long periods of time? We sure hope so, but we’ve got to look carefully at the issue. Let’s come back, though, to the actual performance of the tests. The NCI has been right in the middle of trying to do this kind of validation. How did that happen, and how did that experience go?
Sharpless: Yes, I think one might ask: why is the National Cancer Institute testing antibody kits for the FDA? It is unusual, but certainly not unheard of, for NCI to take up problems like this during a time of a national emergency. During the HIV era, NCI scientists, along with others, identified the virus and did one of the first successful compound screens to find the drug AZT, one of the first effective anti-HIV therapies.
NCI’s Frederick National Lab also has a really good serology lab that had been predominantly working on human papillomavirus (HPV). When the need arose for serologic testing a few months ago, we pivoted that lab to a coronavirus serology lab. It took us a little while, but eventually we rounded up everything you needed to create positive and negative reference panels for antibody testing.
At that time, the FDA had about 200 manufacturers making serology tests that hoped for approval to sell. The FDA wanted some performance testing of those assays by a dispassionate third party. The Frederick National Lab seemed like the ideal place, and the manufacturers started sending us kits. I think we’ve probably tested on the order of 20 so far. We give those data back to the FDA for regulatory decision making. They’re putting all the data online.
Collins: How did it look? Are these all good tests or were there some clunkers?
Sharpless: There were some clunkers. But we were pleased to see that some of the tests appear to be really good, both in our hands and those of other groups, and have been used in thousands of patients.
There are a few tests that have sensitivities that are pretty high and specificities well over 99 percent. The Roche assay has a 99.8 percent specificity claimed on thousands of patients, and for the Mt. Sinai assay developed and tested by our academic collaborators in a panel of maybe 4,000 patients, they’re not sure they’ve ever had a false positive. So, there are some assays out there that are good.
Collins: There’s been talk about how there will soon be monoclonal antibodies directed against SARS-CoV-2. How are those derived?
Sharpless: They’re picked, generally, for appearing to have neutralizing activity. When a person makes antibodies, they don’t make one antibody to a pathogen. They make a whole family of them. And those can be individually isolated, so you can know which antibodies made by a convalescent individual really have virus-neutralizing capacity. That portion of the antibody that recognizes the virus can be engineered into a manufacturing platform to make monoclonal antibodies. Monoclonal means one kind of antibody. That approach has worked for other infectious diseases and is an interesting idea here too.
Collins: I can say a bit about that, because we are engaged in a partnership with industry and FDA called Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV). One of the hottest ideas right now is monoclonal antibodies, and we’re in the process of devising a master protocol, one for outpatients and one for inpatients.
Janet Woodcock of Operation Warp Speed tells me 21 companies are developing monoclonal antibodies. While doing these trials, we’d love to do comparisons, which is why it’s good to have an organization like ACTIV to bring everybody together, making sure you’re using the same endpoints and the same laboratory measures. I think that, maybe even by late summer, we might have some results. For people who are looking at what’s the next most-hopeful therapeutic option for people who are really sick with COVID-19, so far we have remdesivir. It helps, but it’s not a home run. Maybe monoclonal antibodies will be the next thing that really gives a big boost in survival. That would be the hope.
Ned, let me ask you one final question about herd, or group, immunity. One hears a bit about that in terms of how we are all going to get past this COVID-19 pandemic. What’s that all about?
Sharpless: Herd immunity is when a significant portion of the population is immune to a pathogen, then that pathogen will die out in the population. There just aren’t enough susceptible people left to infect. What the threshold is for herd immunity depends on how infectious the virus is. For a highly infectious virus, like measles, maybe up to 90 percent of the population must be immune to get herd immunity. Whereas for other less-infectious viruses, it may only be 50 percent of the population that needs to be immune to get herd immunity. It’s a theoretical thing that makes some assumptions, such as that everybody’s health status is the same and the population mixes perfectly every day. Neither of those are true.
How well that actual predictive number will work for coronavirus is unknown. The other thing that’s interesting is a lot of that work has been based on vaccines, such as what percentage do you have to vaccinate to get herd immunity? But if you get to herd immunity by having people get infected, so-called natural herd immunity, that may be different. You would imagine the most susceptible people get infected soonest, and so the heterogeneity of the population might change the threshold calculation.
The short answer is nobody wants to find out. No one wants to get to herd immunity for COVID-19 through natural herd immunity. The way you’d like to get there is with a vaccine that you then could apply to a large portion of the population, and have them acquire immunity in a more safe and controlled manner. Should we have an efficacious vaccine, this question will loom large: how many people do we need to vaccinate to really try and protect vulnerable populations?
Collins: That’s going to be a really critical question for the coming months, as the first large-scale vaccine trials get underway in July, and we start to see how they work and how successful and safe they are. But I’m also worried seeing some reports that 1 out of 5 Americans say they wouldn’t take a vaccine. It would be truly a tragedy if we have a safe and effective vaccine, but we don’t get enough uptake to achieve herd immunity. So, we’ve got some work to do on all fronts, that’s for sure.
Ned, I want to thank you for sharing all this information about antibodies and serologies and other things, as well as thank you for your hard work with all your amazing NCI colleagues.
Sharpless: Thanks for having me.
Reference:
[1] SARS-CoV-2 IgG Antibody Responses in New York City. Reifer J, Hayum N, Heszkel B, Klagsbald I, Streva VA. medRxiv. Preprint posted May 26, 2020.
Links:
Coronavirus (COVID-19) (NIH)
At NCI, A Robust and Rapid Response to the COVID-19 Pandemic. Norman E. Sharpless. Cancer Currents Blog. April 17, 2020 (National Cancer Institute/NIH)
Serological Testing for SARS-CoV-2 Antibodies (American Medical Association, Chicago)
COVID-19 Antibody Testing Primer (Infectious Diseases Society of America, Arlington, VA)
Accelerating COVID-19 Therapeutic Interventions and Vaccines (NIH)
Enlisting Monoclonal Antibodies in the Fight Against COVID-19
Posted on by Dr. Francis Collins
We now know that the immune system of nearly everyone who recovers from COVID-19 produces antibodies against SARS-CoV-2, the novel coronavirus that causes this easily transmitted respiratory disease [1]. The presence of such antibodies has spurred hope that people exposed to SARS-CoV-2 may be protected, at least for a time, from getting COVID-19 again. But, in this post, I want to examine another potential use of antibodies: their promise for being developed as therapeutics for people who are sick with COVID-19.
In a recent paper in the journal Science, researchers used blood drawn from a COVID-19 survivor to identify a pair of previously unknown antibodies that specifically block SARS-CoV-2 from attaching to human cells [2]. Because each antibody locks onto a slightly different place on SARS-CoV-2, the vision is to use these antibodies in combination to block the virus from entering cells, thereby curbing COVID-19’s destructive spread throughout the lungs and other parts of the body.
The research team, led by Yan Wu, Capital Medical University, Beijing, first isolated the pair of antibodies in the laboratory, starting with white blood cells from the patient. They were then able to produce many identical copies of each antibody, referred to as monoclonal antibodies. Next, these monoclonal antibodies were simultaneously infused into a mouse model that had been infected with SARS-CoV-2. Just one infusion of this combination antibody therapy lowered the amount of viral genetic material in the animals’ lungs by as much as 30 percent compared to the amount in untreated animals.
Monoclonal antibodies are currently used to treat a variety of conditions, including asthma, cancer, Crohn’s disease, and rheumatoid arthritis. One advantage of this class of therapeutics is that the timelines for their development, testing, and approval are typically shorter than those for drugs made of chemical compounds, called small molecules. Because of these and other factors, many experts think antibody-based therapies may offer one of the best near-term options for developing safe, effective treatments for COVID-19.
So, what exactly led up to this latest scientific achievement? The researchers started out with a snippet of SARS-CoV-2’s receptor binding domain (RBD), a vital part of the spike protein that protrudes from the virus’s surface and serves to dock the virus onto an ACE2 receptor on a human cell. In laboratory experiments, the researchers used the RBD snippet as “bait” to attract antibody-producing B cells in a blood sample obtained from the COVID-19 survivor. Altogether, the researchers identified four unique antibodies, but two, which they called B38 and H4, displayed a synergistic action in binding to the RBD that made them stand out for purposes of therapeutic development and further testing.
To complement their lab and animal experiments, the researchers used a particle accelerator called a synchrotron to map, at near-atomic resolution, the way in which the B38 antibody locks onto its viral target. This structural information helps to clarify the precise biochemistry of the complex interaction between SARS-CoV-2 and the antibody, providing a much-needed guide for the rational design of targeted drugs and vaccines. While more research is needed before this or other monoclonal antibody therapies can be used in humans suffering from COVID-19, the new work represents yet another example of how basic science is expanding fundamental knowledge to advance therapeutic discovery for a wide range of health concerns.
Meanwhile, there’s been other impressive recent progress towards the development of monoclonal antibody therapies for COVID-19. In work described in the journal Nature, an international research team started with a set of neutralizing antibodies previously identified in a blood sample from a person who’d recovered from a different coronavirus-caused disease, called severe acute respiratory syndrome (SARS), in 2003 [3]. Through laboratory and structural imaging studies, the researchers found that one of these antibodies, called S309, proved particularly effective at neutralizing the coronavirus that causes COVID-19, SARS-CoV-2, because of its potent ability to target the spike protein that enables the virus to enter cells. The team, which includes NIH grantees David Veesler, University of Washington, Seattle, and Davide Corti, Humabs Biomed, a subsidiary of Vir Biotechnology, has indicated that S309 is already on an accelerated development path toward clinical trials.
In the U.S. and Europe, the Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) partnership, which has brought together public and private sector COVID-19 therapeutic and vaccine efforts, is intensely pursuing the development and testing of therapeutic monoclonal antibodies for COVID-19 [4]. Stay tuned for more information about these potentially significant advances in the next few months.
References:
[1] Humoral immune response and prolonged PCR positivity in a cohort of 1343 SARS-CoV 2 patients in the New York City region. Wajnberg A , Mansour M, Leven E, Bouvier NM, Patel G, Firpo A, Mendu R, Jhang J, Arinsburg S, Gitman M, Houldsworth J, Baine I, Simon V, Aberg J, Krammer F, Reich D, Cordon-Cardo C. medRxiv. Preprint Posted May 5, 2020.
[2] A noncompeting pair of human neutralizing antibodies block COVID-19 virus binding to its receptor ACE2. Wu Y. et al., Science. 13 May 2020 [Epub ahead of publication]
[3] Cross-neutralization of SARS-CoV-2 by a human monoclonal SARS-CoV antibody. Pinto D, Park YJ, Beltramello M, Veesler D, Cortil D, et al. Nature. 18 May 2020 [Epub ahead of print]
[4] Accelerating COVID-19 therapeutic interventions and vaccines (ACTIV): An unprecedented partnership for unprecedented times. Collins FS, Stoffels P. JAMA. 2020 May 18.
Links:
Coronavirus (COVID-19) (NIH)
Monoclonal Antibodies (National Cancer Institute/NIH)
Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV)
NIH Support: National Institute of Allergy and Infectious Diseases; National Institute of General Medical Sciences
Precision Oncology: Gene Changes Predict Immunotherapy Response
Posted on by Dr. Francis Collins

Caption: Adapted from scanning electron micrograph of cytotoxic T cells (red) attacking a cancer cell (white).
Credits: Rita Elena Serda, Baylor College of Medicine; Jill George, NIH
There’s been tremendous excitement in the cancer community recently about the life-saving potential of immunotherapy. In this treatment strategy, a patient’s own immune system is enlisted to control and, in some cases, even cure the cancer. But despite many dramatic stories of response, immunotherapy doesn’t work for everyone. A major challenge has been figuring out how to identify with greater precision which patients are most likely to benefit from this new approach, and how to use that information to develop strategies to expand immunotherapy’s potential.
A couple of years ago, I wrote about early progress on this front, highlighting a small study in which NIH-funded researchers were able to predict which people with colorectal and other types of cancer would benefit from an immunotherapy drug called pembrolizumab (Keytruda®). The key seemed to be that tumors with defects affecting the “mismatch repair” pathway were more likely to benefit. Mismatch repair is involved in fixing small glitches that occur when DNA is copied during cell division. If a tumor is deficient in mismatch repair, it contains many more DNA mutations than other tumors—and, as it turns out, immunotherapy appears to be most effective against tumors with many mutations.
Now, I’m pleased to report more promising news from that clinical trial of pembrolizumab, which was expanded to include 86 adults with 12 different types of mismatch repair-deficient cancers that had been previously treated with at least one type of standard therapy [1]. After a year of biweekly infusions, more than half of the patients had their tumors shrink by at least 30 percent—and, even better, 18 had their tumors completely disappear!
Next Page