IgG
How to Feed a Macrophage
Posted on by Lawrence Tabak, D.D.S., Ph.D.
For Annalise Bond, a graduate student in the lab of Meghan Morrissey, University of California, Santa Barbara (UCSB), macrophages are “the professional eaters of our immune system.” Every minute of every day, macrophages somewhere in the body are gorging themselves to remove the cellular debris that builds up in our tissues and organs.
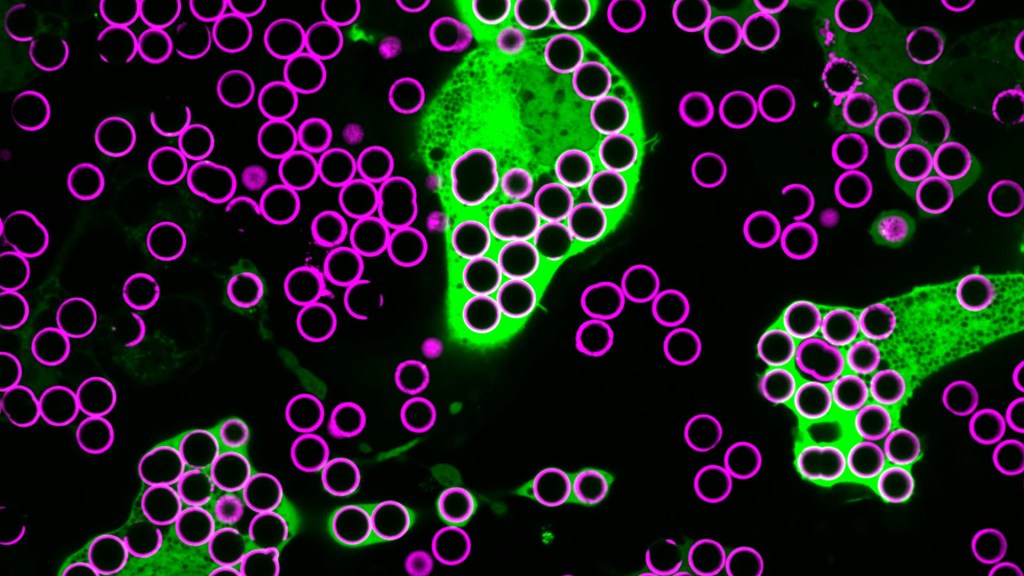
In this image, Bond caught several macrophages (green) doing what they do best: shoveling it in—in this case, during a lab experiment. The macrophages are consuming silica beads (purple) prepared with biochemicals that whet their appetites. Each bead measures about five microns in diameter. That’s roughly the size of a bacterium or a spent red blood cell—debris that a macrophage routinely consumes.
When Bond snapped this image, she noticed a pattern that reminded her of a childhood tabletop game called Hungry Hungry Hippos. Kids press a lever attached to the mouth of a plastic hippo, its lower jaw flaps open, and the challenge is to fill the mouth with as many marbles as possible . . . just like the macrophages eating beads.
Bond adjusted the colors in the photo to make them pop. She then entered it into UCSB’s 2023 Art of Science contest with the caption of Hungry Hungry Macrophages, winning high marks for drawing the association.
Though the caption was written in fun, Bond studies in earnest a fascinating biological question: How do macrophages know what to eat in the body and what to leave untouched?
In her studies, Bond coats the silica beads shown above with a lipid bilayer to mimic a cell membrane. To that coating, she adds various small molecules and proteins as “eat-me” signals often found on the surface of dying cells. Some of the signals are well characterized; but many aren’t, meaning there’s still a lot to learn about what makes a macrophage “particularly hungry” and what makes a particular target cell “extra tasty.”
Capturing fluorescent images of macrophages under the microscope, Bond counts up how many beads are eaten. Beads bearing no signal to stimulate their appetite might get eaten occasionally. But when an especially enticing signal is added, macrophages will gorge themselves until they can’t eat anymore.
In the experiment pictured above, the beads contain the antibody immunoglobulin G (IgG), which tags foreign pathogens for macrophage removal. Interestingly, IgG antibody responses also play an important role in cancer immunotherapies, in which the immune system is unleashed to fight cancer.
Among its many areas of study, the NIH-supported Morrissey lab’s wants to understand better how macrophages interact with cancer cells. They want to learn how to make cancer cells even tastier to macrophages and program their elimination from the body. Sorting out the signals will be challenging, but we know that macrophages will take a bite at the right ones. They are, after all, professional eaters.
Links:
Cancer Immunotherapy (NIH)
Annalise Bond (University of California, Santa Barbara)
Morrissey Lab (University of California, Santa Barbara)
Art of Science (University of California, Santa Barbara)
NIH Support: National Institute of General Medical Sciences
Could a Nasal Spray of Designer Antibodies Help to Beat COVID-19?
Posted on by Dr. Francis Collins

There are now several monoclonal antibodies, identical copies of a therapeutic antibody produced in large numbers, that are authorized for the treatment of COVID-19. But in the ongoing effort to beat this terrible pandemic, there’s plenty of room for continued improvements in treating infections with SARS-CoV-2, the virus that causes COVID-19.
With this in mind, I’m pleased to share progress in the development of a specially engineered therapeutic antibody that could be delivered through a nasal spray. Preclinical studies also suggest it may work even better than existing antibody treatments to fight COVID-19, especially now that new SARS-CoV-2 “variants of concern” have become increasingly prevalent.
These findings come from Zhiqiang An, The University of Texas Health Science Center at Houston, and Pei-Yong Shi, The University of Texas Medical Branch at Galveston, and their colleagues. The NIH-supported team recognized that the monoclonal antibodies currently in use all require time-consuming, intravenous infusion at high doses, which has limited their use. Furthermore, because they are delivered through the bloodstream, they aren’t able to reach directly the primary sites of viral infection in the nasal passages and lungs. With the emergence of new SARS-CoV-2 variants, there’s also growing evidence that some of those therapeutic antibodies are becoming less effective in targeting the virus.
Antibodies come in different types. Immunoglobulin G (IgG) antibodies, for example, are most prevalent in the blood and have the potential to confer sustained immunity. Immunoglobulin A (IgA) antibodies are found in tears, mucus, and other bodily secretions where they protect the body’s moist, inner linings, or mucosal surfaces, of the respiratory and gastrointestinal tracts. Immunoglobulin M (IgM) antibodies are also important for protecting mucosal surfaces and are produced first when fighting an infection.
Though IgA and IgM antibodies differ structurally, both can be administered in an inhaled mist. However, monoclonal antibodies now used to treat COVID-19 are of the IgG type, which must be IV infused.
In the new study, the researchers stitched IgG fragments known for their ability to target SARS-CoV-2 together with those rapidly responding IgM antibodies. They found that this engineered IgM antibody, which they call IgM-14, is more than 230 times better than the IgG antibody that they started with in neutralizing SARS-CoV-2.
Importantly, IgM-14 also does a good job of neutralizing SARS-CoV-2 variants of concern. These include the B.1.1.7 “U.K.” variant (now also called Alpha), the P.1 “Brazilian” variant (called Gamma), and the B.1.351 “South African” variant (called Beta). It also works against 21 other variants carrying alterations in the receptor binding domain (RBD) of the virus’ all-important spike protein. This protein, which allows SARS-CoV-2 to infect human cells, is a prime target for antibodies. Many of these alterations are expected to make the virus more resistant to monoclonal IgG antibodies that are now authorized by the FDA for emergency use.
But would it work to protect against coronavirus infection in a living animal? To find out, the researchers tried it in mice. They squirted a single dose of the IgM-14 antibody into the noses of mice either six hours before exposure to SARS-CoV-2 or six hours after infection with either the P.1 or B.1.351 variants.
In all cases, the antibody delivered in this way worked two days later to reduce dramatically the amount of SARS-CoV-2 in the lungs. That’s important because the amount of virus in the respiratory tracts of infected people is closely linked to severe illness and death due to COVID-19. If the new therapeutic antibody is proven safe and effective in people, it suggests it could become an important tool for reducing the severity of COVID-19, or perhaps even preventing infection altogether.
The researchers already have licensed this new antibody to a biotechnology partner called IGM Biosciences, Mountain View, CA, for further development and future testing in a clinical trial. If all goes well, the hope is that we’ll have a safe and effective nasal spray to serve as an extra line of defense in the fight against COVID-19.
Reference:
[1] Nasal delivery of an IgM offers broad protection from SARS-CoV-2 variants. Ku Z, Xie X, Hinton PR, Liu X, Ye X, Muruato AE, Ng DC, Biswas S, Zou J, Liu Y, Pandya D, Menachery VD, Rahman S, Cao YA, Deng H, Xiong W, Carlin KB, Liu J, Su H, Haanes EJ, Keyt BA, Zhang N, Carroll SF, Shi PY, An Z. Nature. 2021 Jun 3.
Links:
COVID-19 Research (NIH)
Zhiqiang An (The University of Texas Health Science Center at Houston)
Pei-Yong Shi (The University of Texas Medical Branch at Galveston)
IGM Biosciences (Mountain View, CA)
NIH Support: National Institute of Allergy and Infectious Diseases; National Center for Advancing Translational Sciences; National Cancer Institute
Antibody Response Affects COVID-19 Outcomes in Kids and Adults
Posted on by Dr. Francis Collins

Doctors can’t reliably predict whether an adult newly diagnosed with COVID-19 will recover quickly or battle life-threatening complications. The same is true for children.
Thankfully, the vast majority of kids with COVID-19 don’t get sick or show only mild flu-like symptoms. But a small percentage develop a delayed, but extremely troubling, syndrome called multisystem inflammatory syndrome in children (MIS-C). This can cause severe inflammation of the heart, lungs, kidneys, brain, and other parts of the body, coming on weeks after recovering from COVID-19. Fortunately, most kids respond to treatment and make rapid recoveries.
COVID-19’s sometimes different effects on kids likely stem not from the severity of the infection itself, but from differences in the immune response or its aftermath. Additional support for this notion comes from a new study, published in the journal Nature Medicine, that compared immune responses among children and adults with COVID-19 [1]. The study shows that the antibody responses in kids and adults with mild COVID-19 are quite similar. However, the complications seen in kids with MIS-C and adults with severe COVID-19 appear to be driven by two distinctly different types of antibodies involved in different aspects of the immune response.
The new findings come from pediatric pulmonologist Lael Yonker, Massachusetts General Hospital (MGH) Cystic Fibrosis Center, Boston, and immunologist Galit Alter, the Ragon Institute of MGH, Massachusetts Institute of Technology, and Harvard, Cambridge. Yonker runs a biorepository that collects samples from kids with cystic fibrosis. When the pandemic began, she started collecting plasma samples from children with mild COVID-19. Then, when Yonker and others began to see children hospitalized with MIS-C, she collected some plasma samples from them, too.
Using these plasma samples as windows into a child’s immune response, the research teams of Yonker and Alter detailed antibodies generated in 17 kids with MIS-C and 25 kids with mild COVID-19. They also profiled antibody responses of 60 adults with COVID-19, including 26 with severe disease.
Comparing antibody profiles among the four different groups, the researchers had expected children’s antibody responses to look quite different from those in adults. But they were in for a surprise. Adults and kids with mild COVID-19 showed no notable differences in their antibody profiles. The differences only came into focus when they compared antibodies in kids with MIS-C to adults with severe COVID-19.
In kids who develop MIS-C after COVID-19, they saw high levels of long-lasting immunoglobulin G (IgG) antibodies, which normally help to control an acute infection. Those high levels of IgG antibodies weren’t seen in adults or in kids with mild COVID-19. The findings suggest that in kids with MIS-C, those antibodies may activate scavenging immune cells, called macrophages, to drive inflammation and more severe illness.
In adults with severe COVID-19, the pattern differed. Instead of high levels of IgG antibodies, adults showed increased levels of another type of antibody, called immunoglobulin A (IgA). These IgA antibodies apparently were interacting with immune cells called neutrophils, which in turn led to the release of cytokines. That’s notable because the release of too many cytokines can cause what’s known as a “cytokine storm,” a severe symptom of COVID-19 that’s associated with respiratory distress syndrome, multiple organ failure, and other life-threatening complications.
To understand how a single virus can cause such different outcomes, studies like this one help to tease out their underlying immune mechanisms. While more study is needed to understand the immune response over time in both kids and adults, the hope is that these findings and others will help put us on the right path to discover better ways to help protect people of all ages from the most severe complications of COVID-19.
Reference:
[1] Humoral signatures of protective and pathological SARS-CoV-2 infection in children. Bartsch YC, Wang C, Zohar T, Fischinger S, Atyeo C, Burke JS, Kang J, Edlow AG, Fasano A, Baden LR, Nilles EJ, Woolley AE, Karlson EW, Hopke AR, Irimia D, Fischer ES, Ryan ET, Charles RC, Julg BD, Lauffenburger DA, Yonker LM, Alter G. Nat Med. 2021 Feb 12.
Links:
COVID-19 Research (NIH)
“NIH effort seeks to understand MIS-C, range of SARS-CoV-2 effects on children,” NIH news release, March 2, 2021.
Lael Yonker (Massachusetts General Hospital, Boston)
Alter Lab (Ragon Institute of Massachusetts General Hospital, MIT, and Harvard, Cambridge)
NIH Support: National Institute of Allergy and Infectious Diseases; National Cancer Institute
Two Studies Show COVID-19 Antibodies Persist for Months
Posted on by Dr. Francis Collins

More than 8 million people in the United States have now tested positive for COVID-19. For those who’ve recovered, many wonder if fending off SARS-CoV-2—the coronavirus that causes COVID-19—one time means their immune systems will protect them from reinfection. And, if so, how long will this “acquired immunity” last?
The early data brought hope that acquired immunity was possible. But some subsequent studies have suggested that immune protection might be short-lived. Though more research is needed, the results of two recent studies, published in the journal Science Immunology, support the early data and provide greater insight into the nature of the human immune response to this coronavirus [1,2].
The new findings show that people who survive a COVID-19 infection continue to produce protective antibodies against key parts of the virus for at least three to four months after developing their first symptoms. In contrast, some other antibody types decline more quickly. The findings offer hope that people infected with the virus will have some lasting antibody protection against re-infection, though for how long still remains to be determined.
In one of the two studies, partly funded by NIH, researchers led by Richelle Charles, Massachusetts General Hospital, Boston, sought a more detailed understanding of antibody responses following infection with SARS-CoV-2. To get a closer look, they enrolled 343 patients, most of whom had severe COVID-19 requiring hospitalization. They examined their antibody responses for up to 122 days after symptoms developed and compared them to antibodies in more than 1,500 blood samples collected before the pandemic began.
The researchers characterized the development of three types of antibodies in the blood samples. The first type was immunoglobulin G (IgG), which has the potential to confer sustained immunity. The second type was immunoglobulin A (IgA), which protects against infection on the body’s mucosal surfaces, such as those found in the respiratory and gastrointestinal tracts, and are found in high levels in tears, mucus, and other bodily secretions. The third type is immunoglobulin M (IgM), which the body produces first when fighting an infection.
They found that all three types were present by about 12 days after infection. IgA and IgM antibodies were short-lived against the spike protein that crowns SARS-CoV-2, vanishing within about two months.
The good news is that the longer-lasting IgG antibodies persisted in these same patients for up to four months, which is as long as the researchers were able to look. Levels of those IgG antibodies also served as an indicator for the presence of protective antibodies capable of neutralizing SARS-CoV-2 in the lab. Even better, that ability didn’t decline in the 75 days after the onset of symptoms. While longer-term study is needed, the findings lend support to evidence that protective antibody responses against the novel virus do persist.
The other study came to very similar conclusions. The team, led by Jennifer Gommerman and Anne-Claude Gingras, University of Toronto, Canada, profiled the same three types of antibody responses against the SARS-CoV-2 spike protein, They created the profiles using both blood and saliva taken from 439 people, not all of whom required hospitalization, who had developed COVID-19 symptoms from 3 to 115 days prior. The team then compared antibody profiles of the COVID-19 patients to those of people negative for COVID-19.
The researchers found that the antibodies against SARS-CoV-2 were readily detected in blood and saliva. IgG levels peaked about two weeks to one month after infection, and then remained stable for more than three months. Similar to the Boston team, the Canadian group saw IgA and IgM antibody levels drop rapidly.
The findings suggest that antibody tests can serve as an important tool for tracking the spread of SARS-CoV-2 through our communities. Unlike tests for the virus itself, antibody tests provide a means to detect infections that occurred sometime in the past, including those that may have been asymptomatic. The findings from the Canadian team further suggest that tests of IgG antibodies in saliva may be a convenient way to track a person’s acquired immunity to COVID-19.
Because IgA and IgM antibodies decline more quickly, testing for these different antibody types also could help to distinguish between an infection within the last two months and one that more likely occurred even earlier. Such details are important for filling in gaps in our understanding COVID-19 infections and tracking their spread in our communities.
Still, there are rare reports of individuals who survived one bout with COVID-19 and were infected with a different SARS-CoV-2 strain a few weeks later [3]. The infrequency of such reports, however, suggests that acquired immunity after SARS-CoV-2 infection is generally protective.
There remain many open questions, and answering them will require conducting larger studies with greater diversity of COVID-19 survivors. So, I’m pleased to note that the NIH’s National Cancer Institute (NCI) recently launched the NCI Serological Sciences Network for COVID19 (SeroNet), now the nation’s largest coordinated effort to characterize the immune response to COVID-19 [4].
The network was established using funds from an emergency Congressional appropriation of more than $300 million to develop, validate, improve, and implement antibody testing for COVID-19 and related technologies. With help from this network and ongoing research around the world, a clearer picture will emerge of acquired immunity that will help to control future outbreaks of COVID-19.
References:
[1] Persistence and decay of human antibody responses to the receptor binding domain of SARS-CoV-2 spike protein in COVID-19 patients. Iyer AS, Jones FK, Nodoushani A, Ryan ET, Harris JB, Charles RC, et al. Sci Immunol. 2020 Oct 8;5(52):eabe0367.
[2] Persistence of serum and saliva antibody responses to SARS-CoV-2 spike antigens in COVID-19 patients. Isho B, Abe KT, Zuo M, Durocher Y, McGeer AJ, Gommerman JL, Gingras AC, et al. Sci Immunol. 2020 Oct 8;5(52):eabe5511.
[3] What reinfections mean for COVID-19. Iwasaki A. Lancet Infect Dis, 2020 October 12. [Epub ahead of print]
[4] NIH to launch the Serological Sciences Network for COVID-19, announce grant and contract awardees. National Institutes of Health. 2020 October 8.
Links:
Coronavirus (COVID-19) (NIH)
Charles Lab (Massachusetts General Hospital, Boston)
Gingras Lab (University of Toronto, Canada)
Jennifer Gommerman (University of Toronto, Canada)
NCI Serological Sciences Network for COVID-19 (SeroNet) (National Cancer Institute/NIH)
NIH Support: National Institute of Allergy and Infectious Diseases; National Institute of General Medical Sciences; National Cancer Institute
Discussing the Need for Reliable Antibody Testing for COVID-19
Posted on by Dr. Francis Collins

There’s been a great deal of discussion about whether people who recover from coronavirus disease 2019 (COVID-19), have neutralizing antibodies in their bloodstream to guard against another infection. Lots of interesting data continue to emerge, including a recent preprint from researchers at Sherman Abrams Laboratory, Brooklyn, NY [1]. They tested 11,092 people for antibodies in May at a local urgent care facility and found nearly half had long-lasting IgG antibodies, a sign of exposure to the novel coronavirus SARS-CoV-2, the cause of COVID-19. The researchers also found a direct correlation between the severity of a person’s symptoms and their levels of IgG antibodies.
This study and others remind us of just how essential antibody tests will be going forward to learn more about this challenging pandemic. These assays must have high sensitivity and specificity, meaning there would be few false negatives and false positives, to tell us more about a person’s exposure to SARS-CoV-2. While there are some good tests out there, not all are equally reliable.
Recently, I had a chance to discuss COVID-19 antibody tests, also called serology tests, with Dr. Norman “Ned” Sharpless, Director of NIH’s National Cancer Institute (NCI). Among his many talents, Dr. Sharpless is an expert on antibody testing for COVID-19. You might wonder how NCI got involved in COVID-19 testing. Well, you’re going to find out. Our conversation took place while videoconferencing, with him connecting from North Carolina and me linking in from my home in Maryland. Here’s a condensed transcript of our chat:
Collins: Ned, thanks for joining me. Maybe we should start with the basics. What are antibodies anyway?
Sharpless: Antibodies are proteins that your body makes as part of the learned immune system. It’s the immunity that responds to a bacterium or a virus. In general, if you draw someone’s blood after an infection and test it for the presence of these antibodies, you can often know whether they’ve been infected. Antibodies can hang around for quite a while. How long exactly is a topic of great interest, especially in terms of the COVID-19 pandemic. But we think most people infected with coronavirus will make antibodies at a reasonably high level, or titer, in their peripheral blood within a couple of weeks of the infection.
Collins: What do antibodies tell us about exposure to a virus?
Sharpless: A lot of people with coronavirus are infected without ever knowing it. You can use these antibody assays to try and tell how many people in an area have been infected, that is, you can do a so-called seroprevalence survey.
You could also potentially use these antibody assays to predict someone’s resistance to future infection. If you cleared the infection and established immunity to it, you might be resistant to future infection. That might be very useful information. Maybe you could make a decision about how to go out in the community. So, that part is of intense interest as well, although less scientifically sound at the moment.
Collins: I have a 3D-printed model of SARS-CoV-2 on my desk. It’s sort of a spherical virus that has spike proteins on its surface. Do the antibodies interact with the virus in some specific ways?
Sharpless: Yes, antibodies are shaped like the letter Y. They have two binding domains at the head of each Y that will recognize something about the virus. We find antibodies in the peripheral blood that recognize either the virus nucleocapsid, which is the structural protein on the inside; or the spikes, which stick out and give coronavirus its name. We know now that about 99 percent of people who get infected with the virus will develop antibodies eventually. Most of those antibodies that you can detect to the spike proteins will be neutralizing, which means they can kill the virus in a laboratory experiment. We know from other viruses that, generally, having neutralizing antibodies is a promising sign if you want to be immune to that virus in the future.
Collins: Are COVID-19 antibodies protective? Are there reports of people who’ve gotten better, but then were re-exposed and got sick again?
Sharpless: It’s controversial. People can shed the virus’s nucleic acid [genetic material], for weeks or even more than a month after they get better. So, if they have another nucleic acid test it could be positive, even though they feel better. Often, those people aren’t making a lot of live virus, so it may be that they never stopped shedding the virus. Or it may be that they got re-infected. It’s hard to understand what that means exactly. If you think about how many people worldwide have had COVID-19, the number of legitimate possible reinfection cases is in the order of a handful. So, it’s a pretty rare event, if it happens at all.
Collins: For somebody who does have the antibodies, who apparently was previously infected, do they need to stop worrying about getting exposed? Can they can do whatever they want and stop worrying about distancing and wearing masks?
Sharpless: No, not yet. To use antibodies to predict who’s likely to be immune, you’ve got to know two things.
First: can the tests actually measure antibodies reliably? I think there are assays available to the public that are sufficiently good for asking this question, with an important caveat. If you’re trying to detect something that’s really rare in a population, then any test is going to have limitations. But if you’re trying to detect something that’s more common, as the virus was during the recent outbreak in Manhattan, I think the tests are up to the task.
Second: does the appearance of an antibody in the peripheral blood mean that you’re actually immune or you’re just less likely to get the virus? We don’t know the answer to that yet.
Collins: Let’s be optimistic, because it sounds like there’s some evidence to support the idea that people who develop these antibodies are protected against infection. It also sounds like the tests, at least some of them, are pretty good. But if there is protection, how long would you expect it to last? Is this one of those things where you’re all set for life? Or is this going to be something where somebody’s had it and might get it again two or three years from now, because the immunity faded away?
Sharpless: Since we have no direct experience with this virus over time, it’s hard to answer. The potential for this cell-based humoral immunity to last for a while is there. For some viruses, you have a long-lasting antibody protection after infection; for other viruses, not so much.
So that’s the unknown thing. Is immunity going to last for a while? Of course, if one were to bring up the topic of vaccines, that’s very important to know, because you would want to know how often one would have to give that vaccine, even under optimal circumstances.
Collins: Yes, our conversation about immunity is really relevant to the vaccines we’re trying to develop right now. Will these vaccines be protective for long periods of time? We sure hope so, but we’ve got to look carefully at the issue. Let’s come back, though, to the actual performance of the tests. The NCI has been right in the middle of trying to do this kind of validation. How did that happen, and how did that experience go?
Sharpless: Yes, I think one might ask: why is the National Cancer Institute testing antibody kits for the FDA? It is unusual, but certainly not unheard of, for NCI to take up problems like this during a time of a national emergency. During the HIV era, NCI scientists, along with others, identified the virus and did one of the first successful compound screens to find the drug AZT, one of the first effective anti-HIV therapies.
NCI’s Frederick National Lab also has a really good serology lab that had been predominantly working on human papillomavirus (HPV). When the need arose for serologic testing a few months ago, we pivoted that lab to a coronavirus serology lab. It took us a little while, but eventually we rounded up everything you needed to create positive and negative reference panels for antibody testing.
At that time, the FDA had about 200 manufacturers making serology tests that hoped for approval to sell. The FDA wanted some performance testing of those assays by a dispassionate third party. The Frederick National Lab seemed like the ideal place, and the manufacturers started sending us kits. I think we’ve probably tested on the order of 20 so far. We give those data back to the FDA for regulatory decision making. They’re putting all the data online.
Collins: How did it look? Are these all good tests or were there some clunkers?
Sharpless: There were some clunkers. But we were pleased to see that some of the tests appear to be really good, both in our hands and those of other groups, and have been used in thousands of patients.
There are a few tests that have sensitivities that are pretty high and specificities well over 99 percent. The Roche assay has a 99.8 percent specificity claimed on thousands of patients, and for the Mt. Sinai assay developed and tested by our academic collaborators in a panel of maybe 4,000 patients, they’re not sure they’ve ever had a false positive. So, there are some assays out there that are good.
Collins: There’s been talk about how there will soon be monoclonal antibodies directed against SARS-CoV-2. How are those derived?
Sharpless: They’re picked, generally, for appearing to have neutralizing activity. When a person makes antibodies, they don’t make one antibody to a pathogen. They make a whole family of them. And those can be individually isolated, so you can know which antibodies made by a convalescent individual really have virus-neutralizing capacity. That portion of the antibody that recognizes the virus can be engineered into a manufacturing platform to make monoclonal antibodies. Monoclonal means one kind of antibody. That approach has worked for other infectious diseases and is an interesting idea here too.
Collins: I can say a bit about that, because we are engaged in a partnership with industry and FDA called Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV). One of the hottest ideas right now is monoclonal antibodies, and we’re in the process of devising a master protocol, one for outpatients and one for inpatients.
Janet Woodcock of Operation Warp Speed tells me 21 companies are developing monoclonal antibodies. While doing these trials, we’d love to do comparisons, which is why it’s good to have an organization like ACTIV to bring everybody together, making sure you’re using the same endpoints and the same laboratory measures. I think that, maybe even by late summer, we might have some results. For people who are looking at what’s the next most-hopeful therapeutic option for people who are really sick with COVID-19, so far we have remdesivir. It helps, but it’s not a home run. Maybe monoclonal antibodies will be the next thing that really gives a big boost in survival. That would be the hope.
Ned, let me ask you one final question about herd, or group, immunity. One hears a bit about that in terms of how we are all going to get past this COVID-19 pandemic. What’s that all about?
Sharpless: Herd immunity is when a significant portion of the population is immune to a pathogen, then that pathogen will die out in the population. There just aren’t enough susceptible people left to infect. What the threshold is for herd immunity depends on how infectious the virus is. For a highly infectious virus, like measles, maybe up to 90 percent of the population must be immune to get herd immunity. Whereas for other less-infectious viruses, it may only be 50 percent of the population that needs to be immune to get herd immunity. It’s a theoretical thing that makes some assumptions, such as that everybody’s health status is the same and the population mixes perfectly every day. Neither of those are true.
How well that actual predictive number will work for coronavirus is unknown. The other thing that’s interesting is a lot of that work has been based on vaccines, such as what percentage do you have to vaccinate to get herd immunity? But if you get to herd immunity by having people get infected, so-called natural herd immunity, that may be different. You would imagine the most susceptible people get infected soonest, and so the heterogeneity of the population might change the threshold calculation.
The short answer is nobody wants to find out. No one wants to get to herd immunity for COVID-19 through natural herd immunity. The way you’d like to get there is with a vaccine that you then could apply to a large portion of the population, and have them acquire immunity in a more safe and controlled manner. Should we have an efficacious vaccine, this question will loom large: how many people do we need to vaccinate to really try and protect vulnerable populations?
Collins: That’s going to be a really critical question for the coming months, as the first large-scale vaccine trials get underway in July, and we start to see how they work and how successful and safe they are. But I’m also worried seeing some reports that 1 out of 5 Americans say they wouldn’t take a vaccine. It would be truly a tragedy if we have a safe and effective vaccine, but we don’t get enough uptake to achieve herd immunity. So, we’ve got some work to do on all fronts, that’s for sure.
Ned, I want to thank you for sharing all this information about antibodies and serologies and other things, as well as thank you for your hard work with all your amazing NCI colleagues.
Sharpless: Thanks for having me.
Reference:
[1] SARS-CoV-2 IgG Antibody Responses in New York City. Reifer J, Hayum N, Heszkel B, Klagsbald I, Streva VA. medRxiv. Preprint posted May 26, 2020.
Links:
Coronavirus (COVID-19) (NIH)
At NCI, A Robust and Rapid Response to the COVID-19 Pandemic. Norman E. Sharpless. Cancer Currents Blog. April 17, 2020 (National Cancer Institute/NIH)
Serological Testing for SARS-CoV-2 Antibodies (American Medical Association, Chicago)
COVID-19 Antibody Testing Primer (Infectious Diseases Society of America, Arlington, VA)
Accelerating COVID-19 Therapeutic Interventions and Vaccines (NIH)
Study Finds Nearly Everyone Who Recovers From COVID-19 Makes Coronavirus Antibodies
Posted on by Dr. Francis Collins

There’s been a lot of excitement about the potential of antibody-based blood tests, also known as serology tests, to help contain the coronavirus disease 2019 (COVID-19) pandemic. There’s also an awareness that more research is needed to determine when—or even if—people infected with SARS-CoV-2, the novel coronavirus that causes COVID-19, produce antibodies that may protect them from re-infection.
A recent study in Nature Medicine brings much-needed clarity, along with renewed enthusiasm, to efforts to develop and implement widescale antibody testing for SARS-CoV-2 [1]. Antibodies are blood proteins produced by the immune system to fight foreign invaders like viruses, and may help to ward off future attacks by those same invaders.
In their study of blood drawn from 285 people hospitalized with severe COVID-19, researchers in China, led by Ai-Long Huang, Chongqing Medical University, found that all had developed SARS-CoV-2 specific antibodies within two to three weeks of their first symptoms. Although more follow-up work is needed to determine just how protective these antibodies are and for how long, these findings suggest that the immune systems of people who survive COVID-19 have been be primed to recognize SARS-CoV-2 and possibly thwart a second infection.
Specifically, the researchers determined that nearly all of the 285 patients studied produced a type of antibody called IgM, which is the first antibody that the body makes when fighting an infection. Though only about 40 percent produced IgM in the first week after onset of COVID-19, that number increased steadily to almost 95 percent two weeks later. All of these patients also produced a type of antibody called IgG. While IgG often appears a little later after acute infection, it has the potential to confer sustained immunity.
To confirm their results, the researchers turned to another group of 69 people diagnosed with COVID-19. The researchers collected blood samples from each person upon admission to the hospital and every three days thereafter until discharge. The team found that, with the exception of one woman and her daughter, the patients produced specific antibodies against SARS-CoV-2 within 20 days of their first symptoms of COVID-19.
Meanwhile, innovative efforts are being made on the federal level to advance COVID-19 testing. The NIH just launched the Rapid Acceleration of Diagnostics (RADx) Initiative to support a variety of research activities aimed at improving detection of the virus. As I recently highlighted on this blog, one key component of RADx is a “shark tank”-like competition to encourage science and engineering’s most inventive minds to develop rapid, easy-to-use technologies to test for the presence of SARS-CoV-2.
On the serology testing side, the NIH’s National Cancer Institute has been checking out kits that are designed to detect antibodies to SARS-CoV-2 and have found mixed results. In response, the Food and Drug Administration just issued its updated policy on antibody tests for COVID-19. This guidance sets forth precise standards for laboratories and commercial manufacturers that will help to speed the availability of high-quality antibody tests, which in turn will expand the capacity for rapid and widespread testing in the United States.
Finally, it’s important to keep in mind that there are two different types of SARS-CoV-2 tests. Those that test for the presence of viral nucleic acid or protein are used to identify people who are acutely infected and should be immediately quarantined. Tests for IgM and/or IgG antibodies to the virus, if well-validated, indicate a person has previously been infected with COVID-19 and is now potentially immune. Two very different types of tests—two very different meanings.
There’s still a way to go with both virus and antibody testing for COVID-19. But as this study and others begin to piece together the complex puzzle of antibody-mediated immunity, it will be possible to learn more about the human body’s response to SARS-CoV-2 and home in on our goal of achieving safe, effective, and sustained protection against this devastating disease.
Reference:
[1] Antibody responses to SARS-CoV-2 in patients with COVID-19. Long QX, Huang AI, et al. Nat Med. 2020 Apr 29. [Epub ahead of print]
Links:
Coronaviruses (NIH)
“NIH Begins Study to Quantify Undetected Cases of Coronavirus Infection,” NIH News Release, April 10, 2020.
“NIH mobilizes national innovation initiative for COVID-19 diagnostics,” NIH News Release, April 29, 2020.
Policy for Coronavirus Disease-2019 Tests During the Public Health Emergency (Revised), May 2020 (Food and Drug Administration)