hypertension
Bringing Needed Structure to COVID-19 Drug Development
Posted on by Dr. Francis Collins
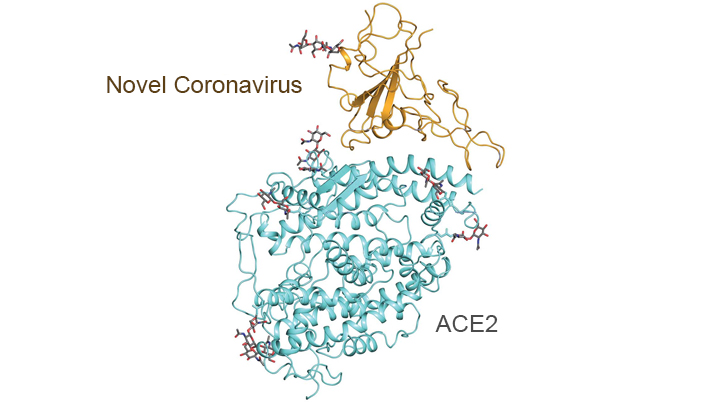
With so much information swirling around these days about the coronavirus disease 2019 (COVID-19) pandemic, it would be easy to miss one of the most interesting and significant basic science reports of the past few weeks. It’s a paper published in the journal Science [1] that presents an atomic-scale snapshot showing the 3D structure of the spike protein on the novel coronavirus attached to a human cell surface protein called ACE2, or angiotensin converting enzyme 2. ACE2 is the receptor that the virus uses to gain entry.
What makes this image such a big deal is that it shows—in exquisite detail—how the coronavirus attaches to human cells before infecting them and making people sick. The structural map of this interaction will help guide drug developers, atom by atom, in devising safe and effective ways to treat COVID-19.
This new work, conducted by a team led by Qiang Zhou, Westlake Institute for Advanced Study, Hangzhou, China, took advantage of a high-resolution imaging tool called cryo-electron microscopy (cryo-EM). This approach involves flash-freezing molecules in liquid nitrogen and bombarding them with electrons to capture their images with a special camera. When all goes well, cryo-EM can solve the structure of intricate macromolecular complexes in a matter of days, including this one showing the interaction between a viral protein and human protein.
Zhou’s team began by mapping the structure of human ACE2 in a complex with B0AT1, which is a membrane protein that it helps to fold. In the context of this complex, ACE2 is a dimer—a scientific term for a compound composed of two very similar units. Additional mapping revealed how the surface protein of the novel coronavirus interacts with ACE2, indicating how the virus’s two trimeric (3-unit) spike proteins might bind to an ACE2 dimer. After confirmation by further research, these maps may well provide a basis for the design and development of therapeutics that specifically target this critical interaction.
The ACE2 protein resides on the surface of cells in many parts of the human body, including the heart and lungs. The protein is known to play a prominent role in the body’s complex system of regulating blood pressure. In fact, a class of drugs that inhibit ACE and related proteins are frequently prescribed to help control high blood pressure, or hypertension. These ACE inhibitors lower blood pressure by causing blood vessels to relax.
Since the COVID-19 outbreak, many people have wondered whether taking ACE inhibitors would be helpful or detrimental against coronavirus infection. This is of particular concern to doctors whose patients are already taking the medications to control hypertension. Indeed, data from China and elsewhere indicate hypertension is one of several coexisting conditions that have consistently been reported to be more common among people with COVID-19 who develop life-threatening severe acute respiratory syndrome.
In a new report in this week’s New England Journal of Medicine, a team of U.K. and U.S. researchers, partly supported by NIH, examined the use of ACE inhibitors and other angiotensin-receptor blockers (ARBs) in people with COVID-19. The team, led by Scott D. Solomon of Brigham and Women’s Hospital and Harvard Medical School, Boston, found that current evidence in humans is insufficient to support or refute claims that ACE inhibitors or ARBs may be helpful or harmful to individuals with COVID-19.
The researchers concluded that these anti-hypertensive drugs should be continued in people who have or at-risk for COVID-19, stating: “Although additional data may further inform the treatment of high-risk patients … clinicians need to be cognizant of the unintended consequences of prematurely discontinuing proven therapies in response to hypothetical concerns.” [2]
Research is underway to generate needed data on the use of ACE inhibitors and similar drugs in the context of the COVID-19 pandemic, as well as to understand more about the basic mechanisms underlying this rapidly spreading viral disease. This kind of fundamental research isn’t necessarily the stuff that will make headlines, but it likely will prove vital to guiding the design of effective drugs that can help bring this serious global health crisis under control.
References:
[1] Structural basis for the recognition of the SARS-CoV-2 by full-length human ACE2. Yan R, Zhang Y, Li Y, Xia L, Guo Y, Zhou Q. Science. 27 March 2020. [Epub ahead of publication]
[2] Renin–Angiotensin–Aldosterone System Inhibitors in Patients with Covid-19. Vaduganathan M, Vardeny O, Michel T, McMurray J, Pfeffer MA, Solomon SD. 30 NEJM. March 2020 [Epub ahead of Publication]
Links:
Coronavirus (COVID-19) (NIH)
COVID-19, MERS & SARS (National Institute of Allergy and Infectious Diseases/NIH)
Transformative High Resolution Cryo-Electron Microscopy (Common Fund/NIH)
Qiang Zhou (Westlake Institute for Advanced Study, Zhejiang Province)
Scott D. Solomon (Brigham and Women’s Hospital, Boston)
NIH Support: National Center for Advancing Translational Sciences; National Heart, Lung, and Blood Institute
Wearable Ultrasound Patch Monitors Blood Pressure
Posted on by Dr. Francis Collins
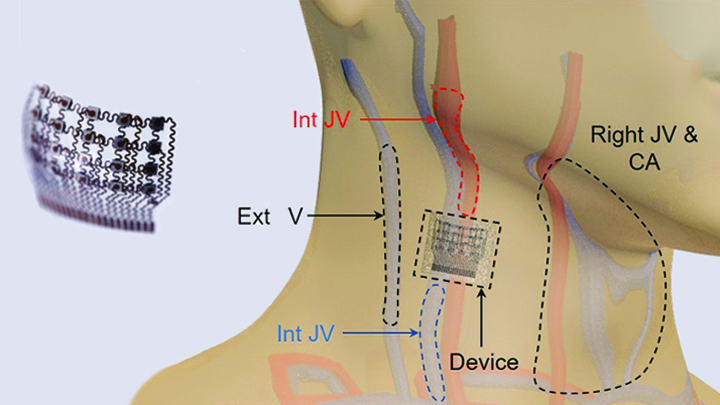
Caption: Worn on the neck, the device records central blood pressure in the carotid artery (CA), internal jugular vein (Int JV) and external jugular vein (Ext JV).
Credit: Adapted from Wang et al, Nature Biomedical Engineering
There’s lots of excitement out there about wearable devices quietly keeping tabs on our health—morning, noon, and night. Most wearables monitor biological signals detectable right at the surface of the skin. But, the sensing capabilities of the “skin” patch featured here go far deeper than that.
As described recently in Nature Biomedical Engineering, when this small patch is worn on the neck, it measures blood pressure way down in the central arteries and veins more than an inch beneath the skin [1]. The patch works by emitting continuous ultrasound waves that monitor subtle, real-time changes in the shape and size of pulsing blood vessels, which indicate rises or drops in pressure.
Can Barbers Help Black Men Lower Their Blood Pressure?
Posted on by Dr. Francis Collins

Caption: Barber Eric Muhammad (left) in his barbershop taking the blood pressure of patron.
Credit: Smidt Heart Institute, Cedars-Sinai Medical Center
You expect to have your blood pressure checked and treated when you visit the doctor’s office or urgent care clinic. But what about the barbershop? New research shows that besides delivering the customary shave and a haircut, barbers might be able to play a significant role in helping control high blood pressure.
High blood pressure, or hypertension, is a particularly serious health problem among non-Hispanic black men. So, in a study involving 52 black-owned barbershops in the Los Angeles area, barbers encouraged their regular, black male patrons, ages 35 to 79, to get their blood pressure checked at their shops [1]. Nearly 320 men turned out to have uncontrolled hypertension and enrolled in the study. In a randomized manner, barbers then encouraged these men to do one of two things: attend one-on-one barbershop meetings with pharmacists who could prescribe blood pressure medicines, or set up appointments with their own doctors and consider making lifestyle changes.
The result? More than 63 percent of the men who received medications prescribed by specially-trained pharmacists lowered their blood pressure to healthy levels within 6 months, compared to less than 12 percent of those who went to see their doctors. The findings serve as a reminder that helping people get healthier doesn’t always require technological advances. Sometimes it may just involve developing more effective ways of getting proven therapy to at-risk communities.
Creative Minds: Exploring the Role of Immunity in Hypertension
Posted on by Dr. Francis Collins

Meena Madhur / Credit: John Russell
If Meena Madhur is correct, people with hypertension will one day pay as much attention to their immune cell profiles as their blood pressure readings. A physician-researcher at Vanderbilt University School of Medicine, Nashville, Madhur is one of a growing number of scientists who thinks the immune system contributes to—or perhaps even triggers—hypertension, which increases the risk of stroke, heart disease, kidney disease, and other serious health problems.
About one of every three adult Americans currently have hypertension, yet a surprising number don’t know they have it and less than half have their high blood pressure under control—leading many health experts to refer to the condition as a “silent killer”[1,2]. For many folks, blood pressure control can be achieved through lifestyle changes, such as losing weight, exercising, limiting salt intake, and taking blood pressure medicines prescribed by their health-care provider. Unfortunately, such measures don’t work for everyone, and some people continue to suffer damage to their kidneys and blood vessels from poorly controlled hypertension.
Madhur wants to know whether the immune system might be playing a role, and whether this might hold some clues for developing new, more targeted ways of treating high blood pressure. To get such answers, this practicing cardiologist will use her 2016 NIH Director’s New Innovator Award to conduct sophisticated, single-cell analyses of the immune systems of people with and without hypertension. Her goal is to produce the most comprehensive catalog to date of which human immune cells might be involved in hypertension.
Cardiometabolic Disease: Big Data Tackles a Big Health Problem
Posted on by Dr. Francis Collins
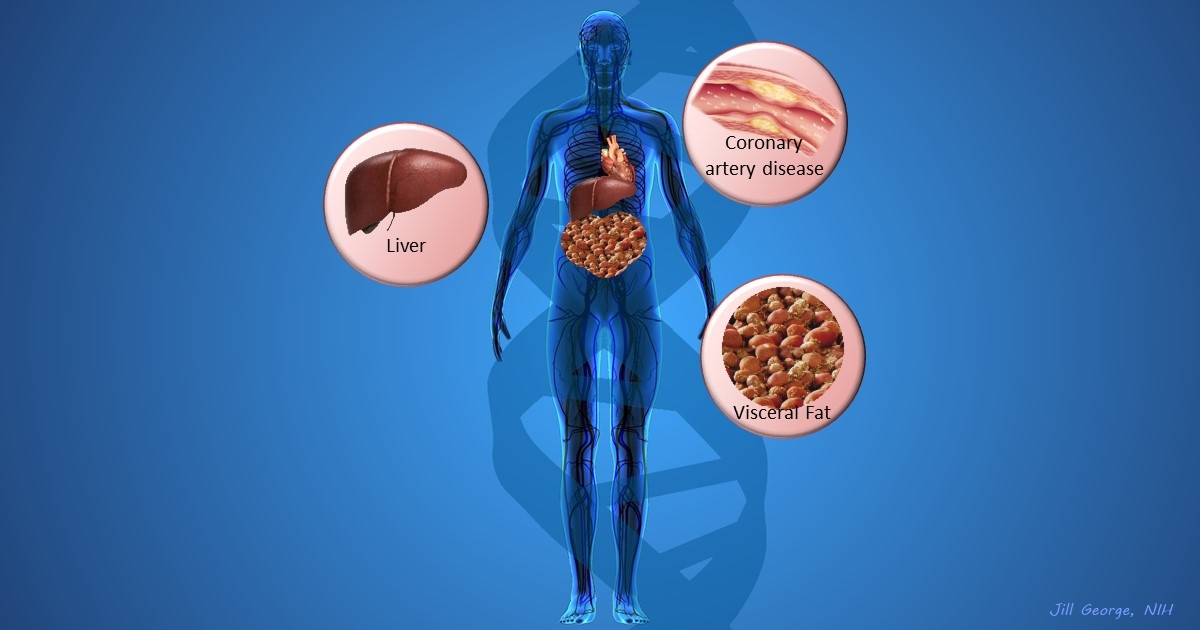
More and more studies are popping up that demonstrate the power of Big Data analyses to get at the underlying molecular pathology of some of our most common diseases. A great example, which may have flown a bit under the radar during the summer holidays, involves cardiometabolic disease. It’s an umbrella term for common vascular and metabolic conditions, including hypertension, impaired glucose and lipid metabolism, excess belly fat, and inflammation. All of these components of cardiometabolic disease can increase a person’s risk for a heart attack or stroke.
In the study, an international research team tapped into the power of genomic data to develop clearer pictures of the complex biocircuitry in seven types of vascular and metabolic tissue known to be affected by cardiometabolic disease: the liver, the heart’s aortic root, visceral abdominal fat, subcutaneous fat, internal mammary artery, skeletal muscle, and blood. The researchers found that while some circuits might regulate the level of gene expression in just one tissue, that’s often not the case. In fact, the researchers’ computational models show that such genetic circuitry can be organized into super networks that work together to influence how multiple tissues carry out fundamental life processes, such as metabolizing glucose or regulating lipid levels. When these networks are perturbed, perhaps by things like inherited variants that affect gene expression, or environmental influences such as a high-carb diet, sedentary lifestyle, the aging process, or infectious disease, the researchers’ modeling work suggests that multiple tissues can be affected, resulting in chronic, systemic disorders including cardiometabolic disease.
Pursuing Precision Medicine for Chronic Kidney Disease
Posted on by Dr. Francis Collins
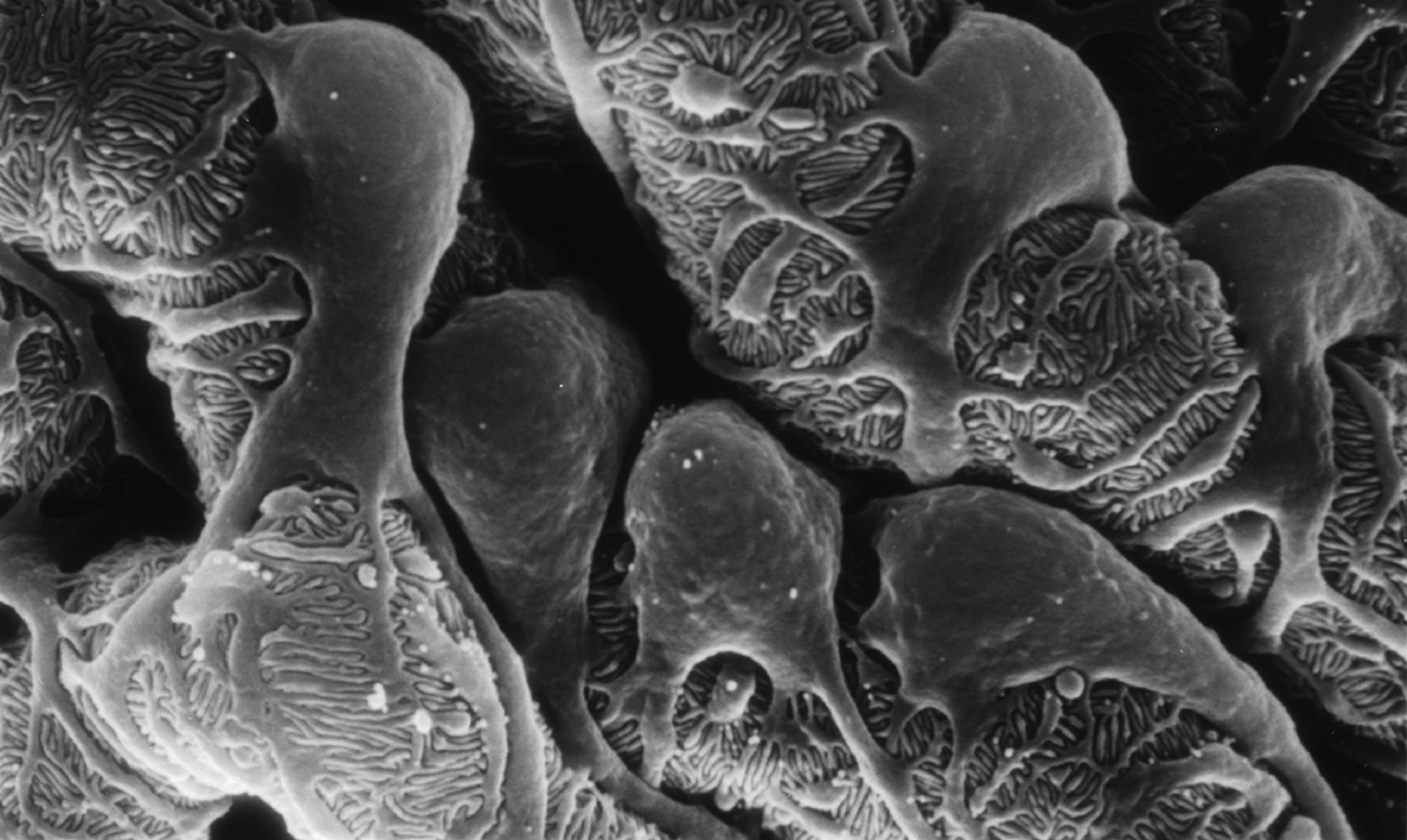
Caption: Scanning electron micrograph showing a part of one of the kidney’s glomerular filters, which are damaged in people with chronic kidney disease (CKD). The cells with the lacy cytoplasmic extensions are called podocytes.
Credit: Kretzler Lab, University of Michigan Health System, Ann Arbor
Every day, our kidneys filter more than 30 gallons of blood to allow excretion of molecules that can harm us if they build up as waste. But, for more than 20 million Americans and a growing number of people around the world, this important function is compromised by chronic kidney disease (CKD) [1]. Some CKD patients are at high risk of progressing to actual kidney failure, treatable only by dialysis or kidney transplants, while others remain generally healthy with stable kidney function for many years with minimal treatment.
The dilemma is that, even when CKD is diagnosed early, there’s been no good way to predict which individuals are at high risk for rapid progression. Those individuals would potentially benefit from more intensive measures to slow or prevent kidney failure, such as drug regimens that tightly control blood pressure and/or blood glucose. So, I’m pleased to report that NIH-funded researchers have made some progress toward developing more precise strategies for identifying individuals at high risk for kidney failure. In recent findings published in Science Translational Medicine [2], an international research team has identified a protein, easily detectable in urine, which appears to serve as an early warning sign of CKD progression.
A wide range of conditions, from diabetes to hypertension to the autoimmune disease lupus, can contribute to the gradual loss of kidney function seen in people with CKD. But research suggests that once kidney damage reaches a critical threshold, it veers off to follow a common downhill course, driven by shared cell signaling pathways and almost independent of the conditions causing it. If there was an easy, reliable way to determine when a CKD patient’s kidneys are approaching this threshold, it could open the door to better strategies for protecting them from kidney failure.
With this need in mind, a team, led by Matthias Kretzler and Wenjun Ju of the University of Michigan, began analyzing gene activity in kidney biopsy samples donated by 164 CKD patients and stored in the European Renal cDNA Bank. Specifically, the researchers looked for patterns of gene activity that corresponded with the patients’ estimated glomerular filtration rates, an indicator of renal function frequently calculated as part of a routine blood workup. Their first pass produced a list of 72 genes that displayed varying levels of activity that corresponded to differences in the patients’ estimated glomerular filtration rates. Importantly, the activity of many of those genes is also increased in cell signaling pathways thought to drive CKD progression.
Further study in two more groups of CKD patients, one from the United States and another from Europe, whittled the list down to three genes that best predicted kidney function. The researchers then zeroed in on the gene that codes for epidermal growth factor (EGF), a protein that, within the kidney, seems to be produced specifically in tubules, which are key components of the waste filtration system. Because EGF appears to enhance tubular repair after injury, researchers had a hunch that it might serve as a positive biomarker of tubular function that could be combined with existing tests of glomerular filtration to detect progression of CKD at an earlier stage.
In groups of CKD patients from the United States and China, the researchers went on to find that the amount of EGF in the urine provides an accurate measure of the protein’s activity in the kidney, making it a promising candidate for a simple urine test. In fact, CKD patients with low levels of EGF in their urine were four times more likely than those with higher EGF levels to have their kidney function worsen within a few years.
These lines of evidence suggest that, if these findings are replicated in additional studies, it may be possible to develop a simple EGF urine test to help identify which individuals with CKD would benefit the most from aggressive disease management and clinical follow-up. Researchers also plan to explore the possibility that such a urine test might prove useful in the early diagnosis of CKD, before there are any other indications of kidney disease. These are very promising new findings, but much remains to be done before we can think of applying these results as standard of care in the clinic. For example, the EGF work needs to be replicated in larger groups of CKD patients, as well as CKD patients with diabetes.
Beyond their implications for CKD, these results demonstrate the power of identifying new biologically important indicators directly from patients and then testing them in large, diverse cohorts of people. I look forward to the day when these sorts of studies will become possible on an even larger scale through our U.S. Precision Medicine Initiative Cohort.
References:
[1] National Chronic Kidney Disease Fact Sheet, 2014. Centers for Disease Control and Prevention.
[2] Tissue transcriptome-driven identification of epidermal growth factor as a chronic kidney disease biomarker. Ju W, Nair V, Smith S, Zhu L, Shedden K, Song PX, Mariani LH, Eichinger FH, Berthier CC, Randolph A, Lai JY, Zhou Y, Hawkins JJ, Bitzer M, Sampson MG, Thier M, Solier C, Duran-Pacheco GC, Duchateau-Nguyen G, Essioux L, Schott B, Formentini I, Magnone MC, Bobadilla M, Cohen CD, Bagnasco SM, Barisoni L, Lv J, Zhang H, Wang HY, Brosius FC, Gadegbeku CA, Kretzler M; ERCB, C-PROBE, NEPTUNE, and PKU-IgAN Consortium. Sci Transl Med. 2015 Dec 2;7(316):316ra193.
Links:
Chronic Kidney Disease: What Does it Mean to Me? (National Institute of Diabetes and Digestive and Kidney Diseases/NIH)
Personalized Molecular Nephrology Research Laboratory (University of Michigan)
C-Probe (University of Michigan)
Precision Medicine Initiative Cohort Program (NIH)
NIH Support: National Center for Advancing Translational Sciences; National Institute of Diabetes and Digestive and Kidney Diseases
Global Health: Time to Pay Attention to Chronic Diseases
Posted on by Dr. Francis Collins

Caption: Projected deaths (in millions) by cause in low-income countries. Note increase in non-communicable diseases (orange).
Credit: Adapted from Beaglehole R, Bonita R. Lancet. 2008 Dec 6;372(9654):1988-96.
Greetings from China. I’m here in Shanghai with other biomedical research leaders for two major meetings. The first one, which is the topic of my blog today, is on global health. So, you might expect there to be a lot of talk about malaria, influenza, MERS-CoV, Ebola virus, sleeping sickness, dengue fever, tuberculosis, HIV/AIDS, and other infectious diseases. And those are most certainly topics of intense interest to NIH and our colleagues around the world. But this particular meeting is about a different kind of global health threat that’s becoming a rapidly growing problem: chronic diseases.
While infectious diseases remain a significant problem in the developing world, cancer, heart disease, obesity, diabetes, and other non-communicable diseases are now among the fastest growing causes of death and disability around the globe. In fact, nearly three-quarters of the 38 million people who died of chronic diseases in 2012 lived in low- or middle-income countries [1].
High Blood Pressure, a Global Health Threat
Posted on by Dr. Francis Collins

Caption: Blood pressure is highest in low-income countries
Source: World Health Organization
{kind=link}
On Sunday April 7th, we mark the 65th anniversary of the World Health Organization (WHO). Each year, WHO uses the occasion to highlight a particular health issue; this year, they chose high blood pressure—hypertension. It’s a timely choice. Worldwide, at least one in three adults suffers from high blood pressure. That amounts to 68 million adults in the U.S. alone.
Your blood pressure naturally rises and falls a bit during the day, but permanent high blood pressure is a dangerous condition that increases your chance of heart disease, heart attacks, strokes, kidney failure, and even blindness.