basic research
Study Suggests Treatments that Unleash Immune Cells in the Brain Could Help Combat Alzheimer’s
Posted on by Dr. Monica M. Bertagnolli
In Alzheimer’s disease, a buildup of sticky amyloid proteins in the brain clump together to form plaques, causing damage that gradually leads to worsening dementia symptoms. A promising way to change the course of this disease is with treatments that clear away damaging amyloid plaques or stop them from forming in the first place. In fact, the Food and Drug Administration recently approved the first drug for early Alzheimer’s that moderately slows cognitive decline by reducing amyloid plaques.1 Still, more progress is needed to combat this devastating disease that as many as 6.7 million Americans were living with in 2023.
Recent findings from a study in mice, supported in part by NIH and reported in Science Translational Medicine, offer another potential way to clear amyloid plaques in the brain. The key component of this strategy is using the brain’s built-in cleanup crew for amyloid plaques and other waste products: immune cells known as microglia that naturally help to limit the progression of Alzheimer’s. The findings suggest it may be possible to develop immunotherapies—treatments that use the body’s immune system to fight disease—to activate microglia in the brains of people with Alzheimer’s and clear amyloid plaques more effectively.2
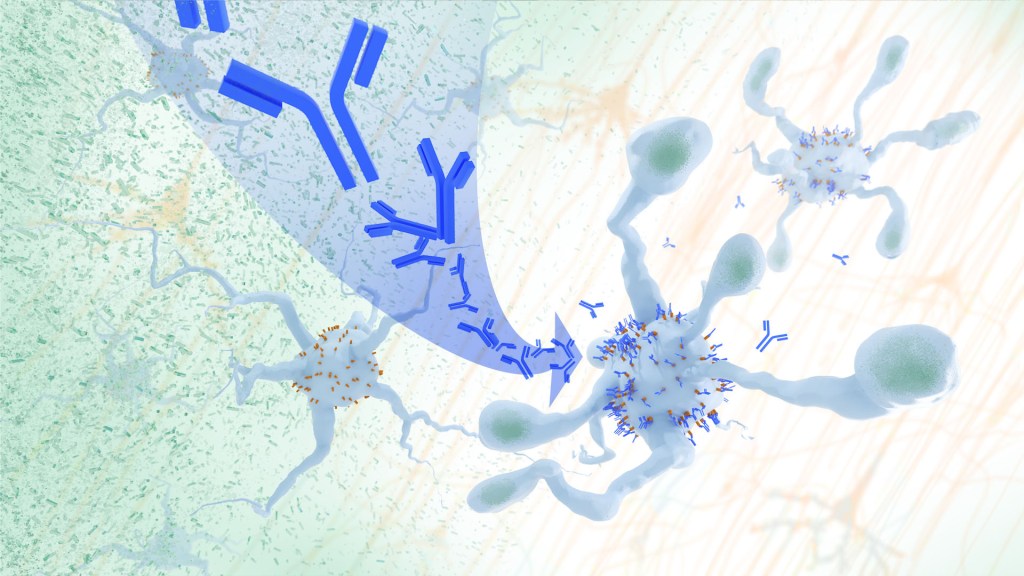
In their report, the research team—including Marco Colonna, Washington University School of Medicine in St. Louis, and Jinchao Hou, now at Children’s Hospital of Zhejiang University School of Medicine in Zhejiang Province, China—wrote that microglia in the brain surround plaques to create a barrier that controls their spread. Microglia can also destroy amyloid plaques directly. But how microglia work in the brain depends on a fine-tuned balance of signals that activate or inhibit them. In people with Alzheimer’s, microglia don’t do their job well enough.
The researchers suspected this might have something to do with a protein called apolipoprotein E (APOE). This protein normally helps carry cholesterol and other fats in the bloodstream. But the gene encoding the protein is known for its role in influencing a person’s risk for developing Alzheimer’s, and in the Alzheimer’s brain, the protein is a key component of amyloid plaques. The protein can also inactivate microglia by binding to a receptor called LILRB4 found on the immune cells’ surfaces.
Earlier studies in mouse models of Alzheimer’s showed that the LILRB4 receptor is expressed at high levels in microglia when amyloid plaques build up. This suggested that treatments targeting this receptor on microglia might hold promise for treating Alzheimer’s. In the new study, the research team looked for evidence that an increase in LILRB4 receptors on microglia plays an important role in the brains of people with Alzheimer’s.
To do this, the researchers first studied brain tissue samples from people who died with this disease and discovered unusually high amounts of the LILRB4 receptor on the surfaces of microglia, similar to what had been seen in the mouse models. This could help explain why microglia struggle to control amyloid plaques in the Alzheimer’s brain.
Next, the researchers conducted studies of mouse brains with accumulating amyloid plaques that express the LILRB4 receptor to see if an antibody targeting the receptor could lower amyloid levels by boosting activity of immune microglia. Their findings suggest that the antibody treatment blocked the interaction between APOE proteins and LILRB4 receptors and enabled microglia to clear amyloid plaques. Intriguingly, the team’s additional studies found that this clearing process also changed the animals’ behavior, making them less likely to take risks. That’s important because people with Alzheimer’s may engage in risky behaviors as they lack memories of earlier experiences that they could use to make decisions.
There’s plenty more to learn. For instance, the researchers don’t know yet whether this approach will affect the tau protein, which forms damaging tangles inside neurons in the Alzheimer’s brain. They also want to investigate whether this strategy of clearing amyloid plaques might come with other health risks.
But overall, these findings add to evidence that immunotherapies of this kind could be a promising way to treat Alzheimer’s. This strategy may also have implications for treating other neurodegenerative conditions characterized by toxic debris in the brain, such as Parkinson’s disease, amyotrophic lateral sclerosis (ALS), and Huntington’s disease. The hope is that this kind of research will ultimately lead to more effective treatments for Alzheimer’s and other conditions affecting the brain.
References:
[1] FDA Converts Novel Alzheimer’s Disease Treatment to Traditional Approval. U.S. Food and Drug Administration (2023).
[2] Hou J, et al. Antibody-mediated targeting of human microglial leukocyte Ig-like receptor B4 attenuates amyloid pathology in a mouse model. Science Translational Medicine. DOI: 10.1126/scitranslmed.adj9052 (2024).
NIH Support: National Institute of General Medical Sciences, National Institute on Aging
Fear Switch in the Brain May Point to Target for Treating Anxiety Disorders Including PTSD
Posted on by Dr. Monica M. Bertagnolli

There’s a good reason you feel fear creep in when you’re walking alone at night in an unfamiliar place or hear a loud and unexpected noise ring out. In those moments, your brain triggers other parts of your nervous system to set a stress response in motion throughout your body. It’s that fear-driven survival response that keeps you alert, ready to fight or flee if the need arises. But when acute anxiety or traumatic events lead to fear that becomes generalized—occurring often and in situations that aren’t threatening—this can lead to debilitating anxiety disorders, including post-traumatic stress disorder (PTSD).
Just what happens in the brain’s circuitry to turn a healthy fear response into one that’s harmful hasn’t been well understood. Now, research findings by a team led by Nicholas Spitzer and Hui-Quan Li at the University of California San Diego and reported in the journal Science have pinpointed changes in the biochemistry of the brain and neural circuitry that lead to generalized fear.1 The intriguing findings, from research supported in part by NIH, raise the possibility that it might be possible to prevent or reverse this process with treatments targeting this fear “switch.”
To investigate generalized fear in the brain, the researchers first studied mice in the lab, looking at parts of the brain known to be linked to panic-like fear responses, including an area of the brainstem known as the dorsal raphe. They found that, in the mouse brain, acute stress led to a switch in the chemical messengers, or neurotransmitters, in some neurons within this portion of the mouse brain. Specifically, the chemical signals in the neurons flipped from producing excitatory glutamate neurotransmitters to inhibitory GABA neurotransmitters, and this led to a generalized fear response. They also found that the neurons that had undergone this switch are connected to brain regions that are known to play a role in fear responses including the amygdala and lateral hypothalamus. Interestingly, the researchers also showed they could avert generalized fear responses by preventing the production of GABA in the mouse brain.
To further support their research, the study team then examined postmortem brains of people who had PTSD and confirmed a similar switch in neurotransmitters to what happened in the mice. Next, they wanted to find out if they could block the switch by treating mice with the commonly used antidepressant fluoxetine. They found that when mice were treated with fluoxetine in their drinking water promptly after a stressful event, the neurotransmitter switch and subsequent generalized fear were prevented.
The researchers made even more findings about the timing of the switch that could lead to better treatments. They found that in mice, the switch to generalized fear persisted for four weeks after an acutely stressful event—a period that for the mice may be the equivalent of three years in people. This suggests that treatments may prevent generalized fear and the development of anxiety disorders when given before the brain undergoes a neurotransmitter switch. The findings may also explain why treatment doesn’t seem to be as effective in people who are initially treated for PTSD after having it for a long time.
Going forward, the researchers want to explore targeted approaches to reversing this fear switch after it has taken place. The hope is to discover new ways to rid the brain of generalized fear responses and help treat anxiety disorders including PTSD, a condition which will affect more than six in every 100 people at some point in their lives.2
References:
[1] Li HQ, et al. Generalized fear after acute stress is caused by change in neuronal cotransmitter identity. Science. DOI: 10.1126/science.adj5996 (2024).
[2] Post-Traumatic Stress Disorder (PTSD). National Institute of Mental Health.
NIH Support: National Institute of Neurological Disorders and Stroke
Understanding Causes of Devastating Neurodegenerative Condition Affecting Children
Posted on by Lawrence Tabak, D.D.S., Ph.D.

A common theme among parents and family members caring for a child with the rare Batten disease is “love, hope, cure.” While inspiring levels of love and hope are found among these amazing families, a cure has been more elusive. One reason is rooted in the need for more basic research. Although researchers have identified an altered gene underlying Batten disease, they’ve had difficulty pinpointing where and how the gene’s abnormal protein product malfunctions, especially in cells within the nervous system.
Now, this investment in more basic research has paid off. In a paper just published in the journal Nature Communications, an international research team pinpointed where and how a key cellular process breaks down in the nervous system to cause Batten disease, sometimes referred to as CLN3 disease [1]. While there’s still a long way to go in learning exactly how to overcome the cellular malfunction, the findings mark an important step forward toward developing targeted treatments for Batten disease and progress in the quest for a cure.
The research also offers yet another excellent example of how studying rare diseases helps to advance our fundamental understanding of human biology. It shows that helping those touched by Batten disease can shed a brighter light on basic cellular processes that drive other diseases, rare and common.
Batten disease affects about 14,000 people worldwide [2]. For those with the juvenile form of this inherited disease of the nervous system, parents may first notice their seemingly healthy child has difficulty saying words, sudden problems with vision or movement, and changes in behavior. Tragically for parents, with no approved treatments to reverse these symptoms, the disease will worsen, leading to severe vision loss, frequent seizures, and impaired motor skills. The disease can be fatal as early as late childhood or the teenage years.
Batten disease also goes by the more technical name of juvenile neuronal ceroid lipofuscinosis. Using this technical name, it represents one of the more than 70 medically recognized lysosomal storage disorders.
These disorders share a breakdown in the ability of membrane-bound cellular components, known as lysosomes, to degrade the molecular waste products of normal cell biology. As a result, all this undegraded material builds up and eventually kills affected cells. In people with Batten disease, the lost and damaged cells cause progressive dysfunction within the nervous system.
Researchers have known for a while that the most common cause of this breakdown in people with Batten disease is the inheritance of two defective copies of a gene called CLN3. As mentioned above, what’s been missing is a more detailed understanding of what exactly a working copy of the CLN3 gene does and how its loss leads to the changes seen in those with this condition.
Hoping to solve this puzzle was an NIH-supported basic research team led by Alessia Calcagni and Andrea Ballabio, Baylor College of Medicine and Texas Children’s Hospital, Houston, and Telethon Institute of Genetics and Medicine, Naples, Italy.
As described in their latest paper, the researchers first generated an antibody that allowed them to visualize where in cells the protein encoded by CLN3 is found. Their studies unexpectedly showed that this protein has a role outside, not inside, the cell’s estimated 50-to-1,000 lysosomes. Before reaching the lysosomes, the protein first moves through another cellular component called the Golgi body, where many proteins are packaged.
They then identified all the other proteins that interact with the CLN3 protein in the Golgi body and elsewhere in the cell. Their data showed that CLN3 interacts with proteins known for transporting other proteins within the cell and forming new lysosomes.
That gave them a valuable clue: the CLN3 gene must be a player in these fundamentally important cellular processes of protein transport and lysosome formation. Among the proteins CLN3 interacts with in the Golgi body is a particular receptor called M6PR. The receptor known for its role in recognizing lysosomal enzymes and delivering them to the lysosomes, where they go to work inside these bubble-like structures degrading cellular waste products.
The researchers found that loss of CLN3 led this important M6PR receptor to be broken down within lysosomes. The breakdown, in turn, altered the normal shape of new lysosomes, and that limits their functionality. The researchers also showed that restoring CLN3 in cells that lacked this gene also restored the production of more functional lysosomes and lysosomal enzymes.
Overall, the findings point to a major role for CLN3 in the formation of lysosomes and their ability to function. Importantly, the findings also offer clues for understanding the mechanisms that underlie other forms of lysosomal storage disease, which collectively affect as many as one in every 40,000 people [3]. The work also may have broader implications for common neurodegenerative diseases, such as Parkinson’s and Alzheimer’s disease.
Most of all, this paper demonstrates the power of basic research to define needed molecular targets. It shows how these fundamental studies are helping families affected by Batten disease and supporting their love, hope, and quest for a cure.
References:
[1] Loss of the batten disease protein CLN3 leads to mis-trafficking of M6PR and defective autophagic-lysosomal reformation. Calcagni’ A, Staiano L, Zampelli N, Minopoli N, Herz NJ, Cullen PJ, Parenti G, De Matteis MA, Grumati P, Ballabio A, et al. Nat Commun. 2023 Jul 3;14(1):3911. doi: 10.1038/s41467-023-39643-7. PMID: 37400440; PMCID: PMC10317969.
[2] Batten Disease. Boston Children’s Hospital.
[3] Lysosomal storage diseases. Cleveland Clinic fact sheet, June 27, 2022.
Links:
Batten Disease (National Institute of Neurological Disorders and Stroke/NIH)
Rare Diseases (NIH)
Alessia Calcagni (Baylor College of Medicine, Houston, TX)
Andrea Ballabio (Telethon Institute of Genetics and Medicine, Naples, Italy)
NIH Support: National Institute of Neurological Disorders and Stroke; National Cancer Institute; National Center for Advancing Translational Sciences
Saving Fat for Lean Times
Posted on by Lawrence Tabak, D.D.S., Ph.D.
Humans and all multi-celled organisms, or metazoans, have evolved through millennia into a variety of competing shapes, sizes, and survival strategies. But all metazoans still share lots of intriguing cell biology, including the ability to store excess calories as fat. In fact, many researchers now consider fat-storing cells to be “nutrient sinks,” or good places for the body to stash excess sugars and lipids. Not only can these provide energy needed to survive a future famine, this is a good way to sequester extra molecules that could prove toxic to cells and organs.
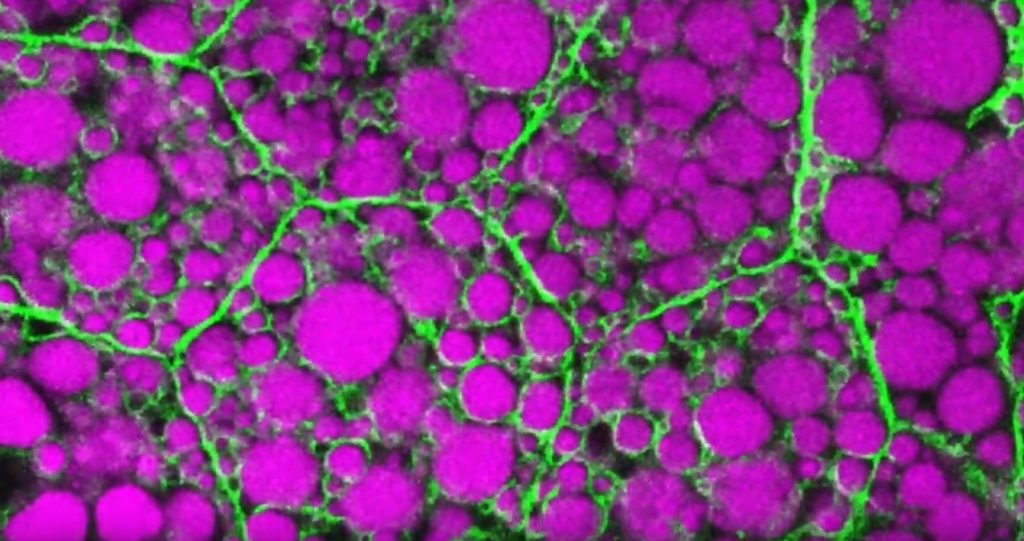
Here’s something to think about the next time you skip a meal. Fat-storing cells organize their fat reserves spatially, grouping them into specific pools of lipid types, in order to generate needed energy when food is scarce.
That’s the story behind this striking image taken in a larval fruit fly (Drosophila melanogaster). The image captures fat-storing adipocytes in an organ called a fat body, where a larval fruit fly stores extra nutrients. It’s like the fat tissue in mammals. You can see both large and small lipid droplets (magenta) inside polygon-shaped fat cells, or adipocytes, lined by their plasma membranes (green). But notice that the small lipid droplets are more visibly lined by green, as only these are destined to be saved for later and exported when needed into the fly’s bloodstream.
Working in Mike Henne’s lab at the University of Texas Southwestern Medical Center, Dallas, research associate Rupali Ugrankar discovered how this clever fat-management system works in Drosophila [1]. After either feeding flies high-or-extremely low-calorie diets, Ugrankar used a combination of high-resolution fluorescence confocal microscopy and thin-section transmission electron microscopy to provide a three-dimensional view of adipocytes and their lipid droplets inside.
She observed two distinct sizes of lipid droplets and saw that only the small ones clustered at the cell surface membrane. The adipocytes contorted their membrane inward to grab these small droplets and package them into readily exportable energy bundles.
Ugrankar saw that during times of plenty, a protein machine could fill these small membrane-wrapped fat droplets with lots of triacylglycerol, a high-energy, durable form of fat storage. Their ready access at the surface of the adipocyte allows the fly to balance lipid storage locally with energy release into its blood in times of famine.
Ugrankar’s adeptness at the microscope resulted in this beautiful photo, which was earlier featured in the American Society for Cell Biology’s Green Fluorescent Protein Image and Video Contest. But her work and that of many others help to open a vital window into nutrition science and many critical mechanistic questions about the causes of obesity, insulin resistance, hyperglycemia, and even reduced lifespan.
Such basic research will provide the basis for better therapies to correct these nutrition-related health problems. But the value of basic science must not be forgotten—some of the most important leads could come from a tiny insect in its larval state that shares many aspects of mammalian metabolism.
Reference:
[1] Drosophila Snazarus regulates a lipid droplet population at plasma membrane-droplet contacts in adipocytes. Ugrankar R, Bowerman J, Hariri H, Chandra M, et al. Dev Cell. 2019 Sep 9;50(5):557-572.e5.
Links:
The Interactive Fly (Society for Developmental Biology, Rockville, MD)
Henne Lab (University of Texas Southwestern Medical Center, Dallas)
NIH Support: National Institute of General Medical Sciences
A Look Back at Science’s 2022 Breakthroughs
Posted on by Lawrence Tabak, D.D.S., Ph.D.
Happy New Year! I hope everyone finished 2022 with plenty to celebrate, whether it was completing a degree or certification, earning a promotion, attaining a physical fitness goal, or publishing a hard-fought scientific discovery.
If the latter, you are in good company. Last year produced some dazzling discoveries, and the news and editorial staff at the journal Science kept a watchful eye on the most high-impact advances of 2022. In December, the journal released its list of the top 10 advances across the sciences, from astronomy to zoology. In case you missed it, Science selected NASA’s James Webb Space Telescope (JWST) as the 2022 Breakthrough of the Year [1].
This unique space telescope took 20 years to complete, but it has turned out to be time well spent. Positioned 1.5-million-kilometers from Earth, the JWST and its unprecedented high-resolution images of space have unveiled the universe anew for astronomers and wowed millions across the globe checking in online. The telescope’s image stream, beyond its sheer beauty, will advance study of the early Universe, allowing astronomers to discover distant galaxies, explore the early formation of stars, and investigate the possibility of life on other planets.
While the biomedical sciences didn’t take home the top prize, they were well represented among Science’s runner-up breakthroughs. Some of these biomedical top contenders also have benefited, directly or indirectly, from NIH efforts and support. Let’s take a look:
RSV vaccines nearing the finish line: It’s been one of those challenging research marathons. But scientists last year started down the homestretch with the first safe-and-effective vaccine for respiratory syncytial virus (RSV), a leading cause of severe respiratory illness in the very young and the old.
In August, the company Pfizer presented evidence that its experimental RSV vaccine candidate offered protection for those age 60 and up. Later, they showed that the same vaccine, when administered to pregnant women, helped to protect their infants against RSV for six months after birth. Meanwhile, in October, the company GSK announced encouraging results from its late-stage phase III trial of an RSV vaccine in older adults.
As Science noted, the latest clinical progress also shows the power of basic science. For example, researchers have been working with chemically inactivated versions of the virus to develop the vaccine. But these versions have a key viral surface protein that changes its shape after fusing with a cell to start an infection. In this configuration, the protein elicits only weak levels of needed protective antibodies.
Back in 2013, Barney Graham, then with NIH’s National Institute of Allergy and Infectious Diseases (NIAID), and colleagues, solved the problem [2]. Graham’s NIH team discovered a way to lock the protein into its original prefusion state, which the immune system can better detect. This triggers higher levels of potent antibodies, and the discovery kept the science—and the marathon—moving forward.
These latest clinical advances come as RSV and other respiratory viruses, including SARS-CoV-2, the cause of COVID-19, are sending an alarming number of young children to the hospital. The hope is that researchers will cross the finish line this year or next, and we’ll have the first approved RSV vaccine.
Virus fingered as cause of multiple sclerosis: Researchers have long thought that multiple sclerosis, or MS, has a viral cause. Pointing to the right virus with the required high degree of certainty has been the challenge, slowing progress on the treatment front for those in need. As published in Science last January, Alberto Ascherio, Harvard T.H. Chan School of Public Health, Boston, and colleagues produced the strongest evidence yet that MS is caused by the Epstein-Barr virus (EBV), a herpesvirus also known for causing infectious mononucleosis [3].
The link between EBV and MS had long been suspected. But it was difficult to confirm because EBV infections are so widespread, and MS is so disproportionately rare. In the recent study, the NIH-supported researchers collected blood samples every other year from more than 10 million young adults in the U.S. military, including nearly 1,000 who were diagnosed with MS during their service. The evidence showed that the risk of an MS diagnosis increased 32-fold after EBV infection, but it held steady following infection with any other virus. Levels in blood serum of a biomarker for MS neurodegeneration also went up only after an EBV infection, suggesting that the viral illness is a leading cause for MS.
Further evidence came last year from a discovery published in the journal Nature by William Robinson, Stanford University School of Medicine, Stanford, CA, and colleagues. The NIH-supported team found a close resemblance between an EBV protein and one made in the healthy brain and spinal cord [4]. The findings suggest an EBV infection may produce antibodies that mistakenly attack the protective sheath surrounding our nerve cells. Indeed, the study showed that up to one in four people with MS had antibodies that bind both proteins.
This groundbreaking research suggests that an EBV vaccine and/or antiviral drugs that thwart this infection might ultimately prevent or perhaps even cure MS. Of note, NIAID launched last May an early-stage clinical trial for an experimental EBV vaccine at the NIH Clinical Center, Bethesda, MD.
AI Gets Creative: Science’s 2021 Breakthrough of the Year was AI-powered predictions of protein structure. In 2022, AI returned to take another well-deserved bow. This time, Science singled out AI’s now rapidly accelerating entry into once uniquely human attributes, such as artistic expression and scientific discovery.
On the scientific discovery side, Science singled out AI’s continued progress in getting creative with the design of novel proteins for vaccines and myriad other uses. One technique, called “hallucination,” generates new proteins from scratch. Researchers input random amino acid sequences into the computer, and it randomly and continuously mutates them into sequences that other AI tools are confident will fold into stable proteins. This greatly simplifies the process of protein design and frees researchers to focus their efforts on creating a protein with a desired function.
AI research now engages scientists around world, including hundreds of NIH grantees. Taking a broader view of AI, NIH recently launched the Artificial Intelligence/Machine Learning Consortium to Advance Health Equity and Researcher Diversity (AIM-AHEAD) Program. It will help to create greater diversity within the field, which is a must. A lack of diversity could perpetuate harmful biases in how AI is used, how algorithms are developed and trained, and how findings are interpreted to avoid health disparities and inequities for underrepresented communities.
And there you have it, some of the 2022 breakthroughs from Science‘s news and editorial staff. Of course, the highlighted biomedical breakthroughs don’t capture the full picture of research progress. There were many other milestone papers published in 2022 that researchers worldwide will build upon in the months and years ahead to make further progress in their disciplines and, for some, draw the attention of Science’s news and editorial staff. Here’s to another productive year in biomedical research, which the blog will continue to feature and share with you as it unfolds in 2023.
References:
[1] 2022 Breakthrough of the Year. Science. Dec 15, 2022.
[2] Structure of RSV fusion glycoprotein trimer bound to a prefusion-specific neutralizing antibody. McLellan JS, Chen M, Leung S, Kwong PD, Graham BS, et al. Science. 2013 May 31;340(6136):1113-1117.
[3] Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. Bjornevik K, Cortese M, Healy BC, Kuhle J, Mina MJ, Leng Y, Elledge SJ, Niebuhr DW, Scher AI, Munger KL, Ascherio A. Science. 2022 Jan 21;375(6578):296-301.
[4] Clonally expanded B cells in multiple sclerosis bind EBV EBNA1 and GlialCAM. Lanz TV, Brewer RC, Steinman L, Robinson WH, et al. Nature. 2022 Mar;603(7900):321-327.
Links:
Respiratory Syncytial Virus (RSV) (National Institute of Allergy and Infectious Diseases/NIH)
Multiple Sclerosis (National Institute of Neurological Disorders and Stroke/NIH)
Barney Graham (Morehouse School of Medicine, Atlanta)
Alberto Ascherio (Harvard T.H. Chan School of Public Health, Boston)
Robinson Lab (Stanford Medicine, Stanford, CA)
James Webb Space Telescope (Goddard Space Flight Center/NASA, Greenbelt, MD)
The Chemistry Clicked: Two NIH-Supported Researchers Win 2022 Nobel Prize in Chemistry
Posted on by Lawrence Tabak, D.D.S., Ph.D.
Through the years, NIH has supported a total of 169 researchers who have received or shared 101 Nobel Prizes. That’s quite a testament to the world-leading science that NIH pursues and its continued impact on improving human health and well-being.
Those numbers include the news late last week that the 2022 Nobel Prize in Chemistry was shared by two long-time grantees for their work on a transformative scientific approach known as “click chemistry.” This form of chemistry has made it possible for researchers to snap together, like LEGO pieces, molecular building blocks to form hybrid biomolecules, often with easy-to-track imaging agents attached. Not only has click chemistry expanded our ability to explore the molecular underpinnings of a wide range of biological processes, but it has provided us with new tools for developing drugs, diagnostics, and a wide array of “smart” materials.
For K. Barry Sharpless, Scripps Research, La Jolla, CA, October 5, 2022 marked the second time that he’s received an early-morning congratulatory call from The Royal Swedish Academy of Sciences. The first such call came in 2001, when Sharpless got the news that he was a co-winner of the Nobel Prize in Chemistry for his discovery of asymmetric catalytic reactions.
This time around, Sharpless was recognized for his groundbreaking studies in the mid-1990s with click chemistry, a term that he coined himself. His initial work established click chemistry as a fast-and-reliable way to attach molecules of interest in the lab [1]. He and co-recipient Morten Meldal, University of Copenhagen, Denmark, who is not funded by NIH, then independently introduced a copper-catalyzed click that further refined the chemistry and helped popularize it across biology and the material sciences [2,3].
For Carolyn R. Bertozzi of Stanford University, Palo Alto, CA, it is her first Nobel. Bertozzi was recognized for expanding the use of click chemistry with so-called bioorthogonal chemistry, which is a copper-free version of the approach that can be used inside living cells without the risk of metal-associated toxicities [4,5].
Bertozzi’s work has been especially interesting to me because of her focus on glycans, which I’ve studied throughout my career. Glycans are the carbohydrate molecules that coat the surfaces of our cells and most secreted proteins. They are essential to life, and, in higher organisms, play fundamental roles in basic processes such as metabolism, immunity, and cellular communication.
Glycans also remain poorly understood, largely because, until recently, they have been so difficult for basic scientists to study with traditional techniques. That has changed with development of new tools to study glycans and the enzymes that assemble them. My long-time collaborator, Kelly Ten Hagen, a senior investigator at NIH’s National Institute of Dental and Craniofacial Research, and I collaborated with Carolyn on identifying small molecules that inhibit the enzyme responsible for the first step in mucin-type O-glycosylation [6]
In the early 2000s, Bertozzi and her team introduced bioorthogonal chemistry, which enabled researchers to label glycans and visualize them in a range of cells and living organisms. Her team’s pioneering approach quickly became an essential tool in basic science labs around the world that study glycans, leading to a number of stunning discoveries that would have otherwise been difficult or impossible.
For clinical researchers, click chemistry has emerged as a workhorse in drug discovery and the improved targeting of cancer chemotherapies and other small-molecule drugs. The approach also is being used to improve delivery of antibody-based therapies and to create new biomaterials. Meanwhile, in the material sciences, click chemistry has been used to solve a number of problems in working with polymers and to expand their industrial uses.
Click chemistry is an excellent example of how advances in basic science can build the foundation for a wide range of practical applications, including those aimed at improving human health. It also highlights the value of strong, sustained public funding for fundamental research, and NIH is proud to have supported Sharpless continuously since 1975 and Bertozzi since 1999. I send my sincere congratulations to both of these most-deserving scientists.
References:
[1] Click Chemistry: Diverse chemical function from a few good reactions. Kolb, HC, Finn, MG, Sharpless, KB. Angew. Chem. Int. Ed. 2001, 40 (11), 2004–2021
[2] A stepwise huisgen cycloaddition process: Copper(I)-catalyzed regioselective “Llgation” of azides and terminal alkynes. Rostovtsev VV, Green LG, Fokin VV, Sharpless KB. Angew. Chem. Int. Ed. 2002, 41 (14), 2596–2599.
[3] Peptidotriazoles on solid phase: [1,2,3]-Triazoles by regiospecific copper(I)-catalyzed 1,3-dipolar cycloadditions of terminal alkynes to azides. Tornøe CW, Sengeløv H, Meldal M. J. Org. Chem. 2002, 67 (9), 3057–3064.
[4] A strain-promoted [3 + 2] azide−alkyne cycloaddition for covalent modification of biomolecules in living systems. Agard NJ, Prescher JA, Bertozzi CR. J. Am. Chem. Soc. 2004, 126 (46), 15046–15047
[5] In vivo imaging of membrane associated glycans in developing zebrafish. Laughlin ST, Baskin JM, Amacher SL, Bertozzi CR. Science 2008, 320 (5876), 664–667.
[6] Small molecule inhibitors of mucin-type O-glycosylation from a uridine-based library. Hang, HC, Yu, C, Ten Hagen, KG, Tian, E, Winans, KA, Tabak, LA, Bertozzi, Chem Biol. 2004 Jul;11(7):1009-1016.
Links:
The Nobel Prize in Chemistry 2022 (The Royal Swedish Academy of Sciences, Stockholm)
Video: Announcement of the 2022 Nobel Prize in Chemistry (YouTube)
Click Chemistry and Bioorthogonal Chemistry (The Royal Swedish Academy of Sciences)
Sharpless Lab (Scripps Research, La Jolla, CA)
Bertozzi Group (Stanford University, Palo Alto, CA)
NIH Support:
K. Barry Sharpless: National Institute of General Medical Sciences
Carolyn R. Bertozzi: National Cancer Institute; National Institute of Allergy and Infectious Diseases; National Institute of General Medical Sciences
Understanding Long-Term COVID-19 Symptoms and Enhancing Recovery
Posted on by Walter J. Koroshetz, M.D., National Institute of Neurological Disorders and Stroke
We are in the third year of the COVID-19 pandemic, and across the world, most restrictions have lifted, and society is trying to get back to “normal.” But for many people—potentially millions globally—there is no getting back to normal just yet.
They are still living with the long-term effects of a COVID-19 infection, known as the post-acute sequelae of SARS-CoV-2 infection (PASC), including Long COVID. These people continue to experience debilitating fatigue, shortness of breath, pain, difficulty sleeping, racing heart rate, exercise intolerance, gastrointestinal and other symptoms, as well as cognitive problems that make it difficult to perform at work or school.
This is a public health issue that is in desperate need of answers. Research is essential to address the many puzzling aspects of Long COVID and guide us to effective responses that protect the nation’s long-term health.
For the past two years, NIH’s National Heart, Lung, and Blood Institute (NHLBI), the National Institute of Allergy and Infectious Diseases (NIAID), and my National Institute of Neurological Disorders and Stroke (NINDS) along with several other NIH institutes and the office of the NIH Director, have been leading NIH’s Researching COVID to Enhance Recovery (RECOVER) initiative, a national research program to understand PASC.
The initiative studies core questions such as why COVID-19 infections can have lingering effects, why new symptoms may develop, and what is the impact of SARS-CoV-2, the virus that causes COVID-19, on other diseases and conditions? Answering these fundamental questions will help to determine the underlying biologic basis of Long COVID. The answers will also help to tell us who is at risk for Long COVID and identify therapies to prevent or treat the condition.
The RECOVER initiative’s wide scope of research is also unprecedented. It is needed because Long COVID is so complex, and history indicates that similar post infectious conditions have defied definitive explanation or effective treatment. Indeed, those experiencing Long COVID report varying symptoms, making it highly unlikely that a single therapy will work for everyone, underscoring the need to pursue multiple therapeutic strategies.
To understand Long COVID fully, hundreds of RECOVER investigators are recruiting more than 17,000 adults (including pregnant people) and more than 18,000 children to take part in cohort studies. Hundreds of enrolling sites have been set up across the country. An autopsy research cohort will also provide further insight into how COVID-19 affects the body’s organs and tissues.
In addition, researchers will analyze electronic health records from millions of people to understand how Long COVID and its symptoms change over time. The RECOVER initiative is also utilizing consistent research protocols across all the study sites. The protocols have been carefully developed with input from patients and advocates, and they are designed to allow for consistent data collection, improve data sharing, and help to accelerate the pace of research.
From the very beginning, people suffering from Long COVID have been our partners in RECOVER. Patients and advocates have contributed important perspectives and provided valuable input into the master protocols and research plans.
Now, with RECOVER underway, individuals with Long COVID, their caregivers, and community members continue to serve a critical role in the Initiative. The National Community Engagement Group (NCEG) has been established to make certain that RECOVER meets the needs of all people affected by Long COVID. The RECOVER Patient and Community Engagement Strategy outlines all the approaches that RECOVER is using to engage with and gather input from individuals impacted by Long COVID.
The NIH recently made more than 40 awards to improve understanding of the underlying biology and pathology of Long COVID. There have already been several important findings published by RECOVER scientists.
For example, in a recent study published in the journal Lancet Digital Health, RECOVER investigators used machine learning to comb through electronic health records to look for signals that may predict whether someone has Long COVID [1]. As new findings, tools, and technologies continue to emerge that help advance our knowledge of the condition, the RECOVER Research Review (R3) Seminar Series will provide a forum for researchers and our partners with up-to-date information about Long COVID research.
It is important to note that post-viral conditions are not a new concept. Many, but not all, of the symptoms reported in Long COVID, including fatigue, post-exertional malaise, chronic musculoskeletal pain, sleep disorders, postural orthostatic tachycardia (POTS), and cognitive issues, overlap with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS).
ME/CFS is a serious disease that can occur following infection and make people profoundly sick for decades. Like Long COVID, ME/CFS is a heterogenous condition that does not affect everybody in the same way, and the knowledge gained through research on Long COVID may also positively impact the understanding, treatment, and prevention of POTS, ME/CFS, and other chronic diseases.
Unlike other post-viral conditions, people who experience Long COVID were all infected by the same virus—albeit different variants—at a similar point in time. This creates a unique opportunity for RECOVER researchers to study post-viral conditions in real-time.
The opportunity enables scientists to study many people simultaneously while they are still infected to monitor their progress and recovery, and to try to understand why some individuals develop ongoing symptoms. A better understanding of the transition from acute to chronic disease may offer an opportunity to intervene, identify who is at risk of the transition, and develop therapies for people who experience symptoms long after the acute infection has resolved.
The RECOVER initiative will soon announce clinical trials, leveraging data from clinicians and patients in which symptom clusters were identified and can be targeted by various interventions. These trials will investigate therapies that are indicated for other non-COVID conditions and novel treatments for Long COVID.
Through extensive collaboration across the multiple NIH institutes and offices that contribute to the RECOVER effort, our hope is critical answers will emerge soon. These answers will help us to recognize the full range of outcomes and needs resulting from PASC and, most important, enable many people to make a full recovery from COVID-19. We are indebted to the over 10,000 subjects who have already enrolled in RECOVER. Their contributions and the hard work of the RECOVER investigators offer hope for the future to the millions still suffering from the pandemic.
Reference:
[1] Identifying who has long COVID in the USA: a machine learning approach using N3C data. Pfaff ER, Girvin AT, Bennett TD, Bhatia A, Brooks IM, Deer RR, Dekermanjian JP, Jolley SE, Kahn MG, Kostka K, McMurry JA, Moffitt R, Walden A, Chute CG, Haendel MA; N3C Consortium. Lancet Digit Health. 2022 Jul;4(7):e532-e541.
Links:
COVID-19 Research (NIH)
Long COVID (NIH)
RECOVER: Researching COVID to Enhance Recovery (NIH)
“NIH builds large nationwide study population of tens of thousands to support research on long-term effects of COVID-19,” NIH News Release, September 15, 2021.
Director’s Messages (National Institute of Neurological Disorders and Stroke/NIH)
Note: Dr. Lawrence Tabak, who performs the duties of the NIH Director, has asked the heads of NIH’s Institutes and Centers (ICs) to contribute occasional guest posts to the blog to highlight some of the interesting science that they support and conduct. This is the 18th in the series of NIH IC guest posts that will run until a new permanent NIH director is in place.
Climate Change and Health Initiative to Expand Research, Build Resiliency
Posted on by Richard Woychik, Ph.D., National Institute of Environmental Health Sciences

Climate change is a global process that affects human health in a variety of complex ways. Wildfires, heat waves, hurricanes, floods, and other climate-related weather events can result in illness, injury, and death. Indirect health threats are cause for concern, too. For example, changes in temperature and rainfall can affect the lifecycle of mosquitoes that transmit diseases such as malaria and dengue fever, thereby paving the way for new outbreaks.
Environmental disruptions worsened by climate change can reduce air quality, diminish water resources, and increase exposure to higher temperatures and pathogens. As a result, we see greater health risks in susceptible individuals such as children, the elderly, the poor, and people with underlying conditions, both in America and around the world.
For decades, the National Institute of Environmental Health Sciences and other NIH institutes and centers (ICs) have advanced important research into how climate change affects health. But expanding knowledge in this area and addressing other key challenges will require much more collaboration. The time is now for an all-hands-on-deck scientific effort—across NIH and the wider biomedical research community—that spans many interconnected disciplines and fields of inquiry.
That is why I am excited to join forces with several other IC directors to launch the NIH Climate Change and Health Initiative. By working together, NIH institutes and centers can harness their technologies, innovative research approaches, and talent to advance the science of climate change and health. Through this timely effort, we will promote resilience in vulnerable communities because our research will help them to understand, prepare for, and recover from climate-related health challenges.
Our Strategic Framework outlines why it is important to go beyond studying the health effects of climate change. We must involve impacted communities in solutions-focused research that empowers them, health care practitioners, and health and social services agencies to reduce climate-related health risks. By generating scientific evidence for public health action, we can use a health equity approach to boost climate resiliency among at-risk groups, whether in the U.S. or low- and middle-income countries.
At the heart of the initiative is a push for transdisciplinary, team-based science that boosts training, research capacity, and community engagement. Our immediate goals are to use existing grant programs to strengthen research infrastructure and enhance communication, internally and externally.
Also, with dedicated support from several ICs and the Office of the Director (OD), NIH is funding a research coordinating center and a community engagement program. The coordinating center will help NIH scientists collaborate and manage data. And the community engagement program will empower underserved populations by encouraging two-way dialogue in which both scientists and community members learn from each other. That inclusive approach will improve research and mitigation efforts and reduce health disparities.
In addition, several Notices of Special Interest are now open for applications. The NIH invites scientists to submit research proposals outlining how they plan either to study the health effects of climate change or develop new technologies to mitigate those effects. Also, with OD support, a Climate and Health Scholars Program will launch later this year. Scientists working on important research will share their expertise and methodologies with the NIH community, spurring opportunities for further collaboration.
Going forward, any additional support from the White House, Congress, and the public will allow NIH to further expand the initiative. For example, we urgently need to test novel interventions for reducing heat stress among agricultural workers and to scale up early-warning systems for climate-related weather events. There is also opportunity to use laboratory-based and clinical methodologies to expand knowledge of how climate factors, such as heat and humidity, affect key cellular systems, including mitochondrial function.
To fill those and other research gaps, we must draw on an array of skill sets and fields of inquiry. Therefore, our Strategic Framework outlines the importance of supporting adaptation research, basic and mechanistic studies, behavioral and social sciences research, data integration, disaster research response, dissemination and implementation science, epidemiology and predictive modeling, exposure and risk assessment, and systems science. Tapping into those areas will help us tackle climate-related health challenges and develop effective solutions.
In recent years, in-depth reports and assessments have provided conclusive evidence that climate change is significantly altering our environment and impacting human health. Although the science of climate change and health has progressed, much work remains. We hope that the Climate Change and Health Initiative expands scientific partnerships and capacity throughout NIH and across the global biomedical and environmental health sciences communities. Greater collaboration will spur new knowledge, interventions, and technologies that help humanity manage the health effects of climate change and strengthen health equity.
(Note: The Initiative’s Executive Committee includes the following IC directors: Richard Woychik, National Institute of Environmental Health Sciences [chair]; Diana Bianchi, Eunice Kennedy Shriver National Institute of Child Health and Human Development; Gary Gibbons, National Heart, Lung, and Blood Institute; Roger Glass, Fogarty International Center; Joshua Gordon, National Institute of Mental Health; Eliseo Pérez-Stable, National Institute on Minority Health and Health Disparities; and Shannon Zenk, National Institute of Nursing Research.)
Links:
Environmental Health Topic: Climate Change (National Institute of Environmental Health Sciences /NIH)
NIH Climate Change and Health Initiative (NIH)
NIH Climate Change and Health Initiative Strategic Framework (NIH)
Research Coordinating Center to Support Climate Change and Health Community of Practice (NIH)
Research Opportunity Announcement: Alliance for Community Engagement—Climate Change and Health (National Heart, Lung, and Blood Institute / NIH)
Notice of Special Interest: Climate Change and Health (NIH)
Note: Dr. Lawrence Tabak, who performs the duties of the NIH Director, has asked the heads of NIH’s Institutes and Centers (ICs) to contribute occasional guest posts to the blog to highlight some of the interesting science that they support and conduct. This is the 14th in the series of NIH IC guest posts that will run until a new permanent NIH director is in place.
NCI Support for Basic Science Paves Way for Kidney Cancer Drug Belzutifan
Posted on by Norman "Ned" Sharpless, M.D., National Cancer Institute

There’s exciting news for people with von Hippel-Lindau (VHL) disease, a rare genetic disorder that can lead to cancerous and non-cancerous tumors in multiple organs, including the brain, spinal cord, kidney, and pancreas. In August 2021, the U.S. Food and Drug Administration (FDA) approved belzutifan (Welireg), a new drug that has been shown in a clinical trial led by National Cancer Institute (NCI) researchers to shrink some tumors associated with VHL disease [1], which is caused by inherited mutations in the VHL tumor suppressor gene.
As exciting as this news is, relatively few people have this rare disease. The greater public health implication of this advancement is for people with sporadic, or non-inherited, clear cell kidney cancer, which is by far the most common subtype of kidney cancer, with more than 70,000 cases and about 14,000 deaths per year. Most cases of sporadic clear cell kidney cancer are caused by spontaneous mutations in the VHL gene.
This advancement is also a great story of how decades of support for basic science through NCI’s scientists in the NIH Intramural Research Program and its grantees through extramural research funding has led to direct patient benefit. And it’s a reminder that we never know where basic science discoveries might lead.
Belzutifan works by disrupting the process by which the loss of VHL in a tumor turns on a series of molecular processes. These processes involve the hypoxia-inducible factor (HIF) transcription factor and one of its subunits, HIF-2α, that lead to tumor formation.
The unraveling of the complex relationship among VHL, the HIF pathway, and cancer progression began in 1984, when Bert Zbar, Laboratory of Immunobiology, NCI-Frederick; and Marston Linehan, NCI’s Urologic Oncology Branch, set out to find the gene responsible for clear cell kidney cancer. At the time, there were no effective treatments for advanced kidney cancer, and 80 percent of patients died within two years.
Zbar and Linehan started by studying patients with sporadic clear cell kidney cancer, but then turned their focus to investigations of people affected with VHL disease, which predisposes a person to developing clear cell kidney cancer. By studying the patients and the genetic patterns of tumors collected from these patients, the researchers hypothesized that they could find genes responsible for kidney cancer.
Linehan established a clinical program at NIH to study and manage VHL patients, which facilitated the genetic studies. It took nearly a decade, but, in 1993, Linehan, Zbar, and Michael Lerman, NCI-Frederick, identified the VHL gene, which is mutated in people with VHL disease. They soon discovered that tumors from patients with sporadic clear cell kidney cancer also have mutations in this gene.
Subsequently, with NCI support, William G. Kaelin Jr., Dana-Farber Cancer Institute, Boston, discovered that VHL is a tumor suppressor gene that, when inactivated, leads to the accumulation of HIF.
Another NCI grantee, Gregg L. Semenza, Johns Hopkins School of Medicine, Baltimore, identified HIF as a transcription factor. And Peter Ratcliffe, University of Oxford, United Kingdom, discovered that HIF plays a role in blood vessel development and tumor growth.
Kaelin and Ratcliffe simultaneously showed that the VHL protein tags a subunit of HIF for destruction when oxygen levels are high. These results collectively answered a very old question in cell biology: How do cells sense the intracellular level of oxygen?
Subsequent studies by Kaelin, with NCI’s Richard Klausner and Linehan, revealed the critical role of HIF in promoting the growth of clear cell kidney cancer. This work ultimately focused on one member of the HIF family, the HIF-2α subunit, as the key mediator of clear cell kidney cancer growth.
The fundamental work of Kaelin, Semenza, and Ratcliffe earned them the 2019 Nobel Prize in Physiology or Medicine. It also paved the way for drug discovery efforts that target numerous points in the pathway leading to clear cell kidney cancer, including directly targeting the transcriptional activity of HIF-2α with belzutifan.
Clinical trials of belzutifan, including several supported by NCI, demonstrated potent anti-cancer activity in VHL-associated kidney cancer, as well as other VHL-associated tumors, leading to the aforementioned recent FDA approval. This is an important development for patients with VHL disease, providing a first-in-class therapy that is effective and well-tolerated.
We believe this is only the beginning for belzutifan’s use in patients with cancer. A number of trials are now studying the effectiveness of belzutifan for sporadic clear cell kidney cancer. A phase 3 trial is ongoing, for example, to look at the effectiveness of belzutifan in treating people with advanced kidney cancer. And promising results from a phase 2 study show that belzutifan, in combination with cabozantinib, a widely used agent to treat kidney cancer, shrinks tumors in patients previously treated for metastatic clear cell kidney cancer [2].
This is a great scientific story. It shows how studies of familial cancer and basic cell biology lead to effective new therapies that can directly benefit patients. I’m proud that NCI’s support for basic science, both intramurally and extramurally, is making possible many of the discoveries leading to more effective treatments for people with cancer.
References:
[1] Belzutifan for Renal Cell Carcinoma in von Hippel-Lindau Disease. Jonasch E, Donskov F, Iliopoulos O, Rathmell WK, Narayan VK, Maughan BL, Oudard S, Else T, Maranchie JK, Welsh SJ, Thamake S, Park EK, Perini RF, Linehan WM, Srinivasan R; MK-6482-004 Investigators. N Engl J Med. 2021 Nov 25;385(22):2036-2046.
[2] Phase 2 study of the oral hypoxia-inducible factor 2α (HIF-2α) inhibitor MK-6482 in combination with cabozantinib in patients with advanced clear cell renal cell carcinoma (ccRCC). Choueiri TK et al. J Clin Oncol. 2021 Feb 20;39(6_suppl): 272-272.
Links:
Von Hippel-Lindau Disease (Genetic and Rare Diseases Information Center/National Center for Advancing Translational Sciences/NIH)
Clear Cell Renal Cell Carcinoma (National Cancer Institute/NIH)
Belzutifan Approved to Treat Tumors Linked to Inherited Disorder VHL, Cancer Currents Blog, National Cancer Institute, September 21, 2021.
The Long Road to Understanding Kidney Cancer (Intramural Research Program/NIH)
[Note: Acting NIH Director Lawrence Tabak has asked the heads of NIH’s institutes and centers to contribute occasional guest posts to the blog as a way to highlight some of the cool science that they support and conduct. This is the first in the series of NIH institute and center guest posts that will run until a new permanent NIH director is in place.]
NIH’s Nobel Winners Demonstrate Value of Basic Research
Posted on by Dr. Francis Collins

Last week was a big one for both NIH and me. Not only did I announce my plans to step down as NIH Director by year’s end to return to my lab full-time, I was reminded by the announcement of the 2021 Nobel Prizes of what an honor it is to be affiliated an institution with such a strong, sustained commitment to supporting basic science.
This year, NIH’s Nobel excitement started in the early morning hours of October 4, when two NIH-supported neuroscientists in California received word from Sweden that they had won the Nobel Prize in Physiology or Medicine. One “wake up” call went to David Julius, University of California, San Francisco (UCSF), who was recognized for his groundbreaking discovery of the first protein receptor that controls thermosensation, the body’s perception of temperature. The other went to his long-time collaborator, Ardem Patapoutian, Scripps Research Institute, La Jolla, CA, for his seminal work that identified the first protein receptor that controls our sense of touch.
But the good news didn’t stop there. On October 6, the 2021 Nobel Prize in Chemistry was awarded to NIH-funded chemist David W.C. MacMillan of Princeton University, N.J., who shared the honor with Benjamin List of Germany’s Max Planck Institute. (List also received NIH support early in his career.)
The two researchers were recognized for developing an ingenious tool that enables the cost-efficient construction of “greener” molecules with broad applications across science and industry—including for drug design and development.
Then, to turn this into a true 2021 Nobel Prize “hat trick” for NIH, we learned on October 12 that two of this year’s three Nobel winners in Economic Sciences had been funded by NIH. David Card, an NIH-supported researcher at University of California, Berkley, was recognized “for his empirical contributions to labor economics.” He shared the 2021 prize with NIH grantee Joshua Angrist of Massachusetts Institute of Technology, Cambridge, and his colleague Guido Imbens of Stanford University, Palo Alto, CA, “for their methodological contributions to the analysis of causal relationships.” What a year!
The achievements of these and NIH’s 163 past Nobel Prize winners stand as a testament to the importance of our agency’s long and robust history of investing in basic biomedical research. In this area of research, scientists ask fundamental questions about how life works. The answers they uncover help us to understand the principles, mechanisms, and processes that underlie living organisms, including the human body in sickness and health.
What’s more, each advance builds upon past discoveries, often in unexpected ways and sometimes taking years or even decades before they can be translated into practical results. Recent examples of life-saving breakthroughs that have been built upon years of fundamental biomedical research include the mRNA vaccines for COVID-19 and the immunotherapy approaches now helping people with many types of cancer.
Take the case of the latest Nobels. Fundamental questions about how the human body responds to medicinal plants were the initial inspiration behind the work of UCSF’s Julius. He’d noticed that studies from Hungary found that a natural chemical in chili peppers, called capsaicin, activated a subgroup of neurons to create the painful, burning sensation that most of us have encountered from having a bit too much hot sauce. But what wasn’t known was the molecular mechanism by which capsaicin triggered that sensation.
In 1997, having settled on the best experimental approach to study this question, Julius and colleagues screened millions of DNA fragments corresponding to genes expressed in the sensory neurons that were known to interact with capsaicin. In a matter of weeks, they had pinpointed the gene encoding the protein receptor through which capsaicin interacts with those neurons [1]. Julius and team then determined in follow-up studies that the receptor, later named TRPV1, also acts as a thermal sensor on certain neurons in the peripheral nervous system. When capsaicin raises the temperature to a painful range, the receptor opens a pore-like ion channel in the neuron that then transmit a signal for the unpleasant sensation on to the brain.
In collaboration with Patapoutian, Julius then turned his attention from hot to cold. The two used the chilling sensation of the active chemical in mint, menthol, to identify a protein called TRPM8, the first receptor that senses cold [2, 3]. Additional pore-like channels related to TRPV1 and TRPM8 were identified and found to be activated by a range of different temperatures.
Taken together, these breakthrough discoveries have opened the door for researchers around the world to study in greater detail how our nervous system detects the often-painful stimuli of hot and cold. Such information may well prove valuable in the ongoing quest to develop new, non-addictive treatments for pain. The NIH is actively pursuing some of those avenues through its Helping to End Addiction Long-termSM (HEAL) Initiative.
Meanwhile, Patapoutian was busy cracking the molecular basis of another basic sense: touch. First, Patapoutian and his collaborators identified a mouse cell line that produced a measurable electric signal when individual cells were poked. They had a hunch that the electrical signal was generated by a protein receptor that was activated by physical pressure, but they still had to identify the receptor and the gene that coded for it. The team screened 71 candidate genes with no luck. Then, on their 72nd try, they identified a touch receptor-coding gene, which they named Piezo1, after the Greek word for pressure [4].
Patapoutian’s group has since found other Piezo receptors. As often happens in basic research, their findings have taken them in directions they never imagined. For example, they have discovered that Piezo receptors are involved in controlling blood pressure and sensing whether the bladder is full. Fascinatingly, these receptors also seem to play a role in controlling iron levels in red blood cells, as well as controlling the actions of certain white blood cells, called macrophages.
Turning now to the 2021 Nobel in Chemistry, the basic research of MacMillan and List has paved the way for addressing a major unmet need in science and industry: the need for less expensive and more environmentally friendly catalysts. And just what is a catalyst? To build the synthetic molecules used in drugs and a wide range of other materials, chemists rely on catalysts, which are substances that control and accelerate chemical reactions without becoming part of the final product.
It was long thought there were only two major categories of catalysts for organic synthesis: metals and enzymes. But enzymes are large, complex proteins that are hard to scale to industrial processes. And metal catalysts have the potential to be toxic to workers, as well as harmful to the environment. Then, about 20 years ago, List and MacMillan, working independently from each other, created a third type of catalyst. This approach, known as asymmetric organocatalysis [5, 6], builds upon small organic molecule catalysts that have a stable framework of carbon atoms, to which more active chemical groups can attach, often including oxygen, nitrogen, sulfur, or phosphorus.
Organocatalysts have gone on to be applied in ways that have proven to be more cost effective and environmentally friendly than using traditional metal or enzyme catalysts. In fact, this precise new tool for molecular construction is now being used to build everything from new pharmaceuticals to light-absorbing molecules used in solar cells.
That brings us to the Nobel Prize in the Economic Sciences. This year’s laureates showed that it’s possible to reach cause-and-effect answers to questions in the social sciences. The key is to evaluate situations in groups of people being treated differently, much like the design of clinical trials in medicine. Using this “natural experiment” approach in the early 1990s, David Card produced novel economic analyses, showing an increase in the minimum wage does not necessarily lead to fewer jobs. In the mid-1990s, Angrist and Imbens then refined the methodology of this approach, showing that precise conclusions can be drawn from natural experiments that establish cause and effect.
Last year, NIH added the names of three scientists to its illustrious roster of Nobel laureates. This year, five more names have been added. Many more will undoubtedly be added in the years and decades ahead. As I’ve said many times over the past 12 years, it’s an extraordinary time to be a biomedical researcher. As I prepare to step down as the Director of this amazing institution, I can assure you that NIH’s future has never been brighter.
References:
[1] The capsaicin receptor: a heat-activated ion channel in the pain pathway. Caterina MJ, Schumacher MA, Tominaga M, Rosen TA, Levine JD, Julius D. Nature 1997:389:816-824.
[2] Identification of a cold receptor reveals a general role for TRP channels in thermosensation. McKemy DD, Neuhausser WM, Julius D. Nature 2002:416:52-58.
[3] A TRP channel that senses cold stimuli and menthol. Peier AM, Moqrich A, Hergarden AC, Reeve AJ, Andersson DA, Story GM, Earley TJ, Dragoni I, McIntyre P, Bevan S, Patapoutian A. Cell 2002:108:705-715.
[4] Piezo1 and Piezo2 are essential components of distinct mechanically activated cation channels. Coste B, Mathur J, Schmidt M, Earley TJ, Ranade S, Petrus MJ, Dubin AE, Patapoutian A. Science 2010:330: 55-60.
[5] Proline-catalyzed direct asymmetric aldol reactions. List B, Lerner RA, Barbas CF. J. Am. Chem. Soc. 122, 2395–2396 (2000).
[6] New strategies for organic catalysis: the first highly enantioselective organocatalytic Diels-AlderReaction. Ahrendt KA, Borths JC, MacMillan DW. J. Am. Chem. Soc. 2000, 122, 4243-4244.
Links:
Basic Research – Digital Media Kit (NIH)
Curiosity Creates Cures: The Value and Impact of Basic Research (National Institute of General Medical Sciences/NIH)
Explaining How Research Works (NIH)
NIH Basics, Collins FS, Science, 3 Aug 2012. 337; 6094: 503.
NIH’s Commitment to Basic Science, Mike Lauer, Open Mike Blog, March 25, 2016
Nobel Laureates (NIH)
The Nobel Prize in Physiology or Medicine 2021 (The Nobel Assembly at the Karolinska Institutet, Stockholm, Sweden)
Video: Announcement of the 2021 Nobel Prize in Physiology or Medicine (YouTube)
The Nobel Prize in Chemistry 2021 (The Nobel Assembly at the Karolinska Institutet)
Video: Announcement of the 2021 Nobel Prize in Chemistry (YouTube)
The Nobel Prize in Economic Sciences (The Nobel Assembly at the Karolinska Institutet)
Video: Announcement of the 2021 Nobel Prize in Economic Sciences (YouTube)
Julius Lab (University of California San Francisco)
The Patapoutian Lab (Scripps Research, La Jolla, CA)
Benjamin List (Max-Planck-Institut für Kohlenforschung, Mülheim an der Ruhr, Germany)
The MacMillan Group (Princeton University, NJ)
David Card (University of California, Berkeley)
Joshua Angrist (Massachusetts Institute of Technology, Cambridge)
NIH Support:
David Julius: National Institute of Neurological Diseases and Stroke; National Institute of General Medical Sciences; National Institute of Dental and Craniofacial Research
Ardem Patapoutian: National Institute of Neurological Diseases and Stroke; National Institute of Dental and Craniofacial Research; National Heart, Lung, and Blood Institute
David W.C. MacMillan: National Institute of General Medical Sciences
David Card: National Institute on Aging; Eunice Kennedy Shriver National Institute of Child Health and Human Development
Joshua Angrist: Eunice Kennedy Shriver National Institute of Child Health and Human Development
Next Page