blood vessels
Visualizing The Placenta, a Critical but Poorly Understood Organ
Posted on by Diana W. Bianchi, M.D., Eunice Kennedy Shriver National Institute of Child Health and Human Development
The placenta is the Rodney Dangerfield of organs; it gets no respect, no respect at all. This short-lived but critical organ supports pregnancy by bringing nutrients and oxygen to the fetus, removing waste, providing immune protection, and producing hormones to support fetal development.
It also influences the lifelong health of both mother and child. Problems with the placenta can lead to preeclampsia, gestational diabetes, poor fetal growth, preterm birth, and stillbirth. Although we were all connected to one, the placenta is the least understood, and least studied, of all human organs.
What we do know about the human placenta largely comes from studying it after delivery. But that’s like studying the heart after it’s stopped beating. It doesn’t help us predict complications in time to avert a crisis.
To fill these knowledge gaps, NIH’s Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) developed the Human Placenta Project (HPP) to noninvasively study the placenta during pregnancy. Since 2014, this approximately $88 million collaborative research effort has been developing ultrasound, magnetic resonance imaging (MRI), and blood-based biomarker methods to study how the placenta functions in real time and in greater detail.
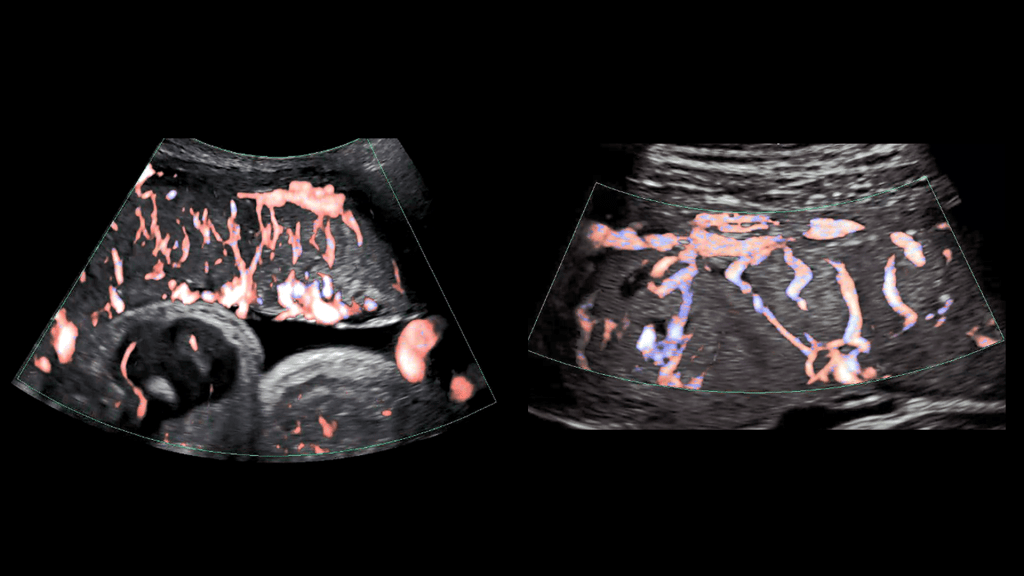
As illustrated in the image above, advanced ultrasound tools allowed HPP researchers at Eastern Virginia Medical School, Norfolk, and the University of Texas Medical Branch, Galveston, to gain a detailed look at the placenta’s intricate arrangement of blood vessels, or vasculature. By evaluating both fetal (left panel) and maternal (right panel) placental vasculature in 610 pregnant people starting at 13 weeks of gestation, the investigators aimed to identify early changes that predicted later complications.
They observed that such changes can start in the first trimester and affect both the vasculature and placental tissue. While further research is needed, these findings suggest that placental ultrasound monitoring can inform efforts to prevent and treat pregnancy complications.
Another HPP team led by Boston Children’s Hospital is developing an MRI strategy to monitor blood flow and oxygen transport through the placenta during pregnancy. Interpreting and visualizing MRI data of the placenta is challenging because of its variable shape, the tendency of muscles in the uterus to begin tightening or contracting well before labor [1], and other factors.
As shown in the video above, the researchers developed a way to account for the motion of the uterus and “freeze” the placenta to make it easier to study (left two panels of video) [2]. They also developed algorithms to better visualize the complex patterns of placental oxygen content during contractions (center panel) [3]. The scientists then carried out initial visualizations of blood flow through the placenta shortly after delivery (second panel from right) [4].
They now intend to map these MRI findings to the placenta itself after delivery (far right panel), which will allow them to explore how additional factors such as gene expression patterns and genetic variants contribute to placental function. Ultimately, they plan to apply these MRI techniques to monitor the placenta in real time during pregnancy and identify changes that indicate compromised function early enough to adjust maternal management as needed.
Other HPP efforts focus on identifying components in maternal blood that reflect the status of the placenta. For example, an HPP research team led by scientists at the University of California, Los Angeles, adapted non-invasive prenatal testing methods to analyze genetic material shed from the placenta into the maternal bloodstream. Their findings suggest that distinctive patterns in this genetic material detected early in pregnancy may indicate risk for later complications [5].
Another HPP team, led by investigators at Columbia University, New York, helped establish that extracellular RNAs (exRNAs) released by the placenta into maternal circulation reflect the placenta’s status at a cellular level beginning in the first trimester. To harness the potential of exRNA biomarkers, the investigators are optimizing methods to isolate, sequence, and analyze exRNAs in maternal blood.
These are just a few examples of the cutting-edge work being funded through the HPP, which complements NICHD’s longstanding investment in basic research to unravel the physiology of and real-time gene expression in the placenta. Unlocking the secrets of the placenta may one day help us to prevent and treat a range of common pregnancy complications, while also providing insights into other areas of science and medicine such as cardiovascular disease and aging. NICHD is committed to giving this important organ the respect it deserves.
References:
[1] Placental MRI: Effect of maternal position and uterine contractions on placental BOLD MRI measurements. Abaci Turk E, Abulnaga SM, Luo J, Stout JN, Feldman H, Turk A, Gagoski B, Wald LL, Adalsteinsson E, Roberts DJ, Bibbo C, Robinson JN, Golland P, Grant PE, Barth, Jr WH. Placenta. 2020 Jun 1; 95: 69-77.
[2] Spatiotemporal alignment of in utero BOLD-MRI series. Turk EA, Luo J, Gagoski B, Pascau J, Bibbo C, Robinson JN, Grant PE, Adalsteinsson E, Golland P, Malpica N. J Magn Reson Imaging. 2017 Aug;46(2):403-412.
[3] Volumetric parameterization of the placenta to a flattened template. Abulnaga SM, Turk EA, Bessmeltsev M, Grant PE, Solomon J, Golland P. IEEE transactions on medical imaging. 2022 April;41(4):925-936.
[4] Placental MRI: development of an MRI compatible ex vivo system for whole placenta dual perfusion. Stout JN, Rouhani S, Turk EA, Ha CG, Luo J, Rich K, Wald LL, Adalsteinsson E, Barth, Jr WH, Grant PE, Roberts DJ. Placenta. 2020 Nov 1; 101: 4-12.
[5] Cell-free DNA methylation and transcriptomic signature prediction of pregnancies with adverse outcomes. Del Vecchio G, Li Q, Li W, Thamotharan S, Tosevska A, Morselli M, Sung K, Janzen C, Zhou X, Pellegrini M, Devaskar SU. Epigenetics. 2021 Jun;16(6):642-661.
Links:
Human Placenta Project (Eunice Kennedy Shriver National Institute of Child Health and Human Development/NIH)
Preeclampsia (NICHD)
Understanding Gestational Diabetes (NICHD)
Preterm Labor and Birth (NICHD)
Stillbirth (NICHD)
Abuhamad Project Information (NIH RePORTER)
Grant Project Information (NIH RePORTER)
Devaskar Project Information (NIH RePORTER)
Williams Project Information (NIH RePORTER)
Note: Acting NIH Director Lawrence Tabak has asked the heads of NIH’s Institutes and Centers (ICs) to contribute occasional guest posts to the blog to highlight some of the interesting science that they support and conduct. This is the 10th in the series of NIH IC guest posts that will run until a new permanent NIH director is in place.
Can Blood Thinners Keep Moderately Ill COVID-19 Patients Out of the ICU?
Posted on by Dr. Francis Collins
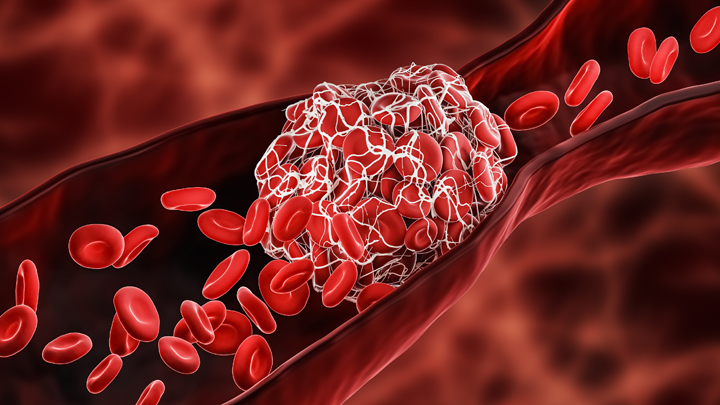
One of many troubling complications of infection with SARS-CoV-2, the coronavirus that causes COVID-19, is its ability to trigger the formation of multiple blood clots, most often in older people but sometimes in younger ones, too. It raises the question of whether and when more aggressive blood thinning treatments might improve outcomes for people hospitalized for COVID-19.
The answer to this question is desperately needed to help guide clinical practice. So, I’m happy to report interim results of three large clinical trials spanning four continents and more than 300 hospitals that are beginning to provide critical evidence on this very question [1]. While it will take time to reach a solid consensus, the findings based on more than 1,000 moderately ill patients suggest that full doses of blood thinners are safe and can help to keep folks hospitalized with COVID-19 from becoming more severely ill and requiring some form of organ support.
The results that are in so far suggest that individuals hospitalized, but not severely ill, with COVID-19 who received a full intravenous dose of the common blood thinner heparin were less likely to need vital organ support, including mechanical ventilation, compared to those who received the lower “prophylactic” subcutaneous dose. It’s important to note that these findings are in contrast to results announced last month indicating that routine use of a full dose of blood thinner for patients already critically ill and in the ICU wasn’t beneficial and may even have been harmful in some cases [2]. This is a compelling example of how critical it is to stratify patients with different severity in clinical trials—what might help one subgroup might be of no benefit, or even harmful, in another.
More study is clearly needed to sort out all the details about when more aggressive blood thinning treatment is warranted. Trial investigators are now working to make the full results available to help inform a doctor’s decisions about how to best to treat their patients hospitalized with COVID-19. It’s worth noting that these trials are overseen by independent review boards, which routinely evaluate the data and are composed of experts in ethics, biostatistics, clinical trials, and blood clotting disorders.
These clinical trials were made possible in part by the Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) public-private partnership and its ACTIV-4 Antithrombotics trials—along with similar initiatives in Canada, Australia, and the European Union. The ACTIV-4 trials are overseen by the NIH’s National Heart, Lung, and Blood institute and funded by Operation Warp Speed.
This ACTIV-4 trial is one of three Phase 3 clinical trials evaluating the safety and effectiveness of blood thinners for patients with COVID-19 [3]. Another ongoing trial is investigating whether blood thinners are beneficial for newly diagnosed COVID-19 patients who do not require hospitalization. There are also plans to explore the use of blood thinners for patients after they’ve been discharged from the hospital following a diagnosis of moderate to severe COVID-19 and to establish more precise methods for identifying which patients with COVID-19 are most at risk for developing life-threatening blood clots.
Meanwhile, research teams are exploring other potentially promising ways to repurpose existing therapeutics and improve COVID-19 outcomes. In fact, the very day that these latest findings on blood thinners were announced, another group at The Montreal Heart Institute, Canada, announced preliminary results of the international COLCORONA trial, testing the use of colchicine—an anti-inflammatory drug widely used to treat gout and other conditions—for patients diagnosed with COVID-19 [4].
Their early findings in treating patients just after a confirmed diagnosis of COVID-19 suggest that colchicine might reduce the risk of death or hospitalization compared to patients given a placebo. In the more than 4,100 individuals with a proven diagnosis of COVID-19, colchicine significantly reduced hospitalizations by 25 percent, the need for mechanical ventilation by 50 percent, and deaths by 44 percent. Still, the actual numbers of individuals represented by these percentages was small.
Time will tell whether and for which patients colchicine and blood thinners prove most useful in treating COVID-19. For those answers, we’ll have to await the analysis of more data. But the early findings on both treatment strategies come as a welcome reminder that we continue to make progress each day on such critical questions about which existing treatments can be put to work to improve outcomes for people with COVID-19. Together with our efforts to slow the spread of SARS-CoV-2, finding better ways to treat those who do get sick and prevent some of the worst outcomes will help us finally put this terrible pandemic behind us.
References:
[1] Full-dose blood thinners decreased need for life support and improved outcome in hospitalized COVID-19 patients. National Heart, Lung, and Blood Institute. January 22, 2021.
[2] NIH ACTIV trial of blood thinners pauses enrollment of critically ill COVID-19 patients. National Heart, Lung, and Blood Institute. December 22, 2020.
[3] NIH ACTIV initiative launches adaptive clinical trials of blood-clotting treatments for COVID-19. National Heart, Lung, and Blood Institute. September 10, 2020.
[4] Colchicine reduces the risk of COVID-19-related complications. The Montreal Heart Institute. January 22, 2021.
Links:
COVID-19 Research (NIH)
Combat COVID (U.S. Department of Health and Human Services, Washington, D.C.)
Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) (NIH)
NIH Support: National Heart, Lung, and Blood Institute
Taking a Closer Look at COVID-19’s Effects on the Brain
Posted on by Dr. Francis Collins

While primarily a respiratory disease, COVID-19 can also lead to neurological problems. The first of these symptoms might be the loss of smell and taste, while some people also may later battle headaches, debilitating fatigue, and trouble thinking clearly, sometimes referred to as “brain fog.” All of these symptoms have researchers wondering how exactly the coronavirus that causes COVID-19, SARS-CoV-2, affects the human brain.
In search of clues, researchers at NIH’s National Institute of Neurological Disorders and Stroke (NINDS) have now conducted the first in-depth examinations of human brain tissue samples from people who died after contracting COVID-19. Their findings, published in the New England Journal of Medicine, suggest that COVID-19’s many neurological symptoms are likely explained by the body’s widespread inflammatory response to infection and associated blood vessel injury—not by infection of the brain tissue itself [1].
The NIH team, led by Avindra Nath, used a high-powered magnetic resonance imaging (MRI) scanner (up to 10 times as sensitive as a typical MRI) to examine postmortem brain tissue from 19 patients. They ranged in age from 5 to 73, and some had preexisting conditions, such as diabetes, obesity, and cardiovascular disease.
The team focused on the brain’s olfactory bulb that controls our ability to smell and the brainstem, which regulates breathing and heart rate. Based on earlier evidence, both areas are thought to be highly susceptible to COVID-19.
Indeed, the MRI images revealed in both regions an unusual number of bright spots, a sign of inflammation. They also showed dark spots, which indicate bleeding. A closer look at the bright spots showed that tiny blood vessels in those areas were thinner than normal and, in some cases, leaked blood proteins into the brain. This leakage appeared to trigger an immune reaction that included T cells from the blood and the brain’s scavenging microglia. The dark spots showed a different pattern, with leaky vessels and clots but no evidence of an immune reaction.
While those findings are certainly interesting, perhaps equally noteworthy is what Nath and colleagues didn’t see in those samples. They could find no evidence in the brain tissue samples that SARS-CoV-2 had invaded the brain tissue. In fact, several methods to detect genetic material or proteins from the virus all turned up empty.
The findings are especially intriguing because there has been some suggestion based on studies in mice that SARS-CoV-2 might cross the blood-brain barrier and invade the brain. Indeed, a recent report by NIH-funded researchers in Nature Neuroscience showed that the viral spike protein, when injected into mice, readily entered the brain along with many other organs [2].
Another recent report in the Journal of Experimental Medicine, which used mouse and human brain tissue, suggests that SARS-CoV-2 may indeed directly infect the central nervous system, including the brain [3]. In autopsies of three people who died from complications of COVID-19, the NIH-supported researchers detected signs of SARS-CoV-2 in neurons in the brain’s cerebral cortex. This work was done using the microscopy-based technique of immunohistochemistry, which uses antibodies to bind to a target, in this case, the virus’s spike protein. Also last month, in a study published in the journal Neurobiology of Disease, another NIH-supported team demonstrated in a series of experiments in cell culture that the SARS-CoV-2 spike protein could cross a 3D model of the blood-brain barrier and infect the endothelial cells that line blood vessels in the brain [4].
Clearly, more research is needed, and NIH’s National Institute of Neurological Disorders and Stroke has just launched the COVID-19 Neuro Databank/Biobank (NeuroCOVID) to collect more clinical information, primarily about COVID-19-related neurological symptoms, complications, and outcomes. Meanwhile, Nath and colleagues continue to explore how COVID-19 affects the brain and triggers the neurological symptoms often seen in people with COVID-19. As we learn more about the many ways COVID-19 wreaks havoc on the body, understanding the neurological symptoms will be critical in helping people, including the so-called Long Haulers bounce back from this terrible viral infection.
References:
[1] Microvascular Injury in the Brains of Patients with Covid-19. Lee MH, Perl DP, Nair G, Li W, Maric D, Murray H, Dodd SJ, Koretsky AP, Watts JA, Cheung V, Masliah E, Horkayne-Szakaly I, Jones R, Stram MN, Moncur J, Hefti M, Folkerth RD, Nath A. N Engl J Med. 2020 Dec 30.
[2] The S1 protein of SARS-CoV-2 crosses the blood-brain barrier in mice. Rhea EM, Logsdon AF, Hansen KM, Williams LM, Reed MJ, Baumann KK, Holden SJ, Raber J, Banks WA, Erickson MA. Nat Neurosci. 2020 Dec 16.
[3] Neuroinvasion of SARS-CoV-2 in human and mouse brain. Song E, Zhang C, Israelow B, et al. J Exp Med (2021) 218 (3): e20202135.
[4] The SARS-CoV-2 spike protein alters barrier function in 2D static and 3D microfluidic in-vitro models of the human blood-brain barrier. Buzhdygan TP, DeOre BJ, Baldwin-Leclair A, Bullock TA, McGary HM, Khan JA, Razmpour R, Hale JF, Galie PA, Potula R, Andrews AM, Ramirez SH. Neurobiol Dis. 2020 Dec;146:105131.
Links:
COVID-19 Research (NIH)
Avindra Nath (National Institute of Neurological Disorders and Stroke/NIH)
NIH Support: National Institute of Neurological Disorders and Stroke; National Institute on Aging; National Institute of General Medical Sciences; National Cancer Institute; National Institute of Mental Health
Using MicroRNA to Starve a Tumor?
Posted on by Dr. Francis Collins
Tumor cells thrive by exploiting the willingness of normal cells in their neighborhood to act as accomplices. One of their sneakier stunts involves tricking the body into helping them form new blood vessels. This growth-enabling process of sprouting new blood vessels, called tumor angiogenesis, remains a vital area of cancer research and continues to yield important clues into how to beat this deadly disease.
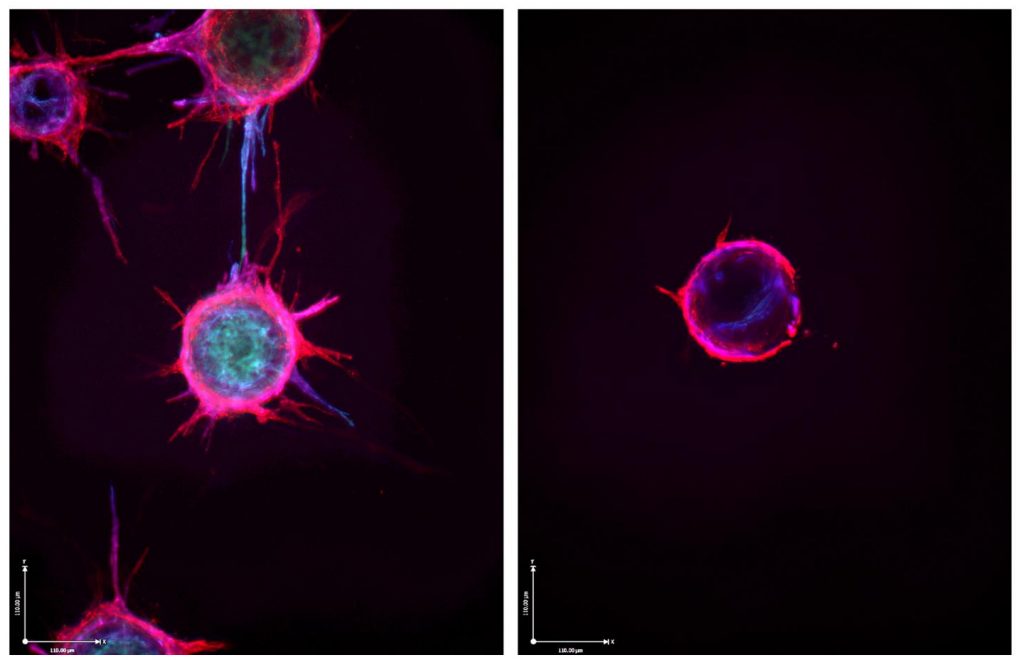
The two-panel image above shows one such promising lead from recent lab studies with endothelial cells, specialized cells that line the inside of all blood vessels. In tumors, endothelial cells are induced to issue non-stop SOS signals that falsely alert the body to dispatch needed materials to rescue these cells. The endothelial cells then use the help to replicate and sprout new blood vessels.
The left panel demonstrates the basics of this growth process under normal conditions. Endothelial cells (red and blue) were cultured under special conditions that help them grow in the lab. When given the right cues, those cells sprout spiky extensions to form new vessels.
But in the right panel, the cells can’t sprout. The reason is because the cells are bathed in a molecule called miR-30c, which isn’t visible in the photo. These specialized microRNA molecules—and humans make a few thousand different versions of them—control protein production by binding to and disabling longer RNA templates, called messenger RNA.
This new anti-angiogenic lead, published in the Journal of Clinical Investigation, comes from a research team led by Andrew Dudley, University of Virginia Medical School, Charlottesville [1]. The team made its discovery while studying a protein called TGF-beta that tumors like to exploit to fuel their growth.
Their studies in mice showed that loss of TGF-beta signals in endothelial cells blocked the growth of new blood vessels and thus tumors. Further study showed that those effects were due in part to elevated levels of miR-30c. The two interact in endothelial cells as part of a previously unrecognized signaling pathway that coordinates the growth of new blood vessels in tumors.
Dudley’s team went on to show that levels of miR-30c vary widely amongst endothelial cells, even when those cells come from the very same tumor. Cells rich in miR-30c struggled to sprout new vessels, while those with less of this microRNA grew new vessels with ease.
Intriguingly, they found that levels of this microRNA also predicted the outcomes for patients with breast cancer. Those whose cancers had high levels of the vessel-stunting miR-30c fared better than those with lower miR-30c levels. While more research is needed, it does offer a potentially promising new lead in the fight against cancer.
Reference:
[1] Endothelial miR-30c suppresses tumor growth via inhibition of TGF-β-induced Serpine1. McCann JV, Xiao L, Kim DJ, Khan OF, Kowalski PS, Anderson DG, Pecot CV, Azam SH, Parker JS, Tsai YS, Wolberg AS, Turner SD, Tatsumi K, Mackman N, Dudley AC. J Clin Invest. 2019 Mar 11;130:1654-1670.
Links:
Angiogenesis Inhibitors (National Cancer Institute/NIH)
Dudley Lab (University of Virginia School of Medicine, Charlottesville)
NIH Support: National Cancer Institute; National Heart, Lung, and Blood Institute
Making Personalized Blood-Brain Barriers in a Dish
Posted on by Dr. Francis Collins

The blood-brain barrier, or BBB, is a dense sheet of cells that surrounds most of the brain’s blood vessels. The BBB’s tiny gaps let vital small molecules, such as oxygen and water, diffuse from the bloodstream into the brain while helping to keep out larger, impermeable foreign substances that don’t belong there.
But in people with certain neurological disorders—such as amyotrophic lateral sclerosis (ALS) and Huntington’s disease—abnormalities in this barrier may block the entry of biomolecules essential to healthy brain activity. The BBB also makes it difficult for needed therapies to reach their target in the brain.
To help look for solutions to these and other problems, researchers can now grow human blood-brain barriers on a chip like the one pictured above. The high-magnification image reveals some of the BBB’s cellular parts. There are endothelial-like cells (magenta), which are similar to those that line the small vessels surrounding the brain. In close association are supportive brain cells known as astrocytes (green), which help to regulate blood flow.
While similar organ chips have been created before, what sets apart this new BBB chip is its use of induced pluripotent stem cell (iPSC) technology combined with advanced chip engineering. The iPSCs, derived in this case from blood samples, make it possible to produce a living model of anyone’s unique BBB on demand.
The researchers, led by Clive Svendsen, Cedars-Sinai, Los Angeles, first use a biochemical recipe to coax a person’s white blood cells to become iPSCs. At this point, the iPSCs are capable of producing any other cell type. But the Svendsen team follows two different recipes to direct those iPSCs to differentiate into endothelial and neural cells needed to model the BBB.
Also making this BBB platform unique is its use of a sophisticated microfluidic chip, produced by Boston-based Emulate, Inc. The chip mimics conditions inside the human body, allowing the blood-brain barrier to function much as it would in a person.
The channels enable researchers to flow cerebral spinal fluid (CSF) through one side and blood through the other to create the fully functional model tissue. The BBB chips also show electrical resistance and permeability just as would be expected in a person. The model BBBs are even able to block the entry of certain drugs!
As described in Cell Stem Cell, the researchers have already created BBB chips using iPSCs from a person with Huntington’s disease and another from an individual with a rare congenital disorder called Allan-Herndon-Dudley syndrome, an inherited disorder of brain development.
In the near term, his team has plans to model ALS and Parkinson’s disease on the BBB chips. Because these chips hold the promise of modeling the human BBB more precisely than animal models, they may accelerate studies of potentially promising new drugs. Svendsen suggests that individuals with neurological conditions might one day have their own BBB chips made on demand to help in selecting the best-available therapeutic options for them. Now that’s a future we’d all like to see.
Reference:
[1] Human iPSC-Derived Blood-Brain Barrier Chips Enable Disease Modeling and Personalized Medicine Applications. Vatine GD, Barrile R, Workman MJ, Sances S, Barriga BK, Rahnama M, Barthakur S, Kasendra M, Lucchesi C, Kerns J, Wen N, Spivia WR, Chen Z, Van Eyk J, Svendsen CN. Cell Stem Cell. 2019 Jun 6;24(6):995-1005.e6.
Links:
Tissue Chip for Drug Screening (National Center for Advancing Translational Sciences/NIH)
Stem Cell Information (NIH)
Svendsen Lab (Cedars-Sinai, Los Angeles)
NIH Support: National Institute of Neurological Disorders and Stroke; National Center for Advancing Translational Sciences
Snapshots of Life: The Brain’s Microscopic Green Trash Bins
Posted on by Dr. Francis Collins
Credit: Marina Venero Galanternik, Daniel Castranova, Tuyet Nguyen, and Brant M. Weinstein, NICHD, NIH
There are trash bins in our homes, on our streets, and even as a popular icon on our desktop computers. And as this colorful image shows, trash bins of the cellular variety are also important in the brain.
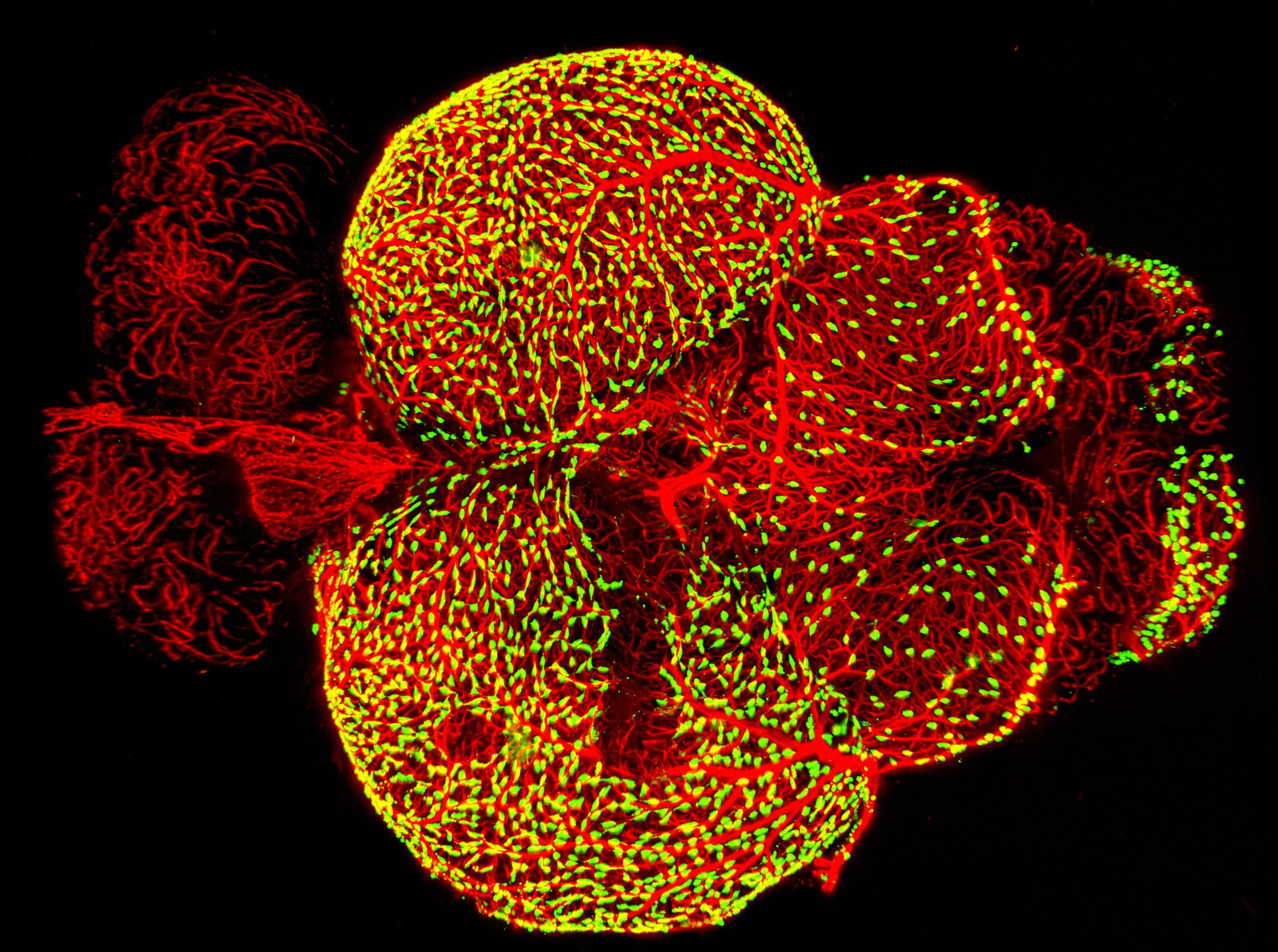
This image—a winner in the Federation of American Societies for Experimental Biology’s 2017 BioArt competition—shows the brain of an adult zebrafish, a popular organism for studying how the brain works. It captures dense networks of blood vessels (red) lining the outer surface of the brain. Next to many of these vessels sit previously little-studied cells called fluorescent granular perithelial cells (yellowish green). Researchers now believe these cells, often shortened to FGPs, act much like trash receptacles that continuously take in and store waste products to keep the brain tidy and functioning well.
Snapshots of Life: Development in Exquisite Detail
Posted on by Dr. Francis Collins
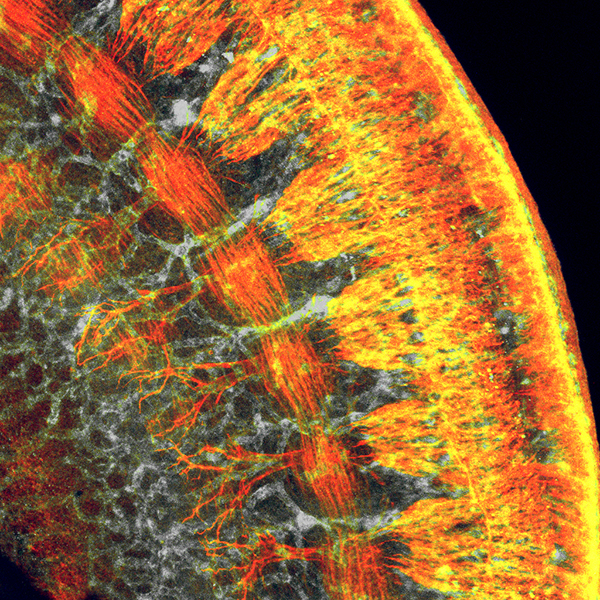
Credit: Shachi Bhatt and Paul Trainor, Stowers Institute for Medical Research, Kansas City, MO
If you’ve ever tried to take photos of wiggly kids, you know that it usually takes several attempts before you get the perfect shot. It’s often the same for biomedical researchers when taking images with microscopes because there are so many variables—from sample preparation to instrument calibration—to take into account. Still, there are always exceptions where everything comes together just right, and you are looking at one of them! On her first try at using a confocal microscope to image this cross-section of a mouse embryo’s torso, postdoc Shachi Bhatt captured a gem of an image that sheds new light on mammalian development.
Bhatt, who works in the NIH-supported lab of Paul Trainor at the Stowers Institute for Medical Research, Kansas City, MO, produced this micrograph as part of a quest to understand the striking parallels seen between the development of the nervous system and the vascular system in mammals. Fluorescent markers were used to label proteins uniquely expressed in each type of tissue: reddish-orange delineates developing nerve cells; gray highlights developing blood vessels; and yellow shows where the nerve cells and blood vessels overlap.
Snapshots of Life: Green Eggs and Heart Valves
Posted on by Dr. Francis Collins

Credit: Jessica Ryvlin, Stephanie Lindsey, and Jonathan Butcher, Cornell University, Ithaca, NY
What might appear in this picture to be an exotic, green glow worm served up on a collard leaf actually comes from something we all know well: an egg. It’s a 3-day-old chicken embryo that’s been carefully removed from its shell, placed in a special nutrient-rich bath to keep it alive, and then photographed through a customized stereo microscope. In the middle of the image, just above the blood vessels branching upward, you can see the outline of a transparent, developing eye. Directly to the left is the embryonic heart, which at this early stage is just a looped tube not yet with valves or pumping chambers.
Developing chicks are one of the most user-friendly models for studying normal and abnormal heart development. Human and chick hearts have a lot in common structurally, with four chambers and four valves pumping two circulations of blood in parallel. Unlike mammalian embryos tucked away in the womb, researchers have free range to study the chick heart in or out of the egg as it develops from a simple looped tube to a four-chambered organ.
Jonathan Butcher and his NIH-supported research group at Cornell University, Ithaca, NY, snapped this photo, a winner in the Federation of American Societies for Experimental Biology’s 2015 BioArt competition, to monitor differences in blood flow through the developing chick heart. You can get a sense of these differences by the varying intensities of green fluorescence in the blood vessels. The Butcher lab is interested in understanding how the force of the blood flow triggers the switching on and off of genes responsible for making functional heart valves. Although the four valves aren’t yet visible in this image, they will soon elongate into flap-like structures that open and close to begin regulating the normal flow of blood through the heart.
Creative Minds: Fighting Cancer with Supercomputers
Posted on by Dr. Francis Collins

Amanda Randles
After graduating college with degrees in physics and computer science, Amanda Randles landed her dream first job. She joined IBM in 2005 to work on its Blue Gene Project, which had just unveiled the world’s fastest supercomputer. So fast, in fact, it’s said that a scientist with a calculator would have to work nonstop for 177,000 years to perform the operations that Blue Gene could complete in one second. As a member of the applications team, Randles was charged with writing new code to make the next model run even faster.
Randles left IBM in 2009 for graduate school, with the goal to apply her supercomputing expertise to biomedical research. She spent the next several years developing the necessary algorithms to produce a high-resolution 3D model of the human cardiovascular system, complete with realistic blood flow. Now, an assistant professor at Duke University, Durham, NC, and a 2014 NIH Director’s Early Independence awardee, Randles will build on her earlier work to attempt something even more challenging: simulating the movement of cancer cells through the circulation to predict where a tumor is most likely to spread. Randles hopes all of her late nights writing code will one day lead to software that helps doctors stage cancer more precisely and gives patients accurate personalized computer simulations that put an earlier, potentially life-saving bullseye on secondary tumors.
Nanoparticles Target Damaged Blood Vessels
Posted on by Dr. Francis Collins

Caption: [A] Elastin stain (black) showing damaged elastic lamina in aorta. Inset (higher magnification) shows fluorescent nanoparticles attached to aorta where elastin is damaged. [B] Elastin stain showing aorta with undamaged elastic lamina. Inset shows no nanoparticle attachment. L stands for lumen, the open area inside the aorta.
Credit: Naren Vyavahare, Clemson University
Next Page