vaccines
Mapping Which Coronavirus Variants Will Resist Antibody Treatments
Posted on by Dr. Francis Collins

You may have heard about the new variants of SARS-CoV-2—the coronavirus that causes COVID-19—that have appeared in other parts of the world and have now been detected in the United States. These variants, particularly one called B.1.351 that was first identified in South Africa, have raised growing concerns about the extent to which their mutations might help them evade current antibody treatments and highly effective vaccines.
While researchers take a closer look, it’s already possible in the laboratory to predict which mutations will help SARS-CoV-2 evade our therapies and vaccines, and even to prepare for the emergence of new mutations before they occur. In fact, an NIH-funded study, which originally appeared as a bioRxiv pre-print in November and was recently peer-reviewed and published in Science, has done exactly that. In the study, researchers mapped all possible mutations that would allow SARS-CoV-2 to resist treatment with three different monoclonal antibodies developed for treatment of COVID-19 [1].
The work, led by Jesse Bloom, Allison Greaney, and Tyler Starr, Fred Hutchinson Cancer Center, Seattle, focused on the receptor binding domain (RBD), a key region of the spike protein that studs SARS-CoV-2’s outer surface. The virus uses RBD to anchor itself to the ACE2 receptor of human cells before infecting them. That makes the RBD a prime target for the antibodies that our bodies generate to defend against the virus.
In the new study, researchers used a method called deep mutational scanning to find out which mutations positively or negatively influence the RBD from being able to bind to ACE2 and/or thwart antibodies from striking their target. Here’s how it works: Rather than waiting for new mutations to arise, the researchers created a library of RBD fragments, each of which contained a change in a single nucleotide “letter” that would alter the spike protein’s shape and/or function by swapping one amino acid for another. It turns out that there are more than 3,800 such possible mutations, and Bloom’s team managed to make all but a handful of those versions of the RBD fragment.
The team then used a standard laboratory approach to measure systematically how each of those single-letter typos altered RBD’s ability to bind ACE2 and infect human cells. They also measured how those changes affected three different therapeutic antibodies from recognizing and binding to the viral RBD. Those antibodies include two developed by Regeneron (REGN10933 and REGN10987), which have been granted emergency use authorization for treatment of COVID-19 together as a cocktail called REGN-COV2. They also looked at an antibody developed by Eli Lilly (LY-CoV016), which is now in phase 3 clinical trials for treating COVID-19.
Based on the data, the researchers created four mutational maps for SARS-CoV-2 to escape each of the three therapeutic antibodies, as well as for the REGN-COV2 cocktail. Their studies show most of the mutations that would allow SARS-CoV-2 to escape treatment differed between the two Regeneron antibodies. That’s encouraging because it indicates that the virus likely needs more than one mutation to become resistant to the REGN-COV2 cocktail. However, it appears there’s one spot where a single mutation could allow the virus to resist REGN-COV2 treatment.
The escape map for LY-CoV016 similarly showed a number of mutations that could allow the virus to escape. Importantly, while some of those changes might impair the virus’s ability to cause infection, most of them appeared to come at little to no cost to the virus to reproduce.
How do these laboratory data relate to the real world? To begin to explore this question, the researchers teamed up with Jonathan Li, Brigham and Women’s Hospital, Boston. They looked at an immunocompromised patient who’d had COVID-19 for an unusually long time and who was treated with the Regeneron cocktail for 145 days, giving the virus time to replicate and acquire new mutations.
Viral genome data from the infected patient showed that these maps can indeed be used to predict likely paths of viral evolution. Over the course of the antibody treatment, SARS-CoV-2 showed changes in the frequency of five mutations that would change the makeup of the spike protein and its RBD. Based on the newly drawn escape maps, three of those five are expected to reduce the efficacy of REGN10933. One of the others is expected to limit binding by the other antibody, REGN10987.
The researchers also looked to data from all known circulating SARS-CoV-2 variants as of Jan. 11, 2021, for evidence of escape mutations. They found that a substantial number of mutations with potential to allow escape from antibody treatment already are present, particularly in parts of Europe and South Africa.
However, it’s important to note that these maps reflect just three important antibody treatments. Bloom says they’ll continue to produce maps for other promising therapeutic antibodies. They’ll also continue to explore where changes in the virus could allow for escape from the more diverse set of antibodies produced by our immune system after a COVID-19 infection or vaccination.
While it’s possible some COVID-19 vaccines may offer less protection against some of these new variants—and recent results have suggested the AstraZeneca vaccine may not provide much protection against the South African variant, there’s still enough protection in most other current vaccines to prevent serious illness, hospitalization, and death. And the best way to keep SARS-CoV-2 from finding new ways to escape our ongoing efforts to end this terrible pandemic is to double down on whatever we can do to prevent the virus from multiplying and spreading in the first place.
For now, emergence of these new variants should encourage all of us to take steps to slow the spread of SARS-CoV-2. That means following the three W’s: Wear a mask, Watch your distance, Wash your hands often. It also means rolling up our sleeves to get vaccinated as soon as the opportunity arises.
Reference:
[1] Prospective mapping of viral mutations that escape antibodies used to treat COVID-19.
Starr TN, Greaney AJ, Addetia A, Hannon WW, Choudhary MC, Dingens AS, Li JZ, Bloom JD.
Science. 2021 Jan 25:eabf9302.
Links:
COVID-19 Research (NIH)
Bloom Lab (Fred Hutchinson Cancer Center, Seattle)
NIH Support: National Institute of Allergy and Infectious Diseases
Following COVID-19 Vaccines Across the United States
Posted on by Dr. Francis Collins
Recently, there is a new and very hopeful COVID-19 number for everyone to track: the total number of vaccine doses that have been administered in the United States. If 80 percent of Americans roll up their sleeves in the coming months and accept COVID-19 vaccinations, we can greatly slow the spread of the novel coronavirus in our communities and bring this horrible pandemic to an end in 2021.
So far, more than 20 million people in our country have received one or two doses of either the Pfizer or Moderna vaccine. While this number is lower than initially projected for a variety of logistical reasons, we’re already seeing improvements in the distribution system that has made it possible to get close to 1 million doses administered per day.
If you want to keep track of the vaccine progress in your state over the coming weeks, it’s now pretty easy to do online. A fine resource is the vaccine information on the Centers for Disease Control and Prevention (CDC) COVID Data Tracker. It offers an interactive state-by-state map, as well as data on vaccinations in long-term care facilities. Keep in mind that there’s a delay of three to five days in reporting actual vaccinations from the states.
There’s also a lot of useful information on the Johns Hopkins Coronavirus Resource Center’s Vaccine Tracker. Posting the daily updates is a team, led by William Moss, that draws on the expertise of data scientists, analysts, programmers, and researchers. The Hopkins team gathers its vaccination data from each state’s official dashboard, webpages, press releases, or wherever cumulative numbers are reported. Not all states publish the same vaccine information, and that’s what can make the Vaccine Tracker so challenging to compile.
The Hopkins team now presents on its homepage the top 10 U. S. states and territories to vaccinate fully the highest percentage of their residents. With another click, there’s also a full rundown of vaccine administration by state and territory, plus the District of Columbia. The site also links to lots of other information about COVID-19—including cases, testing, contact tracing, and an interactive tool about vaccine development.
In uncertain times, knowledge can be a source of comfort. That’s what makes these interactive COVID-19 resources so helpful and empowering. They show that, with time, safe and effective COVID-19 vaccines will indeed coming to everyone. I hope that you will accept your vaccine, like I did when given the opportunity. However, until we get to the point where most Americans are immunized, we must stay vigilant and keep up our tried-and-true public health measures such as wearing masks, limiting physical interactions (especially indoors), and washing our hands.
Links:
COVID-19 Research (NIH)
CDC COVID Data Tracker (Centers for Disease Control and Prevention, Atlanta)
Coronavirus Resource Center (Johns Hopkins University School of Medicine)
William Moss (Johns Hopkins University, Baltimore)
International Vaccine Access Center (Johns Hopkins Bloomberg School of Public Health, Baltimore)
Celebrating the Gift of COVID-19 Vaccines
Posted on by Dr. Francis Collins

The winter holidays are traditionally a time of gift-giving. As fatiguing as 2020 and the COVID-19 pandemic have been, science has stepped up this year to provide humankind with a pair of truly hopeful gifts: the first two COVID-19 vaccines.
Two weeks ago, the U.S. Food and Drug Administration (FDA) granted emergency use authorization (EUA) to a COVID-19 vaccine from Pfizer/BioNTech, enabling distribution to begin to certain high-risk groups just three days later. More recently, the FDA granted an EUA to a COVID-19 vaccine from the biotechnology company Moderna, Cambridge, MA. This messenger RNA (mRNA) vaccine, which is part of a new approach to vaccination, was co-developed by NIH’s National Institute of Allergy and Infectious Diseases (NIAID). The EUA is based on data showing the vaccine is safe and 94.5 percent effective at protecting people from infection with SARS-CoV-2, the coronavirus that causes COVID-19.
Those data on the Moderna vaccine come from a clinical trial of 30,000 individuals, who generously participated to help others. We can’t thank those trial participants enough for this gift. The distribution of millions of Moderna vaccine doses is expected to begin this week.
It’s hard to put into words just how remarkable these accomplishments are in the history of science. A vaccine development process that used to take many years, often decades, has been condensed to about 11 months. Just last January, researchers started out with a previously unknown virus and we now have not just one, but two, vaccines that will be administered to millions of Americans before year’s end. And the accomplishments don’t end there—several other types of COVID-19 vaccines are also on the way.
It’s important to recognize that this couldn’t have happened without the efforts of many scientists working tirelessly behind the scenes for many years prior to the pandemic. Among those who deserve tremendous credit are Kizzmekia Corbett, Barney Graham, John Mascola, and other members of the amazing team at the Dale and Betty Bumpers Vaccine Research Center at NIH’s National Institute of Allergy and Infectious Diseases (NIAID).
When word of SARS-CoV-2 emerged, Corbett, Graham, and other NIAID researchers had already been studying other coronaviruses for years, including those responsible for earlier outbreaks of respiratory disease. So, when word came that this was a new coronavirus outbreak, they were ready to take action. It helped that they had paid special attention to the spike proteins on the surface of coronaviruses, which have turned out to be the main focus the COVID-19 vaccines now under development.
The two vaccines currently authorized for administration in the United States work in a unique way. Their centerpiece is a small, non-infectious snippet of mRNA. Our cells constantly produce thousands of mRNAs, which provide the instructions needed to make proteins. When someone receives an mRNA vaccine for COVID-19, it tells the person’s own cells to make the SARS-CoV-2 spike protein. The person’s immune system then recognizes the viral spike protein as foreign and produces antibodies to eliminate it.
This vaccine-spurred encounter trains the human immune system to remember the spike protein. So, if an actual SARS-CoV-2 virus tries to infect a vaccinated person weeks or months later, his or her immune system will be ready to fend it off. To produce the most vigorous and durable immunity against the virus, people will need to get two shots of mRNA vaccine, which are spaced several weeks to a month apart, depending on the vaccine.
Some have raised concerns on social media that mRNA vaccines might alter the DNA genome of someone being vaccinated. But that’s not possible, since this mRNA doesn’t enter the nucleus of the cell where DNA is located. Instead, the vaccine mRNAs stay in the outer part of the cell (the cytoplasm). What’s more, after being transcribed into protein just one time, the mRNA quickly degrades. Others have expressed concerns about whether the vaccine could cause COVID-19. That is not a risk because there’s no whole virus involved, just the coding instructions for the non-infectious spike protein.
An important advantage of mRNA is that it’s easy for researchers to synthesize once they know the nucleic acid sequence of a target viral protein. So, the gift of mRNA vaccines is one that will surely keep on giving. This new technology can now be used to speed the development of future vaccines. After the emergence of the disease-causing SARS, MERS, and now SARS-CoV-2 viruses, it would not be surprising if there are other coronavirus health threats in our future. Corbett and her colleagues are hoping to design a universal vaccine that can battle all of them. In addition, mRNA vaccines may prove effective for fighting future pandemics caused by other infectious agents and for preventing many other conditions, such as cancer and HIV.
Though vaccines are unquestionably our best hope for getting past the COVID-19 pandemic, public surveys indicate that some people are uneasy about accepting this disease-preventing gift. Some have even indicated they will refuse to take the vaccine. Healthy skepticism is a good thing, but decisions like this ought to be based on weighing the evidence of benefit versus risk. The results of the Pfizer and Moderna trials, all released for complete public scrutiny, indicate the potential benefits are high and the risks, low. Despite the impressive speed at which the new COVID-19 vaccines were developed, they have undergone and continue to undergo a rigorous process to generate all the data needed by the FDA to determine their long-term safety and effectiveness.
Unfortunately, the gift of COVID-19 vaccines comes too late for the more than 313,000 Americans who have died from complications of COVID-19, and many others who’ve had their lives disrupted and may have to contend with long-term health consequences related to COVID-19. The vaccines did arrive in record time, but all of us wish they could somehow have arrived even sooner to avert such widespread suffering and heartbreak.
It will be many months before all Americans who are willing to get a vaccine can be immunized. We need 75-80 percent of Americans to receive vaccines in order to attain the so-called “herd immunity” needed to drive SARS-CoV-2 away and allow us all to get back to a semblance of normal life.
Meanwhile, we all have a responsibility to do everything possible to block the ongoing transmission of this dangerous virus. Each of us needs to follow the three W’s: Wear a mask, Watch your distance, Wash your hands often.
When your chance for immunization comes, please roll up your sleeve and accept the potentially life-saving gift of a COVID-19 vaccine. In fact, I just got my first shot of the Moderna vaccine today along with NIAID Director Anthony Fauci, HHS Secretary Alex Azar, and some front-line healthcare workers at the NIH Clinical Center. Accepting this gift is our best chance to put this pandemic behind us, as we look forward to a better new year.
Links:
Coronavirus (COVID-19) (NIH)
Combat COVID (U.S. Department of Health and Human Services, Washington, D.C.)
Dale and Betty Bumpers Vaccine Research Center (National Institute of Allergy and Infectious Diseases/NIH)
Moderna (Cambridge, MA)
Pfizer (New York, NY)
BioNTech (Mainz, Germany)
Meet the Researcher Leading NIH’s COVID-19 Vaccine Development Efforts
Posted on by Dr. Francis Collins

A safe, effective vaccine is the ultimate tool needed to end the coronavirus disease 2019 (COVID-19) pandemic. Biomedical researchers are making progress every day towards such a vaccine, whether it’s devising innovative technologies or figuring out ways to speed human testing. In fact, just this week, NIH’s National Institute of Allergy and Infectious Diseases (NIAID) established a new clinical trials network that will enroll tens of thousands of volunteers in large-scale clinical trials testing a variety of investigational COVID-19 vaccines.
Among the vaccines moving rapidly through the development pipeline is one developed by NIAID’s Dale and Betty Bumpers Vaccine Research Center (VRC), in partnership with Moderna, Inc., Cambridge, MA. So, I couldn’t think of a better person to give us a quick overview of the COVID-19 vaccine research landscape than NIH’s Dr. John Mascola, who is Director of the VRC. Our recent conversation took place via videoconference, with John linking in from his home in Rockville, MD, and me from my place in nearby Chevy Chase. Here’s a condensed transcript of our chat:
Collins: Vaccines have been around since Edward Jenner and smallpox in the late 1700s. But how does a vaccine actually work to protect someone from infection?
Mascola: The immune system works by seeing something that’s foreign and then responding to it. Vaccines depend on the fact that if the immune system has seen a foreign protein or entity once, the second time the immune response will be much brisker. So, with these principles in mind, we vaccinate using part of a viral protein that the immune system will recognize as foreign. The response to this viral protein, or antigen, calls in specialized T and B cells, the so-called memory cells, and they remember the encounter. When you get exposed to the real thing, the immune system is already prepared. Its response is so rapid that you clear the virus before you get sick.
Collins: What are the steps involved in developing a vaccine?
Mascola: One can’t make a vaccine, generally speaking, without knowing something about the virus. We need to understand its surface proteins. We need to understand how the immune system sees the virus. Once that knowledge exists, we can make a candidate vaccine in the laboratory pretty quickly. We then transfer the vaccine to a manufacturing facility, called a pilot plant, that makes clinical grade material for testing. When enough testable material is available, we do a first-in-human study, often at our vaccine clinic at the NIH Clinical Center.
If those tests look promising, the next big step is finding a pharmaceutical partner to make the vaccine at large scale, seek regulatory approval, and distribute it commercially. That usually takes a while. So, from start to finish, the process often takes five or more years.
Collins: With this global crisis, we obviously don’t have five years to wait. Tell us about what the VRC started to do as soon as you learned about the outbreak in Wuhan, China.
Mascola: Sure. It’s a fascinating story. We had been talking with NIAID Director Dr. Anthony Fauci and our colleagues about how to prepare for the next pandemic. Pretty high on our list were coronaviruses, having already worked on past outbreaks of SARS and MERS [other respiratory diseases caused by coronaviruses]. So, we studied coronaviruses and focused on the unique spike protein crowning their surfaces. We designed a vaccine that presented the spike protein to the immune system.
Collins: Knowing that the spike protein was likely your antigen, what was your approach to designing the vaccine?
Mascola: Our approach was a nucleic acid-based vaccine. I’m referring to vaccines that are based on genetic material, either DNA or RNA. It’s this type of vaccine that can be moved most rapidly into the clinic for initial testing.
When we learned of the outbreak in Wuhan, we simply accessed the nucleic acid sequence of SARS-CoV-2, the novel coronavirus that causes COVID-19. Most of the sequence was on a server from Chinese investigators. We looked at the spike sequence and built that into an RNA vaccine. This is called in silico vaccine design. Because of our experience with the original SARS back in the 2000s, we knew its sequence and we knew this approach worked. We simply modified the vaccine design to the sequence of the spike protein of SARS-CoV-2. Literally within days, we started making the vaccine in the lab.
At the same time, we worked with a biotechnology company called Moderna that creates personalized cancer vaccines. From the time the sequence was made available in early January to the start of the first in-human study, it was about 65 days.
Collins: Wow! Has there ever been a vaccine developed in 65 days?
Mascola: I don’t think so. There are a lot of firsts with COVID, and vaccine development is one of them.
Collins: For the volunteers who enrolled in the phase 1 study, what was actually in the syringe?
Mascola: The syringe included messenger RNA (mRNA), the encoded instructions for making a specific protein, in this case the spike protein. The mRNA is formulated in a lipid nanoparticle shell. The reason is mRNA is less stable than DNA, and it doesn’t like to hang around in a test tube where enzymes can break it down. But if one formulates it just right into a nanoparticle, the mRNA is protected. Furthermore, that protective particle allows one to inject it into muscle and facilitates the uptake of the mRNA into the muscle cells. The cells translate the mRNA into spike proteins, and the immune system sees them and mounts a response.
Collins: Do muscle cells know how to take that protein and put it on their cell surfaces, where the immune system can see it?
Mascola: They do if the mRNA is engineered just the right way. We’ve been doing this with DNA for a long time. With mRNA, the advantage is that it just has to get into the cell [not into the nucleus of the cell as it does for DNA]. But it took about a decade of work to figure out how to do nucleotide silencing, which allows the cell to see the mRNA, not destroy it, and actually treat it as a normal piece of mRNA to translate into protein. Once that was figured out, it becomes pretty easy to make any specific vaccine.
Collins: That’s really an amazing part of the science. While it seems like this all happened in a blink of an eye, 65 days, it was built on years of basic science work to understand how cells treat mRNA. What’s the status of the vaccine right now?
Mascola: Early data from the phase 1 study are very encouraging. There’s a manuscript in preparation that should be out shortly showing that the vaccine was safe. It induced a very robust immune response to that spike protein. In particular, we looked for neutralizing antibodies, which are the ones that attach to the spike, blocking the virus from binding to a cell. There’s a general principle in vaccine development: if the immune system generates neutralizing antibodies, that’s a very good sign.
Collins: You’d be the first to say that you’re not done yet. Even though those are good signs, that doesn’t prove that this vaccine will work. What else do you need to know?
Mascola: The only real way to learn if a vaccine works is to test it in people. We break clinical studies into phases 1, 2, and 3. Phase 1 has already been done to evaluate safety. Phase 2 is a larger evaluation of safety and immune response. That’s ongoing and has enrolled 500 or 600 people, which is good. The plan for the phase 3 study will be to start in July. Again, that’s incredibly fast, considering that we didn’t even know this virus existed until January.
Collins: How many people do you need to study in a phase 3 trial?
Mascola: We’re thinking 20,000 or 30,000.
Collins: And half get the vaccine and half get a placebo?
Mascola: Sometimes it can be done differently, but the classic approach is half placebo, half vaccine.
Collins: We’ve been talking about the VRC-Moderna nucleic acid vaccine. But there are others that are coming along pretty quickly. What other strategies are being employed, and what are their timetables?
Mascola: There are many dozens of vaccines under development. The response has been extraordinary by academic groups, biotech companies, pharmaceutical companies, and NIH’s Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) partnership. I don’t think I’ve ever seen so much activity in a vaccine space moving ahead at such a rapid clip.
As far as being ready for advanced clinical trials, there are a just handful and they involve different types of vaccines. At least three nucleic acid vaccines are in clinical trials. There are also two vaccines that use proteins, which is a more classic approach.
In addition, there are several vaccines based on a viral vector. To make these, one puts the genes for the spike protein inside an adenovirus, which is an innocuous cold virus, and injects it into muscle. In regard to phase 3 trials, there are maybe three or four vaccines that could be formally in such tests by the fall.
Collins: How is it possible to do this so much more rapidly than in the past, without imposing risks?
Mascola: It’s a really important question, Francis. A number of things are being done in parallel, and that wouldn’t usually be the case. We can get a vaccine into a first-in-human study much more quickly because of time-saving technologies.
But the real important point is that for the phase 3 trial, there are no timesavers. One must enroll 30,000 people and watch them over months in a very rigorous, placebo-controlled environment. The NIH has stood up what’s called a Data Safety Monitoring Board for all the trials. That’s an independent group of investigators that will review all vaccine trial data periodically. They can see what the data are showing: Should the trial be stopped early because the vaccine is working? Is there a safety signal that raises concern?
While the phase 3 trial is going on, the U.S. government also will be funding large-scale manufacture of the vaccine. Traditionally, you would do the vaccine trial, wait until it’s all done, and analyze the data. If it worked, you’d build a vaccine plant to make enough material, which takes two or three years, and then go to the Food and Drug Administration (FDA) for regulatory approval.
Everything here is being done in parallel. So, if the vaccine works, it’s already in supply. And we have been engaging the FDA to get real-time feedback. That does save a lot of time.
Collins: Is it possible that we’ll manufacture a whole lot of doses that may have to be thrown out if the vaccine doesn’t work?
Mascola: It certainly is possible. One would like to think that for coronaviruses, vaccines are likely to work, in part because the natural immune response clears them. People get quite sick, but eventually the immune system clears the virus. So, if we can prime it with a vaccine, there is reason to believe vaccines should work.
Collins: If the vaccine does work, will this be for lifelong prevention of COVID-19? Or will this be like the flu, where the virus keeps changing and new versions of the vaccine are needed every year?
Mascola: From what we know about coronaviruses, we think it’s likely COVID-19 is not like the flu. Coronaviruses do have some mutation rate, but the data suggest it’s not as rapid as influenza. If we’re fortunate, the vaccine won’t need to be changed. Still, there’s the matter of whether the immunity lasts for a year, five years, or 10 years. That we don’t know without more data.
Collins: Do we know for sure that somebody who has had COVID-19 can’t get it again a few months later?
Mascola: We don’t know yet. To get the answer, we must do natural history studies, where we follow people who’ve been infected and see if their risk of getting the infection is much lower. Although classically in virology, if your immune system shows neutralizing antibodies to a virus, it’s very likely you have some level of immunity.
What’s a bit tricky is there are people who get very mild symptoms of COVID-19. Does that mean their immune system only saw a little bit of the viral antigen and didn’t respond very robustly? We’re not sure that everyone who gets an infection is equally protected. That’s going to require a natural history study, which will take about a year of follow-up to get the answers.
Collins: Let’s go back to trials that need to happen this summer. You talked about 20,000 to 30,000 people needing to volunteer just for one vaccine. Whom do you want to volunteer?
Mascola: The idea with a phase 3 trial is to have a broad spectrum of participation. To conduct a trial of 30,000 people is an enormous logistical operation, but it has been done for the rotavirus and HPV vaccines. When you get to phase 3, you don’t want to enroll just healthy adults. You want to enroll people who are representative of the diverse population that you want to protect.
Collins: Do you want to enrich for high-risk populations? They’re the ones for whom we hope the vaccine will provide greatest benefit: for example, older people with chronic illnesses, African Americans, and Hispanics.
Mascola: Absolutely. We want to make sure that we can feel comfortable to recommend the vaccine to at-risk populations.
Collins: Some people have floated another possibility. They ask why do we need expensive, long-term clinical trials with tens of thousands of people? Couldn’t we do a human challenge trial in which we give the vaccine to some healthy, young volunteers, wait a couple of weeks, and then intentionally expose them to SARS-CoV-2. If they don’t get sick, we’re done. Are challenge studies a good idea for COVID-19?
Mascola: Not right now. First, one has to make a challenge stock of the SARS-CoV-2 that’s not too pathogenic. We don’t want to make something in the lab that causes people to get severe pneumonia. Also, for challenge studies, it would be preferable to have a very effective small drug or antibody treatment on hand. If someone were to get sick, you could take care of the infection pretty readily with the treatments. We don’t have curative treatments, so the current thinking is we’re not there yet for COVID-19 challenge studies [1]. If you look at our accelerated timeline, formal vaccine trials still may be the fastest and safest way to get the answers.
Collins: I’m glad you’re doing it the other way, John. It’s going to take a lot of effort. You’re going to have to go somewhere where there is still ongoing spread, otherwise you won’t know if the vaccine works or not. That’s going to be tricky.
Mascola: Yes. How do we know where to test the vaccine? We are using predictive analytics, which is just a fancy way of saying that we are trying to predict where in the country there will be ongoing transmission. If we can get really good at it, we’ll have real-time data to say transmission is ongoing in a certain area. We can vaccinate in that community, while also possibly protecting people most at risk.
Collins: John, this conversation has been really informative. What’s your most optimistic view about when we might have a COVID-19 vaccine that’s safe and effective enough to distribute to the public?
Mascola: An optimistic scenario would be that we get an answer in the phase 3 trial towards the end of this year. We have scaled up the production in parallel, so the vaccine should be available in great supply. We still must allow for the FDA to review the data and be comfortable with licensing the vaccine. Then we must factor in a little time for distributing and recommending that people get the vaccine.
Collins: Well, it’s wonderful to have someone with your skills, experience, and vision taking such a leading role, along with your many colleagues at the Vaccine Research Center. People like Kizzmekia Corbett, Barney Graham, and all the others who are a part of this amazing team that you’ve put together, overseen by Dr. Fauci.
While there is still a ways to go, we can take pride in how far we have come since this virus emerged just about six months ago. In my 27 years at NIH, I’ve never seen anything quite like this. There’s been a willingness among people to set aside all kinds of other concerns. They’ve gathered around the same table, worked on vaccine design and implementation, and gotten out there in the real world to launch clinical trials.
John, thank you for what you are doing 24/7 to make this kind of progress possible. We’re all watching, hoping, and praying that this will turn out to be the answer that people desperately need after such a terribly difficult time so far in 2020. I believe 2021 will be a very different kind of experience, largely because of the vaccine science that we’ve been talking about today.
Mascola: Thank you so much, Francis. And thanks for recognizing all the people behind the scenes who are making this happen. They’re working really hard!
Reference:
[1] Accelerating Development of SARS-CoV-2 Vaccines—The Role for Controlled Human Infection Models. Deming ME, Michael, NL, Robb M, Cohen MS, Neuzil KM. N Engl J Med. 2020 July 1. [Epub ahead of print].
Links:
Coronavirus (COVID-19) (NIH)
John R. Mascola (National Institute of Allergy and Infectious Diseases/NIH)
Novel Vaccine Technologies for the 21st Century. Mascola JR, Fauci AS. Nat Rev Immunol. 2020 Feb;20(2):87-88.
Vaccine Research Center (NIAID/NIH)
Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV)
How to Make Biopharmaceuticals Quickly in Small Batches
Posted on by Dr. Francis Collins

Caption: InSCyT system. Image shows (1) production module, (2) purification module, and (3) formulation module.
Credit: Felice Frankel Daniloff, Massachusetts Institute of Technology, Cambridge
Today, vaccines and other protein-based biologic drugs are typically made in large, dedicated manufacturing facilities. But that doesn’t always fit the need, and it could one day change. A team of researchers has engineered a miniaturized biopharmaceutical “factory” that could fit on a dining room table and produce hundreds to thousands of doses of a needed treatment in about three days.
As published recently in the journal Nature Biotechnology, this on-demand manufacturing system is called Integrated Scalable Cyto-Technology (InSCyT). It is fully automated and can be readily reconfigured to produce virtually any approved or experimental vaccine, hormone, replacement enzyme, antibody, or other biopharmaceutical. With further improvements and testing, InSCyT promises to give researchers and health care providers easy access to specialty biologics needed to treat rare diseases, as well as treatments for combating infectious disease outbreaks in remote towns or villages around the globe.
Autism Spectrum Disorder: Progress Toward Earlier Diagnosis
Posted on by Dr. Francis Collins

Stockbyte
Research shows that the roots of autism spectrum disorder (ASD) generally start early—most likely in the womb. That’s one more reason, on top of a large number of epidemiological studies, why current claims about the role of vaccines in causing autism can’t be right. But how early is ASD detectable? It’s a critical question, since early intervention has been shown to help limit the effects of autism. The problem is there’s currently no reliable way to detect ASD until around 18–24 months, when the social deficits and repetitive behaviors associated with the condition begin to appear.
Several months ago, an NIH-funded team offered promising evidence that it may be possible to detect ASD in high-risk 1-year-olds by shifting attention from how kids act to how their brains have grown [1]. Now, new evidence from that same team suggests that neurological signs of ASD might be detectable even earlier.
Snapshots of Life: Portrait of Zika Virus
Posted on by Dr. Francis Collins
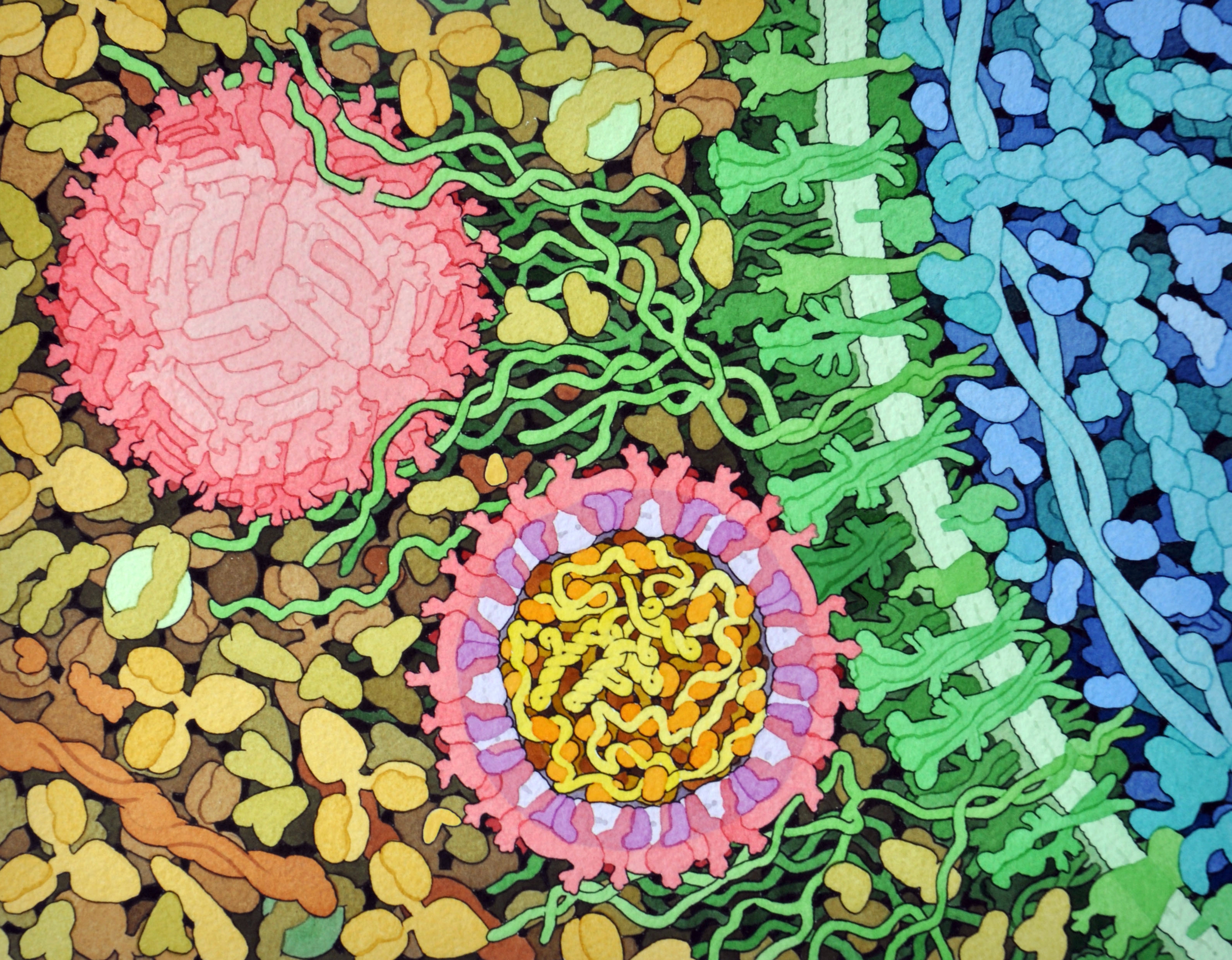
Credit: David Goodsell, The Scripps Research Institute
This lively interplay of shape and color is an artistic rendering of the Zika virus preparing to enter a cell (blue) by binding to its protein receptors (green). The spherical structures (pink) represent two Zika viruses in a blood vessel filled with blood plasma cells (tan). The virus in the middle in cross section shows viral envelope proteins (red) studding the outer surface, with membrane proteins (pink) embedded in a fatty layer of lipids (light purples). In the innermost circle, you can see the viral genome (yellow) coiled around capsid proteins (orange).
This image was sketched and hand-painted with watercolors by David Goodsell, a researcher and illustrator at The Scripps Research Institute, La Jolla, CA. Goodsell put paint and science to paper as part of the “Molecule of the Month” series run by RCSB Protein Data Bank (PDB), which NIH co-supports with the National Science Foundation and the Department of Energy. The PDB, which contains structural data on thousands of proteins and small molecules, uses its “Molecule of the Month” series to help students visualize a molecule or virus and to encourage their exploration of structural biology and its applications to medicine.
Resurgence of Measles, Pertussis Fueled by Vaccine Refusals
Posted on by Dr. Francis Collins

Credit: Centers for Disease Control and Prevention
I was born in 1950 and was home-schooled until the 6th grade. Thus, I missed exposure to several childhood illnesses that affected most of my generation. I never gave it much thought until, as a medical resident in North Carolina in 1979, I came down with a potentially life-threatening febrile illness that required hospitalization. Only after four days of 105 degree fever did a rash appear, and the diagnosis was made: measles. That was the sickest I have ever been. It turned out that one of my daughter’s school friends had developed measles in a small outbreak of unvaccinated kids in Chapel Hill, and I had been exposed to her. I was born too early to have been vaccinated.
But for most people born in the United States after the 1960s, they have never had to experience the high fever and rash of the measles or the coughing fits of pertussis, commonly known as whooping cough. That’s because these extremely contagious and potentially life-threatening diseases have been controlled with the use of highly effective vaccines and strong vaccination programs. And yet, the number of Americans sickened with measles and pertussis each year has recently crept back up.
Now, an NIH-funded report confirms that many of the recent outbreaks of these vaccine-preventable diseases have been fueled by refusal by some parents to have their children vaccinated [1]. The findings, published recently in JAMA, come as an important reminder that successful eradication of infectious diseases depends not only on the availability of safe and effective vaccines, but also on effective communication about the vaccines and the diseases they prevent.
Vaccine Research: New Tactics for Tackling HIV
Posted on by Dr. Francis Collins

Caption: Scanning electron micrograph of an HIV-infected immune cell.
Credit: National Institute of Allergy and Infectious Diseases, NIH
For many of the viruses that make people sick—think measles, smallpox, or polio—vaccines that deliver weakened or killed virus encourage the immune system to produce antibodies that afford near complete protection in the event of an exposure. But that simple and straightforward approach doesn’t work in the case of human immunodeficiency virus (HIV), the virus that causes AIDS. In part, that’s because our immune system is poorly equipped to recognize HIV and mount an attack against the infection. To make matters worse, HIV has a habit of quickly mutating as it multiplies.That means, in order for an HIV vaccine to be effective, it must induce antibodies capable of fighting against a wide range of HIV strains. For all these reasons, the three decades of effort to develop an HIV vaccine have turned out to be enormously challenging and frustrating.
But now I’m pleased to report that NIH-funded scientists have taken some encouraging strides down this path. In two papers published in Science [1, 2] and one in Cell [3], researchers presented results of animal studies that support what most vaccine experts have come to suspect: the immune system is in fact capable of producing the kind of antibodies that should be protective against HIV, but it takes more than one step to get there. In effect, a successful vaccine strategy has to “take the immune system to school,” and it requires more than one lesson to pass the final exam. Specifically, what’s needed seems to be a series of shots—each consisting of a different engineered protein designed to push the immune system, step by step, toward the production of protective antibodies that will work against virtually all HIV strains.
NIH Ebola Update: Working Toward Treatments and Vaccines
Posted on by Drs. Anthony S. Fauci and Francis S. Collins

Credit: National Institutes of Health
Updated Oct. 22, 2014: The National Institutes of Health (NIH) today announced the start of human clinical trials of a second Ebola vaccine candidate at the NIH Clinical Center in Bethesda, MD. In this early phase trial, researchers from NIH’s National Institute of Allergy and Infectious Diseases (NIAID) are evaluating the vaccine, called VSV-ZEBOV, for its safety and ability to generate an immune response in healthy adults who receive two intramuscular doses, called a prime-boost strategy.
The Walter Reed Army Institute of Research is simultaneously testing the vaccine candidate as a single dose at its Clinical Trials Center in Silver Spring, MD. VSV-ZEBOV, which was developed by researchers at the Public Health Agency of Canada’s National Microbiology Laboratory, has been licensed to NewLink Genetics Corp. through its wholly owned subsidiary BioProtection Systems, both based in Ames, Iowa.
Early human testing of another Ebola vaccine candidate, co-developed by NIAID and GlaxoSmithKline, began in early September at the NIH Clinical Center. Initial data on that vaccine’s safety and ability to generate an immune response are expected by the end of 2014.
![]()
We are all alarmed by the scope and scale of the human tragedy occurring in West African nations affected by the Ebola virus disease epidemic. While the cornerstones of the Ebola response remain prompt diagnosis and isolation of patients, tracing of contacts, and proper protective equipment for healthcare workers, the National Institutes of Health (NIH), led by its National Institute of Allergy and Infectious Diseases (NIAID), is spearheading efforts to develop treatments and a vaccine for Ebola as quickly as possible.
For example, NIAID has supported and collaborated with Mapp Biopharmaceutical, Inc., San Diego, in its development of the product known as ZMapp, which has been administered experimentally to several Ebola-infected patients. While it is not possible at this time to determine whether ZMapp benefited these patients, NIAID is supporting a broader effort to advance development and clinical testing of ZMapp to determine if it is safe and effective. In addition, the U.S. Biodefense Advanced Research and Development Agency (BARDA) has announced plans to optimize and accelerate the manufacturing of ZMapp, which is in limited supply, to enable clinical safety testing to proceed as soon as possible.
Previous Page Next Page