clinical trial
Early Data Suggest Pfizer Pill May Prevent Severe COVID-19
Posted on by Dr. Francis Collins
Over the course of this pandemic, significant progress has been made in treating COVID-19 and helping to save lives. That progress includes the development of life-preserving monoclonal antibody infusions and repurposing existing drugs, to which NIH’s Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) public-private partnership has made a major contribution.
But for many months we’ve had hopes that a safe and effective oral medicine could be developed that would reduce the risk of severe illness for individuals just diagnosed with COVID-19. The first indication that those hopes might be realized came from the announcement just a month ago of a 50 percent reduction in hospitalizations from the Merck and Ridgeback drug molnupiravir (originally developed with an NIH grant to Emory University, Atlanta). Now comes word of a second drug with potentially even higher efficacy: an antiviral pill from Pfizer Inc. that targets a different step in the life cycle of SARS-CoV-2, the novel coronavirus that causes COVID-19.
The most recent exciting news started to roll out earlier this month when a Pfizer research team published in the journal Science some promising initial data involving the antiviral pill and its active compound [1]. Then came even bigger news a few days later when Pfizer announced interim results from a large phase 2/3 clinical trial. It found that, when taken within three days of developing symptoms of COVID-19, the pill reduced by 89 percent the risk of hospitalization or death in adults at high risk of progressing to severe illness [2].
At the recommendation of the clinical trial’s independent data monitoring committee and in consultation with the U.S. Food and Drug Administration (FDA), Pfizer has now halted the study based on the strength of the interim findings. Pfizer plans to submit the data to the FDA for Emergency Use Authorization (EUA) very soon.
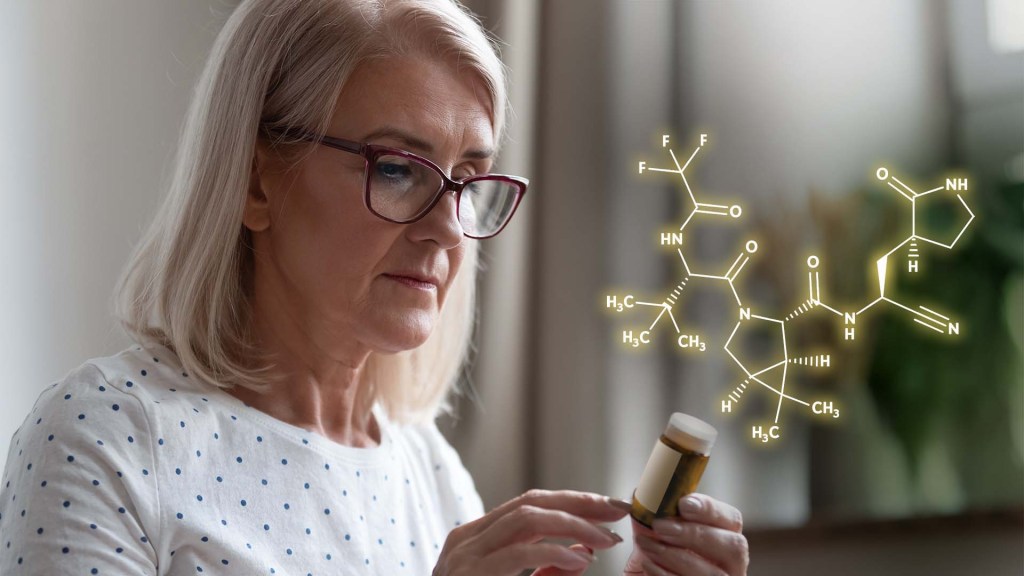
Pfizer’s antiviral pill is a protease inhibitor, originally called PF-07321332, or just 332 for short. A protease is an enzyme that cleaves a protein at a specific series of amino acids. The SARS-CoV-2 virus encodes its own protease to help process a large virally-encoded polyprotein into smaller segments that it needs for its life cycle; a protease inhibitor drug can stop that from happening. If the term protease inhibitor rings a bell, that’s because drugs that work in this way already are in use to treat other viruses, including human immunodeficiency virus (HIV) and hepatitis C virus.
In the case of 332, it targets a protease called Mpro, also called the 3CL protease, coded for by SARS-CoV-2. The virus uses this enzyme to snip some longer viral proteins into shorter segments for use in replication. With Mpro out of action, the coronavirus can’t make more of itself to infect other cells.
What’s nice about this therapeutic approach is that mutations to SARS-CoV-2’s surface structures, such as the spike protein, should not affect a protease inhibitor’s effectiveness. The drug targets a highly conserved, but essential, viral enzyme. In fact, Pfizer originally synthesized and pre-clinically evaluated protease inhibitors years ago as a potential treatment for severe acute respiratory syndrome (SARS), which is caused by a coronavirus closely related to SARS-CoV-2. This drug might even have efficacy against other coronaviruses that cause the common cold.
In the study published earlier this month in Science [1], the Pfizer team led by Dafydd Owen, Pfizer Worldwide Research, Cambridge, MA, reported that the latest version of their Mpro inhibitor showed potent antiviral activity in laboratory tests against not just SARS-CoV-2, but all of the coronaviruses they tested that are known to infect people. Further study in human cells and mouse models of SARS-CoV-2 infection suggested that the treatment might work to limit infection and reduce damage to lung tissue.
In the paper in Science, Owen and colleagues also reported the results of a phase 1 clinical trial with six healthy people. They found that their protease inhibitor, when taken orally, was safe and could reach concentrations in the bloodstream that should be sufficient to help combat the virus.
But would it work to treat COVID-19 in an infected person? So far, the preliminary results from the larger clinical trial of the drug candidate, now known as PAXLOVID™, certainly look encouraging. PAXLOVID™ is a formulation that combines the new protease inhibitor with a low dose of an existing drug called ritonavir, which slows the metabolism of some protease inhibitors and thereby keeps them active in the body for longer periods of time.
The phase 2/3 clinical trial included about 1,200 adults from the United States and around the world who had enrolled in the clinical trial. To be eligible, study participants had to have a confirmed diagnosis of COVID-19 within a five-day period along with mild-to-moderate symptoms of illness. They also required at least one characteristic or condition associated with an increased risk for developing severe illness from COVID-19. Each individual in the study was randomly selected to receive either the experimental antiviral or a placebo every 12 hours for five days.
In people treated within three days of developing COVID-19 symptoms, the Pfizer announcement reports that 0.8 percent (3 of 389) of those who received PAXLOVID™ were hospitalized within 28 days compared to 7 percent (27 of 385) of those who got the placebo. Similarly encouraging results were observed in those who got the treatment within five days of developing symptoms. One percent (6 of 607) on the antiviral were hospitalized versus 6.7 percent (41 of 612) in the placebo group. Overall, there were no deaths among people taking PAXLOVID™; 10 people in the placebo group (1.6 percent) subsequently died.
If all goes well with the FDA review, the hope is that PAXLOVID™ could be prescribed as an at-home treatment to prevent severe illness, hospitalization, and deaths. Pfizer also has launched two additional trials of the same drug candidate: one in people with COVID-19 who are at standard risk for developing severe illness and another evaluating its ability to prevent infection in adults exposed to the coronavirus by a household member.
Meanwhile, Britain recently approved the other recently developed antiviral molnupiravir, which slows viral replication in a different way by blocking its ability to copy its RNA genome accurately. The FDA will meet on November 30 to discuss Merck and Ridgeback’s request for an EUA for molnupiravir to treat mild-to-moderate COVID-19 in infected adults at high risk for severe illness [3]. With Thanksgiving and the winter holidays fast approaching, these two promising antiviral drugs are certainly more reasons to be grateful this year.
References:
[1] An oral SARS-CoV-2 M(pro) inhibitor clinical candidate for the treatment of COVID-19.
Owen DR, Allerton CMN, Anderson AS, Wei L, Yang Q, Zhu Y, et al. Science. 2021 Nov 2: eabl4784.
[2] Pfizer’s novel COVID-19 oral antiviral treatment candidate reduced risk of hospitalization or death by 89% in interim analysis of phase 2/3 EPIC-HR Study. Pfizer. November 5, 2021.
[3] FDA to hold advisory committee meeting to Discuss Merck and Ridgeback’s EUA Application for COVID-19 oral treatment. Food and Drug Administration. October 14, 2021.
Links:
COVID-19 Research (NIH)
Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) (NIH)
A Study of PF-07321332/Ritonavir in Nonhospitalized Low-Risk Adult Participants With COVID-19 (ClinicalTrials.gov)
A Post-Exposure Prophylaxis Study of PF-07321332/Ritonavir in Adult Household Contacts of an Individual With Symptomatic COVID-19 (ClinicalTrials.gov)
Lessons Learned About Substance Use Disorders During the COVID-19 Pandemic
Posted on by Dr. Francis Collins

Every spring, I and my colleague Dr. Nora Volkow, Director of NIH’s National Institute on Drug Abuse (NIDA), join with leaders across the country in the Rx Drug Abuse and Heroin Summit. Our role is to discuss NIH’s continued progress in tackling our nation’s opioid crisis. Because of the continued threat of COVID-19 pandemic, we joined in virtually for the second year in a row.
While the demands of the pandemic have been challenging for everyone, biomedical researchers have remained hard at work to address the opioid crisis. Among the many ways that NIH is supporting these efforts is through its Helping to End Addiction Long-Term (HEAL) Initiative, which is directing more than $1.5 billion to researchers and communities across the country.
Here’s a condensed transcript of our April 6th video dialogue, which focused on the impact of the COVID-19 pandemic on people struggling with substance use disorders and those who are trying to help them.

Collins: What have we learned so far through HEAL? Well, one thing HEAL is doing is tackling the need for pain treatments that help people avoid the risks of opioids. This research has uncovered new targets and therapeutics for different types of pain, including neuropathic, post-surgical, osteoarthritic, and chemotherapy induced. We’re testing implanted devices, such as electrodes and non-invasive nerve stimulation; and looking at complementary and integrative approaches, such as phone-based physical therapy for low back pain.
Through HEAL, we’ve launched a first-in-human test of a vaccine to protect against the harmful effects of opioids, including relapse and overdose. We’re also testing a tool that provides pharmacists with a validated opioid use disorder risk measure. The goal is to identify better who’s at high risk for opioid addiction and to determine what kind of early intervention could be put in place.
Despite COVID, many clinical studies are now recruiting participants. This includes family-based prevention programs, culturally tailored interventions for hard-hit American Indian populations, and interventions that address social inequities, such as lack of housing.
We are also making progress on the truly heart-breaking problem of babies born dependent on opioids. HEAL has launched a study to test the effectiveness of a new approach to care that measures the severity of a baby’s withdrawal, based on their ability to eat, sleep, and be consoled. This approach helps provide appropriate treatment for these infants, without the use of medication when possible. We’re also developing novel technologies to help treat neonatal opioid withdrawal syndrome, including a gently vibrating hospital bassinet pad that’s received breakthrough device designation from the FDA.
2020 was an extraordinary year that was tragic in so many ways, including lives lost and economic disasters that have fallen upon families. The resilience and ingenuity of the scientific community has been impressive. Quick pivoting has resulted in some gains through research, maybe you could even call them silver linings in the midst of this terrible storm.
Nora, what’s been at the forefront of your mind as we’ve watched things unfold?
Volkow: When we did this one year ago, we didn’t know what to expect. Obviously, we were concerned that the stressors associated with a pandemic, with unknowns, are factors that have been recognized for many years to increase drug use. Unfortunately, what we’ve seen is an increase in drug use of all types across the country.
We have seen an exacerbation of the opioid epidemic, as evidenced by the number of people who have died. Already, in the 12 months ending in July 2020, there was a 24 percent increase in mortality from overdoses. Within those numbers, there was close to a 50 percent increase in mortality associated with fentanyl. We’re also seeing an increase, not just in deaths from fentanyl and other synthetic opioids, but in deaths from stimulant drugs, like cocaine and methamphetamine. And the largest increases have been very much driven by drug combinations.
So, we have the perfect storm. We have people stressed to their limits by decreases in the economy, the loss of jobs, the death of loved ones. On the other hand, we see dealers taking the opportunity to bring in drugs such as synthetic opioids and synthetic stimulants and distribute them to a much wider extent than previously seen.

Collins: On top of that, people are at risk of getting sick from COVID-19. What have we learned about the risks of coronavirus illness for people who use drugs?
Volkow: It is a double whammy. When you look at the electronic health records about the outcomes of people diagnosed with substance use disorders, you consistently see an increased risk for getting infected with COVID-19. And if you look at those who get infected, you observe a significantly increased risk of dying from COVID.
What’s driving this vulnerability? One factor is the pharmacological effects of these drugs. Basically, all of the drugs of abuse that result in addiction, notably opioids, damage the cardiopulmonary system. Some also damage the immune system. And we know that individuals who have any disruption of cardiovascular health, pulmonary health, immune function, or metabolism are at higher risk of getting infected with COVID-19 and having adverse outcomes.
But there’s another factor that’s as important—one that’s very tractable. It is the way in which our society has dealt with substance use disorders: not actually treating them as a disease that requires intervention and support for recovery. The stigmatization of individuals with addiction, the lack of access to treatment, the social isolation, have all created havoc by making these individuals so much more vulnerable to get infected with COVID-19.
They will not go to a doctor. They don’t want to be stigmatized. They need to go out into the streets to get access to the drugs. Many times, they don’t have a choice of what drugs to take because they cannot afford anything except what’s offered to them. So, many, especially those who are minorities, end up homeless or in jails or prison. Even before COVID, we knew that prisons and jails are places where infections can transmit extraordinary rapidly. You could see this was going to result in very negative outcomes for this group of individuals.
Collins: Nora, tell us more about the trends contributing to the current crisis. Maybe three or four years ago, what was going straight up was opioid use, especially heroin. Then, fentanyl started coming up very fast and that has continued. Now, we are seeing more stimulants and mixing of different types of drugs. What is the basis for this?
Volkow: At the beginning of the opiate pandemic, mortality was mainly associated with white Americans, many in rural or semi-suburban areas of the Appalachian states and in New Mexico and Arizona. That has shifted. The highest increase in mortality from opioids, predominantly driven by fentanyl, is now among Black Americans. They’ve had very, very high rates of mortality during the COVID pandemic. And when you look at mortality from methamphetamine, it’s chilling to realize that the risk of dying from methamphetamine overdose is 12-fold higher among American Indians and Alaskan Natives than other groups. This should make us pause to think about what’s driving these terrible racial disparities.
As for drug combinations, many deaths from methamphetamine or cocaine—an estimated 50 percent—are linked to these stimulant drugs being combined with fentanyl or heroin. Dealers are lacing these non-opioid drugs with cheaper, yet potent, opioids to make a larger profit. Someone who’s addicted to a stimulant drug like cocaine or methamphetamine is not tolerant to opioids, which means they are going to be at high risk of overdose if they get a stimulant drug that’s laced with an opioid like fentanyl. That’s been contributing to the sharp rise in mortality from non-opioid drugs.
Collins: I’m glad you raised the issue of health disparities. 2020 will go down as a year in which our nation had to focus on three public health crises at once. The first is the crisis of opioid use disorder and rising mortality from use of other drugs. The second is COVID-19. And the third is the realization, although the problem has been there all along, that health disparities continue to shorten the lives of far too many people.
The latter crisis has little to do with biology, but everything to do with the way in which our society still is afflicted by structural racism. We at NIH are looking at this circumstance, realizing that our own health disparities research agenda needs to be rethought. We have not fully incorporated all the factors that play out in health inequities and racial inequities in our country.
You were also talking about how stimulants have become more widespread. What about treatments for people with stimulant use disorders?
Volkow: For opioid addiction, we’re lucky because we have very effective medications: methadone, buprenorphine, naltrexone. On top of that, we have naloxone, Narcan, that if administered on time, can save the life of a person who has overdosed.
We don’t have any FDA-approved medication for methamphetamine addiction, and we don’t have any overdose reversal for methamphetamine. At the beginning of this year, we funded a large clinical trial aimed at investigating the benefits of the combination of two medications that were already approved as anti-depressants and for the treatment of smoking cessation and alcoholism. It found this combination significantly inhibits the urge to take drugs and therefore helps people stay away from use of methamphetamine. Now, we want to replicate these findings, and to tie that replication study in with guidelines from the FDA on what is needed to approve our new indication for these medications. Why? Because then insurance can cover it, and that will increase the likelihood that people will get treated.
Another exciting possibility is a monoclonal antibody against methamphetamine that’s in Phase 2 clinical trials. If someone comes into the emergency room with an overdose of a combination of opioid and methamphetamine, naloxone often will not work. But this monoclonal antibody with naloxone may offer a greater likelihood of success.
Another thing that’s promising is that investigators have been able to modify monoclonal antibodies so they stay in the bloodstream for a longer time. That means we may someday be able to use this passive immunization approach as a treatment for methamphetamine addiction.
Collins: That’s good to hear. Speaking of progress, is there any you want to point to within HEAL?
Volkow: There’s a lot of excitement surrounding medication development. We’re interested in developing antidotes that will be more effective in reversing overdose deaths from fentanyl. We’re also interested in providing longer lasting medications for treatment of opioid use disorders, which would improve the likelihood of patients being protected from overdoses.
The Justice Community Opioid Innovation Network (JCOIN) is another HEAL landmark project. It involves a network of researchers that is working with judges and with the workers in jail and prison systems responsible for taking care of individuals with substance use disorders. Through this network, we’ve been able to start to harmonize practices. One thing that’s been transformative in the jail and prison system has been the embracing of telehealth. In the past, telehealth was not much of a reality in jails and prisons because of the fear of it could lead to communications that could perhaps be considered dangerous. That’s changed due to COVID-19. Now, telehealth is providing access to treatment for individuals in jail and prison, many of them with substance use disorders.
Also, because of COVID, many nonviolent individuals in jails and prisons were released. This gives us an opportunity to evaluate how best to help such individuals achieve recovery from substance use disorders. Hopefully we can generate data to show that there are much more effective strategies than incarceration for dealing with substance use disorders.
The HEALing Communities Study, involves Massachusetts, New York, Ohio, and Kentucky—four of the states with the highest rates of mortality from overdoses from the inception of the opioid epidemic. By implementing a battery of interventions for which there is evidence of benefit, this ambitious study set out to decrease overdose mortality by 40 percent in two years. Then, came COVID and turned everything upside down. Still, because we consolidated interactions between agencies, we’ve been able to apply support systems more efficiently in those communities in ways that have been very, very reinforcing. Obviously, there’ve been delays in implementation of interventions that require in-person interactions or that involve hospital emergency departments, which have been saturated with COVID patients.
We’ve learned a lot in the process. I may be too optimistic, but I do believe that we can stay on goal.
Collins: Now, I’d like to transition to a few questions from people who subscribe to the HEAL website. Announced at this meeting three years ago, the HEAL Initiative involves research participants and patients and stakeholders—especially people who have lived experience with pain, addiction, or both.
Let’s get to the first question: “What is NIH doing through HEAL to address the stigma that prevents people who need opioid medications for treatment from getting them?”
Volkow: A crucial question. As we look at the issue of stigma, we need to recognize that there are structural issues in how our society is prioritizing the importance of substance use disorders and the investments devoted to them. And we need to recognize that substance use disorder doesn’t exist in isolation; it is frequently comorbid with mental illness.
We need to listen. Some of the issues that we believe are most problematic are not. We need to empower these communities to speak up and help them do so. This is probably one of the most important things that we can do in terms of addressing stigma for addiction.
Collins: Absolutely. The HEAL Initiative has a number of projects that are focusing on stigma and coming up with tools to help reduce this. And here’s our second question: “In small communities, how can we provide more access to medications for opioid use disorder?”
Volkow: One project funded through HEAL was to evaluate the effectiveness of community pharmacies for delivering buprenorphine to individuals with opioid use disorder. The results show that patients receiving buprenorphine through community pharmacies in rural areas had as good outcomes as patients being treated by specialized clinicians on site.
Another change that’s made things easier is that in March 2020, the DEA relaxed its rules on how a physician can prescribe buprenorphine. In the past, you needed to go physically to see a doctor. Now, the DEA allows a patient to be initiated on buprenorphine through telehealth, and that’s opened the possibility of greater access to treatment in rural communities.
My perspective is let’s look at innovative ways of solving problems. Because the technology is changing in so many ways and so rapidly, let’s take advantage of it.
Collins: Totally with you on that. If there’s a silver lining to COVID-19, it’s that we’ve been forced to take stock of the ways we’ve been doing things. We will learn from this pandemic and change the way we approach so many things in health and medicine as a result. Certainly, opioid use disorder ought to be very high on that list. Let’s move on to another question: “What is the HEAL initiative doing to promote prevention of opioid use?”
Volkow: This is where the HEAL initiative is aiming to provide alternative treatments for the management of pain that reduce the risk of addiction.
Then there’s the issue of prevention in people who start to take opioids because they either want to get high or escape. With the COVID pandemic, we’ve seen increases in anxiety and in depression. Those are factors that can put a teenager or young adult on a trajectory for higher risk of substance use disorders.
So, what is HEAL doing? There is prevention research specifically targeted, for example, at the transition from adolescence to young adulthood. That is the period of greatest vulnerability of uptake of opioids, or drugs of misuse. We’re also targeting minority groups that may be at very, very high risk. We want to be able to understand the factors that make them more vulnerable to tailor prevention interventions more effectively.
Collins: Today, we’ve shared some of the issues that NIH is wrestling with in its efforts to address the crisis of opioid misuse and overdose, as well as other drugs that are now very much part of the challenge. To learn more, go to the HEAL website. You can also send us your thoughts through the HEAL Idea Exchange.
These developments give me hope in the wake of a very difficult year. Clearly, we still have the capacity to work together, we are resilient, and we are determined to put an end to our nation’s opioid crisis.
Volkow: Francis, I want to thank you for your incredible leadership and your support. I hope the COVID pandemic will bring forth a more equitable system, in which all people are given the chance for resilience that maximizes their life, happiness, and productivity. I think science is an extraordinary tool to help us do that.
Links:
Video: The 2021 Rx Drug Abuse & Heroin Summit: Francis Collins with Nora Volkow (NIH)
COVID-19 Research (NIH)
Helping to End Addiction Long-term (HEAL) Initiative (NIH)
HEAL Idea Exchange (NIH)
National Institute on Drug Abuse (NIH)
COVID-19 Vaccine Appears Well-Tolerated and Effective in Developing Antibodies in Small Study of Older Adults
Posted on by Dr. Francis Collins

It’s been truly breathtaking to watch the progress being made on a daily basis to develop safe and effective vaccines for SARS-CoV-2, the novel coronavirus that causes COVID-19. Indeed, months sooner than has ever been possible for a newly emerging infection, several promising vaccines are already working their way through Phase 3 studies, the final stage of clinical evaluation. I remain optimistic that we will have one or more vaccines that prove to be safe and effective by January 2021.
But, as encouraging as the early data have been, uncertainty has remained over whether vaccines that appear safe and effective in developing antibodies in younger adults will work as well in older people, too. It’s a critical issue given that older individuals also are at greater risk for severe or life-threatening illness if they do get sick from COVID-19.
So, I’m pleased to highlight some recent findings, published in the New England Journal of Medicine [1], from an early Phase 1 clinical trial that was expanded to include 40 adults over age 55. While we eagerly await the results of ongoing and larger studies, these early data suggest that an innovative COVID-19 vaccine co-developed by NIH’s Vaccine Research Center (VRC), in partnership with Moderna Inc., Cambridge, MA, is both well tolerated and effective in generating a strong immune response when given to adults of any age.
The centerpiece of the vaccine in question, known as mRNA-1273, is a small, non-infectious snippet of messenger RNA (mRNA). When this mRNA is injected into muscle, a person’s own body will begin to make the key viral spike protein. As the immune system detects this spike protein, it spurs the production of antibodies that may help to fend off the novel SARS-CoV-2.
Earlier findings from the NIH-supported phase 1 human clinical trial found mRNA-1273 was safe and effective in generating a vigorous immune response in people ages 18 to 55, when delivered in two injections about a month apart. Based on those findings, a large Phase 3 clinical trial is currently enrolling 30,000 volunteers, with results expected in the next few weeks [2]. But, given that immune response to many other vaccines tends to grow weaker with age, how well would this new COVID-19 vaccine work for older individuals?
To find out, a team at Kaiser Permanente Washington Health Research Institute, Seattle, and Emory University School of Medicine, Atlanta, expanded the initial Phase 1 trial to include 20 healthy volunteers ages 56 to 70 and another 20 healthy volunteers ages 71 and older. Ten volunteers in each of the two older age groups received a lower dose of the vaccine (25 micrograms) in two injections given about a month apart. The other 10 in each age group received a higher dose (100 micrograms), given on the same schedule.
Here’s what they found:
• No volunteers suffered serious adverse events. The most common adverse events were mild-to-moderate in severity and included headache, fatigue, muscle aches, chills and pain at the injection site. Those symptoms occurred most often after the second dose and in individuals receiving the higher dose of 100 micrograms.
• Volunteers showed a rapid production of protective antibodies against the spike protein following immunization. After the second injection, all participants showed a strong immune response, with production of robust binding and neutralizing antibodies against SARS-CoV-2.
• The higher dose of 100 micrograms safely produced a stronger immune response compared to the lower dose, supporting its use in larger clinical studies.
• Most importantly, the immune response observed in these older individuals was comparable to that seen previously in younger adults.
The researchers will continue to follow the volunteer trial participants of all ages for about a year to monitor the vaccine’s longer-term effects. But these findings provided support for continued testing of this promising vaccine in older adults in the ongoing Phase 3 clinical trial.
There are currently four SARS-CoV-2 vaccines in phase 3 clinical trials in the United States (though two are currently on hold). Trials of two more vaccines are expected start in the next month or two.
It is not known whether all of these vaccines will have the same vigorous immune response in older individuals that has been demonstrated for this one. But if more than one of these vaccines turns out to be safe and effective, it will be important to know about the response in various populations, so that distribution to high-risk groups can be planned accordingly.
References:
[1] Safety and immunogenicity of SARS-CoV-2 mRNA-1273 vaccine in older adults. Anderson EJ, Rouphael NG, Widge AT, Jackson LA, Roberts PC, Makhene M, Chappell JD, Denison MR, Stevens LJ, Pruijssers AJ, McDermott AB, Flach B, Lin BC, Doria-Rose NA, O’Dell S, Schmidt SD, Corbett KS, Swanson PA 2nd, Padilla M, Neuzil KM, Bennett H, Leav B, Makowski M, Albert J, Cross K, Edara VV, Floyd K, Suthar MS, Martinez DR, Baric R, Buchanan W, Luke CJ, Phadke VK, Rostad CA, Ledgerwood JE, Graham BS, Beigel JH; mRNA-1273 Study Group. N Engl J Med. 2020 Sep 29.
[2] “Phase 3 clinical trial of investigational vaccine for COVID-19 begins.” National Institutes of Heath. July 27, 2020
Links:
Coronavirus (COVID-19) (NIH)
COVID-19 Prevention Network (National Institute of Allergy and Infectious Diseases/NIH)
Dale and Betty Bumpers Vaccine Research Center (National Institute of Allergy and Infectious Diseases/NIH)
Moderna, Inc. (Cambridge, MA)
Safety and Immunogenicity Study of 2019-nCoV Vaccine (mRNA-1273) for Prophylaxis of SARS-CoV-2 Infection (COVID-19) (ClinicalTrials.gov)
NIH Support: National Institute of Allergy and Infectious Diseases
Another Milestone in COVID-19 Vaccine Research
Posted on by Dr. Francis Collins

Searching for Ways to Prevent Life-Threatening Blood Clots in COVID-19
Posted on by Dr. Francis Collins

Six months into the coronavirus disease 2019 (COVID-19) pandemic, researchers still have much to learn about the many ways in which COVID-19 can wreak devastation on the human body. Among the many mysteries is exactly how SARS-CoV-2, which is the novel coronavirus that causes COVID-19, triggers the formation of blood clots that can lead to strokes and other life-threatening complications, even in younger people.
Recently, I had a chance to talk with Dr. Gary Gibbons, Director of NIH’s Heart, Lung, and Blood Institute (NHLBI) about what research is being done to tackle this baffling complication of COVID-19. Our conversation took place via videoconference, with him connecting from his home in Washington, D.C., and me linking in from my home just up the road in Maryland. Here’s a condensed transcript of our chat:
Collins: I’m going to start by asking about the SARS-CoV-2-induced blood clotting not only in the lungs, but in other parts of the body. What do we know about the virus that would explain this?
Gibbons: It seems like every few weeks another page gets turned on COVID-19, and we learn even more about how this virus affects the body. Blood clots are one of the startling and, unfortunately, devastating complications that emerged as patients were cared for, particularly in New York City. It became apparent that certain individuals had difficulty getting enough oxygen into their system. The difficulty couldn’t be explained entirely by the extent of the pneumonia affecting the lungs’ ability to exchange oxygen.
It turned out that, in addition to the pneumonia, blood clots in the lungs were compromising oxygenation. But some patients also had clotting, or thrombotic, complications in their veins and arteries in other parts of the body. Quite puzzling. There were episodes of relatively young individuals in their 30s and 40s presenting with strokes related to blood clots affecting the arterial circulation to the brain.
We’re still trying to understand what promotes the clotting. One clue involves the endothelial cells that form the inner lining of our blood vessels. These cells have on their surface a protein called the angiotensin-converting enzyme 2 (ACE2) receptor, and this clue is important for two reasons. One, the virus attaches to the ACE2 receptor, using it as an entry point to infect cells. Two, endothelial-lined blood vessels extend to every organ in the body. Taken together, it seems that some COVID-19 complications relate to the virus attaching to endothelial cells, not only in the lungs, but in the heart and multiple organs.
Collins: So, starting in the respiratory tree, the virus somehow breaks through into a blood vessel and then gets spread around the body. There have been strange reports of people with COVID-19 who may not get really sick, but their toes look frostbitten. Is “COVID toes,” as some people call it, also part of this same syndrome?
Gibbons: We’re still in the early days of learning about this virus. But I think this offers a further clue that the virus not only affects large vessels but small vessels. In fact, clots have been reported at the capillary level, and that’s fairly unusual. It’s suggestive that an interaction is taking place between the platelets and the endothelial surface.
Normally, there’s a tightly regulated balance in the bloodstream between pro-coagulant and anticoagulant proteins to prevent clotting and keep the blood flowing. But when you cut your finger, for example, you get activation for blood clots in the form of a protein mesh. It looks like a fishing net that can help seal the injury. In addition, platelets in the blood stream help to plug the holes in that fishing net and create a real seal of a blood vessel.
Well, imagine it happening in those small vessels, which usually have a non-stick endothelial surface, almost like Teflon, that prevents clotting. Then the virus comes along and tips the balance toward promoting clot formation. This disturbs the Teflon-like property of the endothelial lining and makes it sticky. It’s incredible the tricks this virus has learned by binding onto one of these molecules in the endothelial lining.
Collins: Who are the COVID-19 patients most at risk for this clotting problem?
Gibbons: Unfortunately, it appears right now that older adults are among the most vulnerable. They have a lot of the risks for the formation of these blood clots. What’s notable is these thrombotic complications are also happening to relatively young adults or middle-aged individuals who don’t have a lot of other chronic conditions, or comorbidities, to put them at higher risk for severe disease. Again, it’s suggestive that this virus is doing something that is particular to the coagulation system.
Collins: We’d love to have a way of identifying in advance the people who are most likely to get into trouble with blood clotting. They might be the ones you’d want to start on an intervention, even before you have evidence that things are getting out of control. Do you have any kind of biomarker to tell you which patients might benefit from early intervention?
Gibbons: Biomarkers are being actively studied. What we do know from some earlier observations is that you can assess the balance of clotting and anticlotting factors in the blood by measuring a biomarker called D-dimer. It’s basically a protein fragment, a degradation product, from a prior clot. It tells you a bit about the system’s activity in forming and dissolving clots.
If there’s a lot of D-dimer activity, it suggests a coagulation cascade is jazzed up. In those patients, it’s probably a clue that this is a big trigger in terms of coagulation and thrombosis. So, D-dimer levels could maybe tell us which patients need really aggressive full anticoagulation.
Collins: Have people tried empirically using blood thinners for people who seem to be getting into trouble with this clotting problem?
Gibbons: There’s a paper out of the Mount Sinai in New York City that looked at thousands of patients being treated for COVID-19 [1]. Based on clinical practice and judgments, one of the striking findings is that those who were fully anticoagulated had better survival than those who were not. Now, this was not a randomized, controlled clinical trial, where some were given full anticoagulation and others were not. It was just an observational study that showed an association. But this study indicated indirectly that by giving the blood thinners, changing that thrombotic risk, maybe it’s possible to reduce morbidity and mortality. That’s why we need to do a randomized, controlled clinical trial to see if it can be used to reduce these case fatality rates.
Collins: You and your colleagues got together and came up with a design for such a clinical trial. Tell us about that.
Gibbons: My institute studies the heart, lung, and blood. The virus attacks all three. So, our community has a compelling need to lean in and study COVID-19. Recently, NIH helped to launch a public-private partnership called Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV). As the name spells out, this initiative provides is a clinical platform to generate life-saving treatments as we wait for the development of a vaccine.
Through ACTIV, a protocol is now in the final stages of review for a clinical trial that will involve a network of hospitals and explore the question: is it sufficient to try a low-dose thrombo-prophylactic, or clot preventative, approach versus full anticoagulation? Some think patients ought to have full anticoagulation, but that’s not without risk. So, we want to put that question to the test. As part of that, we’ll also learn more about biomarkers and what could be predictive of individuals getting the greatest benefit.
If we find that fully anticoagulating patients prevents clots, then that’s great. But it begs the question: what happens when patients go home? Is it sufficient to just turn off the drip and let them go their merry way? Should they have a low dose thrombo-prophylactic regimen for a period of time? If so, how long? Or should they be fully anticoagulated with oral anticoagulation for a certain period of time? All these and other questions still remain.
Collins: This can make a huge difference. If you’re admitted to the hospital with COVID-19, that means you’re pretty sick and, based on the numbers that I’ve seen, your chance of dying is about 12 percent if nothing else happens. If we can find something like an anticoagulant that would reduce that risk substantially, we can have a huge impact on reducing deaths from COVID-19. How soon can we get this trial going, Gary?
Gibbons: We have a sense of urgency that clearly this pandemic is taking too many lives and time is of the essence. So, we’ve indeed had a very streamlined process. We’re leveraging the fact that we have clinical trial networks, where regardless of what they were planning to do, it’s all hands on deck. As a result, we’re able to move faster to align with that sense of urgency. We hope that we can be off to a quick launch within the next two to three weeks with the anticoagulation trials.
Collins: This is good because people are waiting on the vaccines, but realistically we won’t know whether the vaccines are working for several more months, and having them available for lots of people will be at the very end of this year or early 2021 at best. Meanwhile, people still are going to be getting sick with COVID-19. We want to be able to have as many therapeutic options as possible to offer to them. And this seems like a pretty exciting one to try and move forward as quickly as possible. You and your colleagues deserve a lot of credit for bringing this to everybody’s attention.
But before we sign off, I have to raise another issue of deep significance. Gary, I think both of us are struggling not only with the impact of COVID-19 on the world, but the profound sorrow, grief, frustration, and anger that surrounds the death of George Floyd. This brings into acute focus the far too numerous other circumstances where African Americans have been mistreated and subjected to tragic outcomes.
This troubling time also shines a light on the health disparities that affect our nation in so many ways. We can see what COVID-19 has done to certain underrepresented groups who have borne an undue share of the burden, and have suffered injustices at the hands of society. It’s been tough for many of us to admit that our country is far from treating everyone equally, but it’s a learning opportunity and a call to redouble our efforts to find solutions.
Gary, you’ve been a wonderful leader in that conversation for a long time. I want to thank you both for what you’re doing scientifically and for your willingness to speak the truth and stand up for what’s right and fair. It’s been great talking to you about all these issues.
Gibbons: Thank you. We appreciate this opportunity to fulfill NIH’s mission of turning scientific discovery into better health for all. If there’s any moment that our nation needs us, this is it.
Reference:
[1] Association of Treatment Dose Anticoagulation With In-Hospital Survival Among Hospitalized Patients With COVID-19. Paranjpe I, Fuster V, Lala A, Russak A, Glicksberg BS, Levin MA, Charney AW, Narula J, Fayad ZA, Bagiella E, Zhao S, Nadkarni GN. J Am Coll Cardiol. 2020 May 5;S0735-1097(20)35218-9.
Links:
Coronavirus (COVID-19) (NIH)
“Rising to the Challenge of COVID-19: The NHLBI Community Response,” Director’s Messages, National Heart, Lung, and Blood Institute/NIH, April 29, 2020.
Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) (NIH)
Encouraging News for Kids with Neurofibromatosis Type 1
Posted on by Dr. Francis Collins
Amid all the headlines and uncertainty surrounding the current COVID-19 pandemic, it’s easy to overlook the important progress that biomedical research is making against other diseases. So, today, I’m pleased to share word of what promises to be the first effective treatment to help young people suffering from the consequences of a painful, often debilitating genetic disorder called neurofibromatosis type 1 (NF1).
This news is particularly meaningful to me because, 30 years ago, I led a team that discovered the gene that underlies NF1. About 1 in 3,000 babies are born with NF1. In about half of those affected, a type of tumor called a plexiform neurofibroma arises along nerves in the skin, face, and other parts of the body. While plexiform neurofibromas are not cancerous, they grow steadily and can lead to severe pain and a range of other health problems, including vision and hearing loss, hypertension, and mobility issues.
The good news is the results of a phase II clinical trial involving NF1, just published in the New England Journal of Medicine. The trial was led by Brigitte Widemann and Andrea Gross, researchers in the Center for Cancer Research at NIH’s National Cancer Institute.
The trial’s results confirm that a drug originally developed to treat cancer, called selumetinib, can shrink inoperable tumors in many children with NF1. They also establish that the drug can help affected kids make significant improvements in strength, range of motion, and quality of life. While selumetinib is not a cure, and further studies are still needed to see how well the treatment works in the long term, these results suggest that the first effective treatment for NF1 is at last within our reach.
Selumetinib blocks a protein in human cells called MEK. This protein is involved in a major cellular pathway known as RAS that can become dysregulated and give rise to various cancers. By blocking the MEK protein in animal studies and putting the brakes on the RAS pathway when it malfunctions, selumetinib showed great initial promise as a cancer drug.
Selumetinib was first tested several years ago in people with a variety of other cancers, including ovarian and non-small cell lung cancers. The clinical research looked good at first but eventually stalled, and so did much of the initial enthusiasm for selumetinib.
But the enthusiasm picked up when researchers considered repurposing the drug to treat NF1. The neurofibromas associated with the condition were known to arise from a RAS-activating loss of the NF1 gene. It made sense that blocking the MEK protein might blunt the overactive RAS signal and help to shrink these often-inoperable tumors.
An earlier phase 1 safety trial looked promising, showing for the first time that the drug could, in some cases, shrink large NF1 tumors [2]. This fueled further research, and the latest study now adds significantly to that evidence.
In the study, Widemann and colleagues enrolled 50 children with NF1, ranging in age from 3 to 17. Their tumor-related symptoms greatly affected their wellbeing and ability to thrive, including disfigurement, limited strength and motion, and pain. Children received selumetinib alone orally twice a day and went in for assessments at least every four months.
As of March 2019, 35 of the 50 children in the ongoing study had a confirmed partial response, meaning that their tumors had shrunk by more than 20 percent. Most had maintained that response for a year or more. More importantly, the kids also felt less pain and were more able to enjoy life.
It’s important to note that the treatment didn’t work for everyone. Five children stopped taking the drug due to side effects. Six others progressed while on the drug, though five of them had to reduce their dose because of side effects before progressing. Nevertheless, for kids with NF1 and their families, this is a big step forward.
Drug developer AstraZeneca, working together with the researchers, has submitted a New Drug Application to the Food and Drug Administration (FDA). While they’re eagerly awaiting the FDA’s decision, the work continues.
The researchers want to learn much more about how the drug affects the health and wellbeing of kids who take it over the long term. They’re also curious whether it could help to prevent the growth of large tumors in kids who begin taking it earlier in the course of the disease, and whether it might benefit other features of the disorder. They will continue to look ahead to other potentially promising treatments or treatment combinations that may further help, and perhaps one day even cure, kids with NF1. So, even while we cope with the COVID-19 pandemic, there are reasons to feel encouraged and grateful for continued progress made throughout biomedical research.
References:
[1] Selumitinib in children with inoperable plexiform neurofibromas. New England Journal of Medicine. Gross AM, Wolters PL, Dombi E, Baldwin A, Whitcomb P, Fisher MJ, Weiss B, Kim A, Bornhorst M, Shah AC, Martin S, Roderick MC, Pichard DC, Carbonell A, Paul SM, Therrien J, Kapustina O, Heisey K, Clapp DW, Zhang C, Peer CJ, Figg WD, Smith M, Glod J, Blakeley JO, Steinberg SM, Venzon DJ, Doyle LA, Widemann BC. 18 March 2020. N Engl J Med. 2020 Mar 18. [Epub ahead of publication.]
[2] Activity of selumetinib in neurofibromatosis type 1-related plexiform neurofibromas. Dombi E, Baldwin A, Marcus LJ, Fisher MJ, Weiss B, Kim A, Whitcomb P, Martin S, Aschbacher-Smith LE, Rizvi TA, Wu J, Ershler R, Wolters P1, Therrien J, Glod J, Belasco JB, Schorry E, Brofferio A, Starosta AJ, Gillespie A, Doyle AL, Ratner N, Widemann BC. N Engl J Med. 2016 Dec 29;375(26):2550-2560.
Links:
Neurofibromatosis Fact Sheet (National Institute of Neurological Disorders and Stroke/NIH)
Brigitte Widemann (National Cancer Institute/NIH)
Andrea Gross (National Cancer Institute/NIH)
NIH Support: National Cancer Institute
Targeting the Microbiome to Treat Malnutrition
Posted on by Dr. Francis Collins

Credit: International Centre for Diarrhoeal Disease Research, Bangladesh
A few years ago, researchers discovered that abnormalities in microbial communities, or microbiomes, in the intestine appear to contribute to childhood malnutrition. Now comes word that this discovery is being translated into action, with a new study showing that foods formulated to repair the “gut microbiome” may help malnourished kids rebuild their health [1].
In a month-long clinical trial in Bangladesh, 63 children received either regular foods to treat malnutrition or alternative formulations for needed calories and nutrition that also encouraged growth of beneficial microbes in the intestines. The kids who ate the microbiome-friendly diets showed improvements in their microbiome, which helps to extract and metabolize nutrients in our food to help the body grow. They also had significant improvements in key blood proteins associated with bone growth, brain development, immunity, and metabolism; those who ate standard therapeutic food did not experience the same benefit.
Globally, malnutrition affects an estimated 238 million children under the age 5, stunting their normal growth, compromising their health, and limiting their mental development [2]. Malnutrition can arise not only from a shortage of food but from dietary imbalances that don’t satisfy the body’s need for essential nutrients. Far too often, especially in impoverished areas, the condition can turn extremely severe and deadly. And the long term effects on intellectual development can limit the ability of a country’s citizens to lift themselves out of poverty.
Jeffrey Gordon, Washington University School of Medicine in St. Louis, and his NIH-supported research team have spent decades studying what constitutes a normal microbiome and how changes can affect health and disease. Their seminal studies have revealed that severely malnourished kids have “immature” microbiomes that don’t develop in the intestine like the microbial communities seen in well nourished, healthy children of the same age.
Gordon and team have also found that this microbial immaturity doesn’t resolve when kids consume the usual supplemental foods [3]. In another study, they turned to mice raised under sterile conditions and with no microbes of their own to demonstrate this cause and effect. The researchers colonized the intestines of the germ-free mice with microbes from malnourished children, and the rodents developed similar abnormalities in weight gain, bone growth, and metabolism [4].
All of this evidence raised a vital question: Could the right combination of foods “mature” the microbiome and help to steer malnourished children toward a healthier state?
To get the answer, Gordon and his colleagues at the International Centre for Diarrhoeal Disease Research, Dhaka, Bangladesh, led by Tahmeed Ahmed, first had to formulate the right, microbiome-friendly food supplements, and that led to some interesting science. They carefully characterized over time the immature microbiomes found in Bangladeshi children treated for severe malnutrition. This allowed them to test their new method for analyzing how individual microbial species fluctuate over time and in relationship to one another in the intestine [5]. The team then paired up these data with measurements of a set of more than 1,300 blood proteins from the children that provide “readouts” of their biological state.
Their investigation identified a network of 15 bacterial species that consistently interact in the gut microbiomes of Bangladeshi children. This network became their means to characterize sensitively and accurately the development of a child’s microbiome and/or its relative state of repair.
Next, they turned to mice colonized with the same collections of microbes found in the intestines of the Bangladeshi children. Gordon’s team then tinkered with the animals’ diets in search of ingredients commonly consumed by young children in Bangladesh that also appeared to encourage a healthier, more mature microbiome. They did similar studies in young pigs, whose digestive and immune systems more closely resemble humans.
The Gordon team settled on three candidate microbiome-friendly formulations. Two included chickpea flour, soy flour, peanut flour, and banana at different concentrations; one of these two also included milk powder. The third combined chickpea flour and soy flour. All three contained similar amounts of protein, fat, and calories.
The researchers then launched a randomized, controlled clinical trial with children from a year to 18 months old with moderate acute malnutrition. These young children were enrolled into one of four treatment groups, each including 14 to 17 kids. Three groups received one of the newly formulated foods. The fourth group received standard rice-and-lentil-based meals.
The children received these supplemental meals twice a day for four weeks at the International Centre for Diarrhoeal Disease Research followed by two-weeks of observation. Mothers were encouraged throughout the study to continue breastfeeding their children.
The formulation containing chickpea, soy, peanut, and banana, but no milk powder, stood out above the rest in the study. Children taking this supplement showed a dramatic shift toward a healthier state as measured by those more than 1,300 blood proteins. Their gut microbiomes also resembled those of healthy children their age.
Their new findings published in the journal Science offer the first evidence that a therapeutic food, developed to support the growth and development of a healthy microbiome, might come with added benefits for children suffering from malnutrition. Importantly, the researchers took great care to design the supplements with foods that are readily available, affordable, culturally acceptable, and palatable for young children in Bangladesh.
A month isn’t nearly long enough to see how the new foods would help children grow and recover over time. So, the researchers are now conducting a much larger study of their leading supplement in children with histories of malnutrition, to explore its longer-term health effects for them and their microbiomes. The hope is that these new foods and others adapted for use around the world soon will help many more kids grow up to be healthy adults.
References:
[1] Effects of microbiota-directed foods in gnotobiotic animals and undernourished children. Gehrig JL, Venkatesh S, Chang HW, Hibberd MC, Kung VL, Cheng J, Chen RY, Subramanian S, Cowardin CA, Meier MF, O’Donnell D, Talcott M, Spears LD, Semenkovich CF, Henrissat B, Giannone RJ, Hettich RL, Ilkayeva O, Muehlbauer M, Newgard CB, Sawyer C, Head RD, Rodionov DA, Arzamasov AA, Leyn SA, Osterman AL, Hossain MI, Islam M, Choudhury N, Sarker SA, Huq S, Mahmud I, Mostafa I, Mahfuz M, Barratt MJ, Ahmed T, Gordon JI. Science. 2019 Jul 12;365(6449).
[2] Childhood Malnutrition. World Health Organization
[3] Persistent gut microbiota immaturity in malnourished Bangladeshi children. Subramanian S, Huq S, Yatsunenko T, Haque R, Mahfuz M, Alam MA, Benezra A, DeStefano J, Meier MF, Muegge BD, Barratt MJ, VanArendonk LG, Zhang Q, Province MA, Petri WA Jr, Ahmed T, Gordon JI. Nature. 2014 Jun 19;510(7505):417-21.
[4] Gut bacteria that prevent growth impairments transmitted by microbiota from malnourished children. Blanton LV, Charbonneau MR, Salih T, Barratt MJ, Venkatesh S, Ilkaveya O, Subramanian S, Manary MJ, Trehan I, Jorgensen JM, Fan YM, Henrissat B, Leyn SA, Rodionov DA, Osterman AL, Maleta KM, Newgard CB, Ashorn P, Dewey KG, Gordon JI. Science. 2016 Feb 19;351(6275).
[5] A sparse covarying unit that describes healthy and impaired human gut microbiota development. Raman AS, Gehrig JL, Venkatesh S, Chang HW, Hibberd MC, Subramanian S, Kang G, Bessong PO, Lima AAM, Kosek MN, Petri WA Jr, Rodionov DA, Arzamasov AA, Leyn SA, Osterman AL, Huq S, Mostafa I, Islam M, Mahfuz M, Haque R, Ahmed T, Barratt MJ, Gordon JI. Science. 2019 Jul 12;365(6449).
Links:
Childhood Nutrition Facts (Centers for Disease Control and Prevention)
Gordon Lab (Washington University School of Medicine in St. Louis)
International Centre for Diarrhoeal Disease Research (Dhaka, Bangladesh)
NIH Support: National Institute of Diabetes and Digestive and Kidney Diseases; National Institute of General Medical Sciences; National Institute of Arthritis and Musculoskeletal and Skin Diseases; National Center for Advancing Translational Sciences; National Cancer Institute
Personalized Combination Therapies Yield Better Cancer Outcomes
Posted on by Dr. Francis Collins

Gratifying progress has been made recently in an emerging area of cancer medicine called precision oncology. It’s a bold attempt to target treatment to the very genes and molecules driving a cancer, aiming to slow or even halt its growth. But there’s always more to learn. Now comes evidence that, while a single well-matched drug might be good, a tailored combination of drugs that attack a cancer in multiple ways at once might be even better.
The findings come from the I-PREDICT clinical trial, which treated people with advanced cancer who hadn’t benefited from previous therapy [1]. The NIH-funded team found that analyzing a tumor’s unique genetic and molecular profile provided enough information to recommend individualized combination therapies to patients. What’s more, patients who followed their individualized combination therapies most closely lived longer, with longer periods of progression-free disease, than did those who took fewer of the recommended drugs.
In most previous clinical trials of precision oncology, researchers have relied on a tumor’s unique profile to identify a single, well-matched drug to treat each patient. But cancer is complex, and, just as with certain infectious diseases, tumors commonly develop resistance to a single drug.
In the trial reported in Nature Medicine, researchers led by Razelle Kurzrock and Jason Sicklick, University of California, San Diego, wondered if they could improve treatment responses by tailoring combinations of cancer drugs to target as many molecular and genetic changes in a person’s cancer as possible.
To test the potential for this strategy to work, the researchers enrolled 83 people with various cancers that had advanced despite previous treatment. Tumor tissue from each patient was run through a comprehensive battery of tests, and researchers sequenced hundreds of genes to look for telltale alterations in their DNA.
They also looked for evidence that a cancer had defects affecting the DNA “mismatch repair” pathway, which causes some tumors to generate larger numbers of mutations than others. Mismatch repair defects have been shown to predict better responses to immunotherapies, which are designed to harness the immune system against cancer .
With all the data in hand, a special panel of oncologists, pharmacologists, cancer biologists, geneticists, surgeons, radiologists, pathologists, and bioinformatics experts consulted to arrive at the right customized combination of drugs for each patient.
The panel’s findings were presented to the health care team working with each patient. The physician for each patient then had the final decision on whether to recommend the treatment regimen, balancing the panel’s suggestions with other real-world factors, such as a patient’s insurance coverage, availability of drugs, and his or her treatment preference.
Ten patients decided to stick with unmatched treatment. But 73 participants received a customized combination therapy. As no two molecular profiles were identical, the customized treatment regimens varied from person to person.
Many people received designer drugs targeting particular genetic alterations. Some also received checkpoint inhibitor immunotherapies to unleash the immune system against cancer. Four people also were treated with hormone therapies in combination with molecularly targeted drugs. In all, most regimens combined two to five drugs to target each cancer profile.
Participants were followed until their cancer progressed, they could no longer take treatment, or they died. For each person, the researchers calculated a “matching score,” roughly defined as the number of molecular alterations matched to administered drug(s), with some further calculations.
The evidence showed that those with matching scores greater than 50 percent, meaning more than half of a tumor’s identified aberrations had been targeted, were more likely to have stopped the progression of their cancers. Importantly, half of patients with the higher matching scores had prolonged stable disease (six months or longer) or a complete or partial remission. Similar results were attained in only 22 percent of those with low or no matching scores.
These encouraging results suggest that customized combinations of targeted treatments will help to advance precision oncology. However, there are still many challenges. For example, many of the combinations used in the study have not yet been safety tested. The researchers managed the potential risk of toxicities by starting patients on an initial low dose and having their physicians follow them closely while the dose was increased to a level well-tolerated by each individual patient.
And indeed, they saw no evidence that those receiving a greater proportion of “matched” drugs (i.e. those with a higher matching score) were more likely to experience adverse effects than those who took fewer drugs. So, that’s an encouraging sign.
The researchers are now enrolling patients in a new version of the I-PREDICT trial. Unlike the initial plan, patients are now being enrolled prior to receiving any treatment for a recently diagnosed aggressive, often-lethal form of cancer. The hope is that treating patients with well-matched, multi-drug treatment combinations early will yield even better results than waiting until standard treatment has failed. If correct, it would mark significant progress in building the future of precision oncology.
Reference:
[1] Molecular profiling of cancer patients enables personalized combination therapy: the I-PREDICT study. Sicklick JK, Kato S, Okamura R, Schwaederle M, Hahn ME, Williams CB, De P, Krie A, Piccioni DE, Miller VA, Ross JS, Benson A, Webster J, Stephens PJ, Lee JJ, Fanta PT, Lippman SM, Leyland-Jones B, Kurzrock R. Nat Med. 2019 Apr 22.
Links:
Precision Medicine in Cancer Treatment (National Cancer Institute/NIH)
Study of Molecular Profile-Related Evidence to Determine Individualized Therapy for Advanced or Poor Prognosis Cancers (I-PREDICT) (Clinicaltrials.gov)
Razelle Kurzrock (University of California, San Diego)
Jason Sicklick (University of California, San Diego)
NIH Support: National Cancer Institute
Most Women with Early-Stage Breast Cancer Don’t Need Chemo
Posted on by Dr. Francis Collins

Credit: National Cancer Institute, NIH
In the last few days, you may have heard that there’s been a significant development in the management of breast cancer. So here’s the NIH Director’s blog description of what’s happened. Each year, as many as 135,000 American women who’ve undergone surgery for the most common form of early-stage breast cancer face a difficult decision: whether or not to undergo chemotherapy. Genetic testing of tumor tissue has helped to inform some of these decisions, with women whose tumors score high on the breast cancer recurrence scale likely to benefit from chemo, and those with low-scoring tumors able to skip the cost and potentially serious side effects. But there’s been a catch: most tumors score somewhere in the middle, leaving women and their doctors uncertain about what to do.
Now, thanks to the long-awaited results of a large, NIH-funded clinical trial, we finally have an answer. About 70 percent of women with hormone receptor (HR)-positive, HER2-negative, axillary lymph node-negative breast cancer—including those with mid-range scores on the cancer recurrence scale—do not benefit from chemotherapy [1]. These findings promise to spare a great many women with breast cancer from unnecessary exposure to costly and potentially toxic chemotherapy.
Can Barbers Help Black Men Lower Their Blood Pressure?
Posted on by Dr. Francis Collins

Caption: Barber Eric Muhammad (left) in his barbershop taking the blood pressure of patron.
Credit: Smidt Heart Institute, Cedars-Sinai Medical Center
You expect to have your blood pressure checked and treated when you visit the doctor’s office or urgent care clinic. But what about the barbershop? New research shows that besides delivering the customary shave and a haircut, barbers might be able to play a significant role in helping control high blood pressure.
High blood pressure, or hypertension, is a particularly serious health problem among non-Hispanic black men. So, in a study involving 52 black-owned barbershops in the Los Angeles area, barbers encouraged their regular, black male patrons, ages 35 to 79, to get their blood pressure checked at their shops [1]. Nearly 320 men turned out to have uncontrolled hypertension and enrolled in the study. In a randomized manner, barbers then encouraged these men to do one of two things: attend one-on-one barbershop meetings with pharmacists who could prescribe blood pressure medicines, or set up appointments with their own doctors and consider making lifestyle changes.
The result? More than 63 percent of the men who received medications prescribed by specially-trained pharmacists lowered their blood pressure to healthy levels within 6 months, compared to less than 12 percent of those who went to see their doctors. The findings serve as a reminder that helping people get healthier doesn’t always require technological advances. Sometimes it may just involve developing more effective ways of getting proven therapy to at-risk communities.
Previous Page Next Page