24 Search Results for "Addiction Science"
Lessons Learned About Substance Use Disorders During the COVID-19 Pandemic
Posted on by Dr. Francis Collins

Every spring, I and my colleague Dr. Nora Volkow, Director of NIH’s National Institute on Drug Abuse (NIDA), join with leaders across the country in the Rx Drug Abuse and Heroin Summit. Our role is to discuss NIH’s continued progress in tackling our nation’s opioid crisis. Because of the continued threat of COVID-19 pandemic, we joined in virtually for the second year in a row.
While the demands of the pandemic have been challenging for everyone, biomedical researchers have remained hard at work to address the opioid crisis. Among the many ways that NIH is supporting these efforts is through its Helping to End Addiction Long-Term (HEAL) Initiative, which is directing more than $1.5 billion to researchers and communities across the country.
Here’s a condensed transcript of our April 6th video dialogue, which focused on the impact of the COVID-19 pandemic on people struggling with substance use disorders and those who are trying to help them.

Collins: What have we learned so far through HEAL? Well, one thing HEAL is doing is tackling the need for pain treatments that help people avoid the risks of opioids. This research has uncovered new targets and therapeutics for different types of pain, including neuropathic, post-surgical, osteoarthritic, and chemotherapy induced. We’re testing implanted devices, such as electrodes and non-invasive nerve stimulation; and looking at complementary and integrative approaches, such as phone-based physical therapy for low back pain.
Through HEAL, we’ve launched a first-in-human test of a vaccine to protect against the harmful effects of opioids, including relapse and overdose. We’re also testing a tool that provides pharmacists with a validated opioid use disorder risk measure. The goal is to identify better who’s at high risk for opioid addiction and to determine what kind of early intervention could be put in place.
Despite COVID, many clinical studies are now recruiting participants. This includes family-based prevention programs, culturally tailored interventions for hard-hit American Indian populations, and interventions that address social inequities, such as lack of housing.
We are also making progress on the truly heart-breaking problem of babies born dependent on opioids. HEAL has launched a study to test the effectiveness of a new approach to care that measures the severity of a baby’s withdrawal, based on their ability to eat, sleep, and be consoled. This approach helps provide appropriate treatment for these infants, without the use of medication when possible. We’re also developing novel technologies to help treat neonatal opioid withdrawal syndrome, including a gently vibrating hospital bassinet pad that’s received breakthrough device designation from the FDA.
2020 was an extraordinary year that was tragic in so many ways, including lives lost and economic disasters that have fallen upon families. The resilience and ingenuity of the scientific community has been impressive. Quick pivoting has resulted in some gains through research, maybe you could even call them silver linings in the midst of this terrible storm.
Nora, what’s been at the forefront of your mind as we’ve watched things unfold?
Volkow: When we did this one year ago, we didn’t know what to expect. Obviously, we were concerned that the stressors associated with a pandemic, with unknowns, are factors that have been recognized for many years to increase drug use. Unfortunately, what we’ve seen is an increase in drug use of all types across the country.
We have seen an exacerbation of the opioid epidemic, as evidenced by the number of people who have died. Already, in the 12 months ending in July 2020, there was a 24 percent increase in mortality from overdoses. Within those numbers, there was close to a 50 percent increase in mortality associated with fentanyl. We’re also seeing an increase, not just in deaths from fentanyl and other synthetic opioids, but in deaths from stimulant drugs, like cocaine and methamphetamine. And the largest increases have been very much driven by drug combinations.
So, we have the perfect storm. We have people stressed to their limits by decreases in the economy, the loss of jobs, the death of loved ones. On the other hand, we see dealers taking the opportunity to bring in drugs such as synthetic opioids and synthetic stimulants and distribute them to a much wider extent than previously seen.

Collins: On top of that, people are at risk of getting sick from COVID-19. What have we learned about the risks of coronavirus illness for people who use drugs?
Volkow: It is a double whammy. When you look at the electronic health records about the outcomes of people diagnosed with substance use disorders, you consistently see an increased risk for getting infected with COVID-19. And if you look at those who get infected, you observe a significantly increased risk of dying from COVID.
What’s driving this vulnerability? One factor is the pharmacological effects of these drugs. Basically, all of the drugs of abuse that result in addiction, notably opioids, damage the cardiopulmonary system. Some also damage the immune system. And we know that individuals who have any disruption of cardiovascular health, pulmonary health, immune function, or metabolism are at higher risk of getting infected with COVID-19 and having adverse outcomes.
But there’s another factor that’s as important—one that’s very tractable. It is the way in which our society has dealt with substance use disorders: not actually treating them as a disease that requires intervention and support for recovery. The stigmatization of individuals with addiction, the lack of access to treatment, the social isolation, have all created havoc by making these individuals so much more vulnerable to get infected with COVID-19.
They will not go to a doctor. They don’t want to be stigmatized. They need to go out into the streets to get access to the drugs. Many times, they don’t have a choice of what drugs to take because they cannot afford anything except what’s offered to them. So, many, especially those who are minorities, end up homeless or in jails or prison. Even before COVID, we knew that prisons and jails are places where infections can transmit extraordinary rapidly. You could see this was going to result in very negative outcomes for this group of individuals.
Collins: Nora, tell us more about the trends contributing to the current crisis. Maybe three or four years ago, what was going straight up was opioid use, especially heroin. Then, fentanyl started coming up very fast and that has continued. Now, we are seeing more stimulants and mixing of different types of drugs. What is the basis for this?
Volkow: At the beginning of the opiate pandemic, mortality was mainly associated with white Americans, many in rural or semi-suburban areas of the Appalachian states and in New Mexico and Arizona. That has shifted. The highest increase in mortality from opioids, predominantly driven by fentanyl, is now among Black Americans. They’ve had very, very high rates of mortality during the COVID pandemic. And when you look at mortality from methamphetamine, it’s chilling to realize that the risk of dying from methamphetamine overdose is 12-fold higher among American Indians and Alaskan Natives than other groups. This should make us pause to think about what’s driving these terrible racial disparities.
As for drug combinations, many deaths from methamphetamine or cocaine—an estimated 50 percent—are linked to these stimulant drugs being combined with fentanyl or heroin. Dealers are lacing these non-opioid drugs with cheaper, yet potent, opioids to make a larger profit. Someone who’s addicted to a stimulant drug like cocaine or methamphetamine is not tolerant to opioids, which means they are going to be at high risk of overdose if they get a stimulant drug that’s laced with an opioid like fentanyl. That’s been contributing to the sharp rise in mortality from non-opioid drugs.
Collins: I’m glad you raised the issue of health disparities. 2020 will go down as a year in which our nation had to focus on three public health crises at once. The first is the crisis of opioid use disorder and rising mortality from use of other drugs. The second is COVID-19. And the third is the realization, although the problem has been there all along, that health disparities continue to shorten the lives of far too many people.
The latter crisis has little to do with biology, but everything to do with the way in which our society still is afflicted by structural racism. We at NIH are looking at this circumstance, realizing that our own health disparities research agenda needs to be rethought. We have not fully incorporated all the factors that play out in health inequities and racial inequities in our country.
You were also talking about how stimulants have become more widespread. What about treatments for people with stimulant use disorders?
Volkow: For opioid addiction, we’re lucky because we have very effective medications: methadone, buprenorphine, naltrexone. On top of that, we have naloxone, Narcan, that if administered on time, can save the life of a person who has overdosed.
We don’t have any FDA-approved medication for methamphetamine addiction, and we don’t have any overdose reversal for methamphetamine. At the beginning of this year, we funded a large clinical trial aimed at investigating the benefits of the combination of two medications that were already approved as anti-depressants and for the treatment of smoking cessation and alcoholism. It found this combination significantly inhibits the urge to take drugs and therefore helps people stay away from use of methamphetamine. Now, we want to replicate these findings, and to tie that replication study in with guidelines from the FDA on what is needed to approve our new indication for these medications. Why? Because then insurance can cover it, and that will increase the likelihood that people will get treated.
Another exciting possibility is a monoclonal antibody against methamphetamine that’s in Phase 2 clinical trials. If someone comes into the emergency room with an overdose of a combination of opioid and methamphetamine, naloxone often will not work. But this monoclonal antibody with naloxone may offer a greater likelihood of success.
Another thing that’s promising is that investigators have been able to modify monoclonal antibodies so they stay in the bloodstream for a longer time. That means we may someday be able to use this passive immunization approach as a treatment for methamphetamine addiction.
Collins: That’s good to hear. Speaking of progress, is there any you want to point to within HEAL?
Volkow: There’s a lot of excitement surrounding medication development. We’re interested in developing antidotes that will be more effective in reversing overdose deaths from fentanyl. We’re also interested in providing longer lasting medications for treatment of opioid use disorders, which would improve the likelihood of patients being protected from overdoses.
The Justice Community Opioid Innovation Network (JCOIN) is another HEAL landmark project. It involves a network of researchers that is working with judges and with the workers in jail and prison systems responsible for taking care of individuals with substance use disorders. Through this network, we’ve been able to start to harmonize practices. One thing that’s been transformative in the jail and prison system has been the embracing of telehealth. In the past, telehealth was not much of a reality in jails and prisons because of the fear of it could lead to communications that could perhaps be considered dangerous. That’s changed due to COVID-19. Now, telehealth is providing access to treatment for individuals in jail and prison, many of them with substance use disorders.
Also, because of COVID, many nonviolent individuals in jails and prisons were released. This gives us an opportunity to evaluate how best to help such individuals achieve recovery from substance use disorders. Hopefully we can generate data to show that there are much more effective strategies than incarceration for dealing with substance use disorders.
The HEALing Communities Study, involves Massachusetts, New York, Ohio, and Kentucky—four of the states with the highest rates of mortality from overdoses from the inception of the opioid epidemic. By implementing a battery of interventions for which there is evidence of benefit, this ambitious study set out to decrease overdose mortality by 40 percent in two years. Then, came COVID and turned everything upside down. Still, because we consolidated interactions between agencies, we’ve been able to apply support systems more efficiently in those communities in ways that have been very, very reinforcing. Obviously, there’ve been delays in implementation of interventions that require in-person interactions or that involve hospital emergency departments, which have been saturated with COVID patients.
We’ve learned a lot in the process. I may be too optimistic, but I do believe that we can stay on goal.
Collins: Now, I’d like to transition to a few questions from people who subscribe to the HEAL website. Announced at this meeting three years ago, the HEAL Initiative involves research participants and patients and stakeholders—especially people who have lived experience with pain, addiction, or both.
Let’s get to the first question: “What is NIH doing through HEAL to address the stigma that prevents people who need opioid medications for treatment from getting them?”
Volkow: A crucial question. As we look at the issue of stigma, we need to recognize that there are structural issues in how our society is prioritizing the importance of substance use disorders and the investments devoted to them. And we need to recognize that substance use disorder doesn’t exist in isolation; it is frequently comorbid with mental illness.
We need to listen. Some of the issues that we believe are most problematic are not. We need to empower these communities to speak up and help them do so. This is probably one of the most important things that we can do in terms of addressing stigma for addiction.
Collins: Absolutely. The HEAL Initiative has a number of projects that are focusing on stigma and coming up with tools to help reduce this. And here’s our second question: “In small communities, how can we provide more access to medications for opioid use disorder?”
Volkow: One project funded through HEAL was to evaluate the effectiveness of community pharmacies for delivering buprenorphine to individuals with opioid use disorder. The results show that patients receiving buprenorphine through community pharmacies in rural areas had as good outcomes as patients being treated by specialized clinicians on site.
Another change that’s made things easier is that in March 2020, the DEA relaxed its rules on how a physician can prescribe buprenorphine. In the past, you needed to go physically to see a doctor. Now, the DEA allows a patient to be initiated on buprenorphine through telehealth, and that’s opened the possibility of greater access to treatment in rural communities.
My perspective is let’s look at innovative ways of solving problems. Because the technology is changing in so many ways and so rapidly, let’s take advantage of it.
Collins: Totally with you on that. If there’s a silver lining to COVID-19, it’s that we’ve been forced to take stock of the ways we’ve been doing things. We will learn from this pandemic and change the way we approach so many things in health and medicine as a result. Certainly, opioid use disorder ought to be very high on that list. Let’s move on to another question: “What is the HEAL initiative doing to promote prevention of opioid use?”
Volkow: This is where the HEAL initiative is aiming to provide alternative treatments for the management of pain that reduce the risk of addiction.
Then there’s the issue of prevention in people who start to take opioids because they either want to get high or escape. With the COVID pandemic, we’ve seen increases in anxiety and in depression. Those are factors that can put a teenager or young adult on a trajectory for higher risk of substance use disorders.
So, what is HEAL doing? There is prevention research specifically targeted, for example, at the transition from adolescence to young adulthood. That is the period of greatest vulnerability of uptake of opioids, or drugs of misuse. We’re also targeting minority groups that may be at very, very high risk. We want to be able to understand the factors that make them more vulnerable to tailor prevention interventions more effectively.
Collins: Today, we’ve shared some of the issues that NIH is wrestling with in its efforts to address the crisis of opioid misuse and overdose, as well as other drugs that are now very much part of the challenge. To learn more, go to the HEAL website. You can also send us your thoughts through the HEAL Idea Exchange.
These developments give me hope in the wake of a very difficult year. Clearly, we still have the capacity to work together, we are resilient, and we are determined to put an end to our nation’s opioid crisis.
Volkow: Francis, I want to thank you for your incredible leadership and your support. I hope the COVID pandemic will bring forth a more equitable system, in which all people are given the chance for resilience that maximizes their life, happiness, and productivity. I think science is an extraordinary tool to help us do that.
Links:
Video: The 2021 Rx Drug Abuse & Heroin Summit: Francis Collins with Nora Volkow (NIH)
COVID-19 Research (NIH)
Helping to End Addiction Long-term (HEAL) Initiative (NIH)
HEAL Idea Exchange (NIH)
National Institute on Drug Abuse (NIH)
Could CRISPR Gene-Editing Technology Be an Answer to Chronic Pain?
Posted on by Dr. Francis Collins

Gene editing has shown great promise as a non-heritable way to treat a wide range of conditions, including many genetic diseases and more recently, even COVID-19. But could a version of the CRISPR gene-editing tool also help deliver long-lasting pain relief without the risk of addiction associated with prescription opioid drugs?
In work recently published in the journal Science Translational Medicine, researchers demonstrated in mice that a modified version of the CRISPR system can be used to “turn off” a gene in critical neurons to block the transmission of pain signals [1]. While much more study is needed and the approach is still far from being tested in people, the findings suggest that this new CRISPR-based strategy could form the basis for a whole new way to manage chronic pain.
This novel approach to treating chronic pain occurred to Ana Moreno, the study’s first author, when she was a Ph.D. student in the NIH-supported lab of Prashant Mali, University of California, San Diego. Mali had been studying a wide range of novel gene- and cell-based therapeutics. While reading up on both, Moreno landed on a paper about a mutation in a gene that encodes a pain-enhancing protein in spinal neurons called NaV1.7.
Moreno read that kids born with a loss-of-function mutation in this gene have a rare condition known as congenital insensitivity to pain (CIP). They literally don’t sense and respond to pain. Although these children often fail to recognize serious injuries because of the absence of pain to alert them, they have no other noticeable physical effects of the condition.
For Moreno, something clicked. What if it were possible to engineer a new kind of treatment—one designed to turn this gene down or fully off and stop people from feeling chronic pain?
Moreno also had an idea about how to do it. She’d been working on repressing or “turning off” genes using a version of CRISPR known as “dead” Cas9 [2]. In CRISPR systems designed to edit DNA, the Cas9 enzyme is often likened to a pair of scissors. Its job is to cut DNA in just the right spot with the help of an RNA guide. However, CRISPR-dead Cas9 no longer has any ability to cut DNA. It simply sticks to its gene target and blocks its expression. Another advantage is that the system won’t lead to any permanent DNA changes, since any treatment based on CRISPR-dead Cas9 might be safely reversed.
After establishing that the technique worked in cells, Moreno and colleagues moved to studies of laboratory mice. They injected viral vectors carrying the CRISPR treatment into mice with different types of chronic pain, including inflammatory and chemotherapy-induced pain.
Moreno and colleagues determined that all the mice showed evidence of durable pain relief. Remarkably, the treatment also lasted for three months or more and, importantly, without any signs of side effects. The researchers are also exploring another approach to do the same thing using a different set of editing tools called zinc finger nucleases (ZFNs).
The researchers say that one of these approaches might one day work for people with a large number of chronic pain conditions that involve transmission of the pain signal through NaV1.7. That includes diabetic polyneuropathy, sciatica, and osteoarthritis. It also could provide relief for patients undergoing chemotherapy, along with those suffering from many other conditions. Moreno and Mali have co-founded the spinoff company Navega Therapeutics, San Diego, CA, to work on the preclinical steps necessary to help move their approach closer to the clinic.
Chronic pain is a devastating public health problem. While opioids are effective for acute pain, they can do more harm than good for many chronic pain conditions, and they are responsible for a nationwide crisis of addiction and drug overdose deaths [3]. We cannot solve any of these problems without finding new ways to treat chronic pain. As we look to the future, it’s hopeful that innovative new therapeutics such as this gene-editing system could one day help to bring much needed relief.
References:
[1] Long-lasting analgesia via targeted in situ repression of NaV1.7 in mice. Moreno AM, Alemán F, Catroli GF, Hunt M, Hu M, Dailamy A, Pla A, Woller SA, Palmer N, Parekh U, McDonald D, Roberts AJ, Goodwill V, Dryden I, Hevner RF, Delay L, Gonçalves Dos Santos G, Yaksh TL, Mali P. Sci Transl Med. 2021 Mar 10;13(584):eaay9056.
[2] Nuclease dead Cas9 is a programmable roadblock for DNA replication. Whinn KS, Kaur G, Lewis JS, Schauer GD, Mueller SH, Jergic S, Maynard H, Gan ZY, Naganbabu M, Bruchez MP, O’Donnell ME, Dixon NE, van Oijen AM, Ghodke H. Sci Rep. 2019 Sep 16;9(1):13292.
[3] Drug Overdose Deaths. Centers for Disease Control and Prevention.
Links:
Congenital insensitivity to pain (National Center for Advancing Translational Sciences/NIH)
Opioids (National Institute on Drug Abuse/NIH)
Mali Lab (University of California, San Diego)
Navega Therapeutics (San Diego, CA)
NIH Support: National Human Genome Research Institute; National Cancer Institute; National Institute of General Medical Sciences; National Institute of Neurological Disorders and Stroke
Addressing the Twin Challenges of Substance Use Disorders and COVID-19
Posted on by Dr. Francis Collins

The coronavirus disease 2019 (COVID-19) pandemic is having a wide range of negative impacts on people affected by a variety of health conditions. Among the hardest hit are individuals struggling with substance use disorders, with recent data indicating that suspected drug-related overdoses and deaths are on the rise across the United States [1].
One recent analysis of nationwide surveillance data, collected by the federal Overdose Detection Mapping and Application Program, found that suspected drug overdoses rose by 18 percent in March, 29 percent in April, and 42 percent in May compared to the same months in 2019 [2]. Another analysis of state and local mortality data showed that drug-related deaths have increased about 13 percent so far this year, compared to last year [3].
To find out what may be contributing to this tragic situation and learn what NIH-funded research is doing to help, I recently had a conversation with Dr. Nora Volkow, Director of NIH’s National Institute on Drug Abuse (NIDA). Here’s a condensed version of our interview, which took place via videoconference, with both of us linking in from our homes near NIH’s main campus in Bethesda, MD
Collins: Here we are today talking about two public health crises: the crisis of COVID-19 and another crisis that has been going on for quite some time, of drug overdoses and drug deaths. The opioid crisis is difficult in any circumstance, but when you add to it what’s happening right now with the global COVID-19 pandemic, it becomes difficult squared. What has happened during this pandemic?
Volkow: One of the first things that we’ve heard from the communities and the families afflicted by addiction is that the support systems that were there to help people achieve recovery are no longer present. At the same time, it’s been much harder to get access to some of the treatment programs, including hospital emergency departments that can initiate treatment. It’s also been more difficult to access syringe exchange programs and programs, like Narcotics Anonymous, that provide people with a mentor and a social support system that’s fundamental for recovery. Part of recovery is also for individuals to work at re-building their lives, and that too has become much more challenging due to the threat of COVID-19.
All of these aspects are translating into much more stress. And stress, as we know, is one of the factors that leads people to relapse. Stress is also a factor that leads many to increase the consumption of drugs.
Collins: What about the impact of the stay-at-home orders for people who are depending on social networks? You’ve talked about Narcotics Anonymous as an example. But for anybody who’s faced stress challenges, mental health issues, which often coexist with drug problems, what’s the effect of losing those face-to-face social connections?
Volkow: Isolation is difficult for anyone. We depend on others for our wellbeing. The harder our situation, the more vulnerable we are if we don’t have those support systems.
One of the major concerns that we’ve had all along is not just the enormous risk of relapse in many people, but also the risk of suicide—which is always much higher in individuals that are addicted to drugs, particularly to opioids. Indeed, there’s been an increase in the number of suicides associated with the COVID-19 pandemic, including among people that are addicted.
One of the elements we are using to try to overcome that is virtual interactions, like we are having right now. They are fulfilling, certainly for me. And when we’ve surveyed patients and families to see how much these virtual support systems are helping them, we see in many instances that this can be lifesaving. For example, with telehealth, a physician now can prescribe buprenorphine [a treatment medication] without necessarily having to see the individual physically. That’s a major breakthrough because it expands the number of people that can be treated. So, you can provide buprenorphine, and you can also provide support that someone with co-morbid mental illness may need. It’s not the same as physically being with others, but we have to recognize virtual technologies may enable greater equity in providing treatments.
Collins: What’s happened to methadone clinics, a place where people were required to show up in person every day? What’s become of people who depended on those?
Volkow: These spaces are small and there’s not enough staff, so it was very, very high risk. So, one of the positives of COVID-19 is that there was a change in the policy that enabled a methadone clinic to provide take-home methadone for patients, rather than have them come in daily and often at very restricted times, which made it incredibly difficult to comply.
We’re now trying to evaluate the outcomes when people are given take-home methadone. If we can show from evidence that the outcomes are as good as when you go in daily, then we hope that will help to transform these policies permanently.
Collins: So, there’s a silver lining in a few places. Are people who suffer from drug use disorders at increased risk of getting sick from COVID-19?
Volkow: There are many factors that place them at very, very high risk: pharmacological, structural, and social.
Pharmacological, because these drugs negatively affect multiple systems in your body and one of the main targets is the pulmonary system. If your pulmonary system already has pathology because of prior conditions, it’s much easier for the virus to actually infect you and lead to negative outcomes. That pertains to cigarette smoking that produces COPD and pulmonary damage, as well as to very toxic drugs like methamphetamine, which produces pulmonary hypertension; or opioids, which actually depress respiration and produce hypoxia.
You can see that the combination of depressed respiration and having a viral infection that attacks your lungs is not going to be positive. Indeed, it is very likely that that combination lowers the threshold for people to die from overdoses or to die from COVID-19. Drugs can also affect the cardiovascular system and the metabolic system, so all of the factors that we’ve identified as conditions that make you more vulnerable to COVID-19 are affected by drugs.
Then there are structural issues. We’ve already discussed methadone clinics, which put people together in very close spaces. Before COVID-19, one of our main priorities was to bring the treatment of substance use disorder and the screening into the healthcare system. But now the healthcare system is saturated and individuals who’ve gotten their treatment in healthcare systems no longer can access them and that restricts their ability to seek help. In our country, we basically criminalize people who take drugs, and many of them are in jail systems and prisons, where COVID-19 infections can rapidly occur. That is another element where they are at much higher risk.
Also, the number of individuals with substance use disorder who have medical insurance is much less than that of the general population. Not having such insurance is associated with a greater likelihood of having chronic medical conditions, which again is another risk factor for COVID-19. This mixes the structural with the social and, in the social category, you also have stigma.
Stigmatizing individuals with addiction makes them very vulnerable. That’s because, first of all, they are afraid to seek help—they don’t want to be discriminated against. Secondly, if they are in a situation where decisions are being made about providing medical care when resources are limited, that stigma can make them much more vulnerable.
While we are dealing with COVID-19, we cannot ignore the disparities that exist in our society. This pandemic has made it very clear how horrifically disparate health outcomes are between groups of people in our country.
Collins: Nora, you’ve been a real leader on what we might do to try to bring attention to helping people with drug use problems in the criminal justice system. This is often a point where an opportunity for treatment arises, but unfortunately that opportunity is often missed.
Volkow: One of our priorities as we address the opioid crisis is to do research in justice settings in order to be able to identify the models that lead to the best outcomes and to understand how to implement them. This has resulted in the creation of a research network that enables us to connect across the justice and the healthcare systems.
The network that started to emerge before COVID-19 hit has given us an opportunity to get direct information about what’s happening out there. From what we know, because prisons and jails are at such high risk for infection, many states—if not all—are releasing people that are not violent into their communities. Many of them have a substance use disorder. If someone has a long history of a substance use disorder, you cannot release them into the community without a support system, especially in the midst of the COVID-19 pandemic, where it’s hard to find a job and their families may be rejecting them. You can predict the outcome is going to be very poor, including dying from overdoses.
So, we now have a chance to show that treating these people in their community with appropriate support is going to lead to much better outcomes than leaving them in jail or prison. We are now working with our researchers and with appropriate agencies to figure out how to provide the support that’s necessary as individuals with substance use disorders are released into their communities. It can go both ways. Without support, the outcomes may be very poor. With support, we have the opportunity of transforming the way that we deal with addiction in this country.
Collins: A lot of people may not realize that effective medical treatment for substance use disorders does exist. Treatment has been demonstrated to change lives and improve outcomes over the long term. Still, a lot of folks out there think it’s just hopeless, or, alternatively, if someone just had a little bit more willpower, he or she would be able to take care of this. Please say a little bit about what the current treatment options are, and what the evidence is that they’re needed if you’re going to help somebody recover from a substance use disorder.
Volkow: There are medications for alcoholism and medications for nicotine use disorders. But, by far, the most effective medications are for opioid addiction. It’s very frustrating these medications are not necessarily given to patients—or sometimes even given to patients, but they reject them. I think part of the issue is because of the stigma against the medications. The opioid crisis has helped smooth that out somewhat, so there’s been a greater acceptance of medication. In partnership with the pharmaceutical industry, we have also been working towards developing extended-release formulations that make it much easier for people to take these medications.
In parallel, not just for opioid addiction, we have built up the scientific evidence for behavioral interventions that can improve outcomes for people with substance use disorder in general, if provided concurrently with medical treatment. Recognizing that there is a high risk of comorbidity with mental illness, we also need to provide treatments to address psychiatric disease problems or symptoms, as well as the addiction process. A lot of the work right now is going into creating models that allow this comprehensive treatment, tailored to the needs of the person.
Collins: Where can people who have a family member or friend who’s struggling with substance use disorder in the midst of COVID-19 go to get reliable evidence-based information about treatment programs?
Volkow: They can go to the NIDA website or the website of NIH’s sister agency, the Substance Abuse and Mental Health Services Administration (SAMHSA). One of the problems is that there hasn’t been any way of assessing the quality of treatment for substance use disorder. For many other conditions, you can check the track records of this or that hospital for this or that surgery, but such information does not exist for substance use disorder.
So, we’ve been funding researchers to develop metrics that can predict good outcomes in treatment programs. These metrics can be based on the experiences of people and family that actually took these services, and from the structural characteristics of the program, such as whether they have the evidence-based components shown by research to lead to better outcomes. Researchers are now developing “report cards” for treatment programs that hopefully will do two things: give a family member a sense of how others are rating a program, and, importantly, incentivize treatment programs to do better.
Collins: It would be wonderful to have more objective data for people searching for good answers. Now, let’s talk about HEAL, which stands for Helping to End Addiction Long-term. HEAL is a trans-agency initiative funded by the Congress to support research to address, from multiple different directions, multiple different problems relating to addiction and chronic pain.
How does the HEAL initiative need to adapt to the current health crisis of COVID-19? And what’s your institute doing to try to address some of the significant problems that have emerged in just the last two or three months?
Volkow: COVID-19 has placed HEAL and much of our other research on a very slow trajectory. For example, one program that we were very interested in expanding was the use of the emergency department for the screening of opioid use disorder and the initiation of treatment medications. Another major HEAL program was going to start using the justice system to conduct clinical trials to evaluate the outcomes of different types of medication for opioid use disorder. They are all basically on hold.
Collins: Nora, what’s your hope going forward over the next few months? What can NIH do to try to address this situation in the most effective way possible?
Volkow: I am optimistic because I can see how science can help to solve extremely challenging problems. I think this is the time for science to shine again and show us that methodologies aimed at gathering objective data to develop optimal solutions can resolve problems. But the question is: how long will it take?
I’ve been very impressed about how these devastating circumstances have led us to question the pace at which we moved projects in the past. I think it is wonderful that we have recognized that time is a luxury, that we need to move rapidly. With respect to the issue of substance use disorders, I would hope that, as we as a nation become aware of the suffering that the COVID-19 pandemic is putting on all of us, we become more empathetic to the suffering of others.
And as I see the movements across the country speaking out against injustice, I would hope that this will also extend to diseases that have been stigmatized. We need to modify our stigma so we provide the same level of importance to treating these diseases and supporting people afflicted by them.
I think that science will prevail. What is going to be important is that we also allow for our humanity in order to use that science in a way that everyone can take advantage of it.
Collins: That’s a wonderful way to wind up because I think the calling to bring together science and compassion is what drives all of us who have the privilege of working at NIH, the largest supporter of biomedical research in the world. Our purpose is clear: to find answers for all of these difficult problems that cause suffering and early death for people who deserve better.
Our vision is set on helping the most vulnerable populations right now. COVID-19 has pointed us toward that, and our discussion about those who suffer from substance use disorders also focuses on that.
I’m always one who likes to talk about hope, because, after all, that’s what we get up in the morning thinking about at NIH. We hope that our research efforts are going to lead to a new vaccine or a new treatment for COVID-19, or a better way of helping people who have been afflicted with drug problems.
Yet one of my favorite sayings is that “hope is a privilege that attaches to action.” This means that you can’t just say “Well, I hope for something,” unless you attach that hope to concrete actions you’re going to take.
Nora, your institute has been living that out. You don’t just hope that something good will happen to turn the tide of this terrible crisis of suffering and death from opioid overdoses, you’re all about action. So, thank you for your incredible dedication to the science and to the people whom we are trying to serve.
Volkow: Francis, thanks very much for your support.
References:
{1] Issue brief: Reports of increases in opioid-related overdose and other concerns during COVID pandemic, American Medical Association. Updated July 20, 2020
[2] “Cries for help’: Drug overdoses are soaring during the coronavirus pandemic.” William Wan, Healther Long. The Washington Post, July 1, 2020.
[3] “In the shadow of the pandemic, U.S. drug overdose deaths resurge to record.” Josh Katz, Abby Goodnough, Margot Sanger-Katz. July 15, 2020.
Links:
Coronavirus (COVID-19) (NIH)
Overdose Mapping Application Program (White House Office of National Drug Control Policy, Washington, D.C.)
Helping to End Addiction Long-term (HEAL) Initiative (NIH)
National Institute on Drug Abuse (NIH)
Video: Effects of COVID-19 on the Opioid Crisis: Francis Collins with Nora Volkow (National Institute on Drug Abuse/NIH)
Substance Abuse and Mental Health Services Administration (SAMHSA)
The Amazing Brain: Deep Brain Stimulation
Posted on by Dr. Francis Collins

August is here, and many folks have plans to enjoy a well-deserved vacation this month. I thought you might enjoy taking a closer look during August at the wonder and beauty of the brain here on my blog, even while giving your own brains a rest from some of the usual work and deadlines.
Some of the best imagery—and best science—comes from the NIH-led Brain Research through Advancing Innovative Neurotechnologies® (BRAIN) Initiative, a pioneering project aimed at revolutionizing our understanding of the human brain. Recently, the BRAIN Initiative held a “Show Us Your Brain Contest!”, which invited researchers involved in the effort to submit their coolest images. So, throughout this month, I’ve decided to showcase a few of these award-winning visuals.
Let’s start with the first-place winner in the still-image category. What you see above is an artistic rendering of deep brain stimulation (DBS), an approach now under clinical investigation to treat cognitive impairment that can arise after a traumatic brain injury and other conditions.
The vertical lines represent wire leads with a single electrode that has been inserted deep within the brain to reach a region involved in cognition, the central thalamus. The leads are connected to a pacemaker-like device that has been implanted in a patient’s chest (not shown). When prompted by the pacemaker, the leads’ electrode emits electrical impulses that stimulate a network of neuronal fibers (blue-white streaks) involved in arousal, which is an essential component of human consciousness. The hope is that DBS will improve attention and reduce fatigue in people with serious brain injuries that are not treatable by other means.
Andrew Janson, who is a graduate student in Christopher Butson’s NIH-supported lab at the Scientific Computing and Imaging Institute, University of Utah, Salt Lake City, composed this image using a software program called Blender. It’s an open-source, 3D computer graphics program often used to create animated films or video games, but not typically used in biomedical research. That didn’t stop Janson.
With the consent of a woman preparing to undergo experimental DBS treatment for a serious brain injury suffered years before in a car accident, Janson used Blender to transform her clinical brain scans into a 3D representation of her brain and the neurostimulation process. Then, he used a virtual “camera” within Blender to capture the 2D rendering you see here. Janson plans to use such imagery, along with other patient-specific modeling and bioelectric fields simulations, to develop a virtual brain stimulation surgery to predict the activation of specific fiber pathways, depending upon lead location and stimulation settings.
DBS has been used for many years to relieve motor symptoms of certain movement disorders, including Parkinson’s disease and essential tremor. More recent experimental applications include this one for traumatic brain injury, and others for depression, addiction, Alzheimer’s disease, and chronic pain. As the BRAIN Initiative continues to map out the brain’s complex workings in unprecedented detail, it will be exciting to see how such information can lead to even more effective applications of to DBS to help people living with a wide range of neurological conditions.
Links:
Deep Brain Stimulation for Movement Disorders (National Institute of Neurological Disorders and Stroke/NIH)
Video: Deep Brain Stimulation (University of Utah, Salt Lake City)
Deep Brain Stimulation for the Treatment of Parkinson’s Disease and Other Movement Disorders (NINDS/NIH)
Butson Lab (University of Utah)
Show Us Your Brain! (BRAIN Initiative/NIH)
Brain Research through Advancing Innovative Neurotechnologies® (BRAIN) Initiative (NIH)
NIH Support: National Institute of Neurological Disorders and Stroke
Easier Access to Naloxone Linked to Fewer Opioid Deaths
Posted on by Dr. Francis Collins

A few weeks ago, I was pleased to take part in the announcement of NIH’s HEALing Communities Study in four states hard hit by the opioid epidemic. This study will test a comprehensive, evidence-based approach—which includes the wide distribution of naloxone to reverse overdoses—with the aim of reducing opioid-related deaths in selected communities by 40 percent over three years.
That’s a very ambitious goal. So, I was encouraged to read about new findings that indicate such reductions may be within our reach if society implements a number of key changes. Among those is the need to arm friends, family members, and others with the ability to save lives from opioid overdoses. Between 2013 and 2016, nine states instituted laws that give pharmacists direct authority to dispense naloxone to anyone without a prescription. However, the impact of such changes has remained rather unclear. Now, an NIH-funded analysis has found that within a couple of years of these new laws taking effect, fatal opioid overdoses in these states fell significantly [1].
The misuse and overuse of opioids, which include heroin, fentanyl, and prescription painkillers, poses an unprecedented public health crisis. Every day, more than 130 people in the United States die from opioid overdoses [2]. Not only are far too many families losing their loved ones, this crisis is costing our nation tens of billions of dollars a year in lost productivity and added expenses for healthcare, addiction treatment, and criminal justice.
Opioid overdoses lead to respiratory arrest. If not reversed in a few minutes, this will be fatal. In an effort to address this crisis, the federal government and many states have pursued various strategies to increase access to naloxone, which is a medication that can quickly restore breathing in a person overdosing on opioids. Naloxone, which can be delivered via nasal spray or injection, works by binding opioid receptors to reverse or block the effect of opioids. The challenge is to get naloxone to those who need it before it’s too late.
In some states, a physician still must prescribe naloxone. In others, naloxone access laws (NALs) have given pharmacists the authority to supply naloxone without a doctor’s orders. But not all NALs are the same.
Some NALs, including those in Alaska, California, Connecticut, Idaho, New Mexico, North Dakota, Oklahoma, Oregon, and South Carolina, give pharmacists direct authority to dispense naloxone to anyone who requests it. But NALs in certain other states only give pharmacists indirect authority to dispense naloxone to people enrolled in certain treatment programs, or who meet other specific criteria.
In the new analysis, published in JAMA Internal Medicine, a team that included Rahi Abouk, William Paterson University, Wayne, NJ, and Rosalie Liccardo Pacula and David Powell, RAND Corp., Arlington, VA, asked: Do state laws to improve naloxone access lead to reductions in fatal overdoses involving opioids? The answer appears to be “yes,” but success seems to hinge on the details of those laws.
The evidence shows that states allowing pharmacists direct authority to dispense naloxone to anyone have seen large increases in the dispensing of the medication. In contrast, states granting pharmacists’ only indirect authority to dispense naloxone have experienced little change.
Most importantly, the research team found that states that adopted direct authority NALs experienced far greater reductions in opioid-related deaths than states with indirect authority NALs or no NALs. Specifically, the analysis showed that in the year after direct authority NALs were enacted, fatal opioid overdoses in those states fell an average of 27 percent, with even steeper declines in ensuing years. Longer-term data are needed, and, as in all observational studies of this sort, one must be careful not to equate correlation with causation. But these findings are certainly encouraging.
There were some other intriguing trends. For instance, the researchers found that states that allow pharmacists to dispense naloxone without a prescription also saw an increase in the number of patients treated at emergency departments for nonfatal overdoses. This finding highlights the importance of combining strategies to improve naloxone access with other proven interventions and access to medications aimed to treat opioid addiction. Integration of all possible interventions is exactly the goal of the HEALing Communities Study mentioned above.
Successfully tackling the opioid epidemic will require a multi-pronged approach, including concerted efforts and research advances in overdose reversal, addiction treatment, and non-addictive pain management . As I’ve noted before, we cannot solve the opioid addiction and overdose crisis without finding innovative new ways to treat pain. The NIH is partnering with pharmaceutical industry leaders to accelerate this process, but it will take time. The good news based on this new study is that, with thoughtful strategies and policies in place, many of the tools needed to help address this epidemic and save lives may already be at our disposal.
References:
[1] Association Between State Laws Facilitating Pharmacy Distribution of Naloxone and Risk of Fatal Overdose. Abouk R, Pacula RL, Powell D. JAMA Intern Med. 2019 May 6
[2] Opioid Overdose Crisis. National Institute on Drug Abuse/NIH. Updated January 2019.
Links:
HEAL (Helping to End Addiction Long-Term) Initiative (NIH)
Naloxone for Opioid Overdose (National Institute on Drug Abuse/NIH)
NIH Support: National Institute on Drug Abuse
Mood-Altering Messenger Goes Nuclear
Posted on by Dr. Francis Collins
Serotonin is best known for its role as a chemical messenger in the brain, helping to regulate mood, appetite, sleep, and many other functions. It exerts these influences by binding to its receptor on the surface of neural cells. But startling new work suggests the impact of serotonin does not end there: the molecule also can enter a cell’s nucleus and directly switch on genes.
While much more study is needed, this is a potentially groundbreaking discovery. Not only could it have implications for managing depression and other mood disorders, it may also open new avenues for treating substance abuse and neurodegenerative diseases.
To understand how serotonin contributes to switching genes on and off, a lesson on epigenetics is helpful. Keep in mind that the DNA instruction book of all cells is essentially the same, yet the chapters of the book are read in very different ways by cells in different parts of the body. Epigenetics refers to chemical marks on DNA itself or on the protein “spools” called histones that package DNA. These marks influence the activity of genes in a particular cell without changing the underlying DNA sequence, switching them on and off or acting as “volume knobs” to turn the activity of particular genes up or down.
The marks include various chemical groups—including acetyl, phosphate, or methyl—which are added at precise locations to those spool-like proteins called histones. The addition of such groups alters the accessibility of the DNA for copying into messenger RNA and producing needed proteins.
In the study reported in Nature, researchers led by Ian Maze and postdoctoral researcher Lorna Farrelly, Icahn School of Medicine at Mount Sinai, New York, followed a hunch that serotonin molecules might also get added to histones [1]. There had been hints that it might be possible. For instance, earlier evidence suggested that inside cells, serotonin could enter the nucleus. There also was evidence that serotonin could attach to proteins outside the nucleus in a process called serotonylation.
These data begged the question: Is serotonylation important in the brain and/or other living tissues that produce serotonin in vivo? After a lot of hard work, the answer now appears to be yes.
These NIH-supported researchers found that serotonylation does indeed occur in the cell nucleus. They also identified a particular enzyme that directly attaches serotonin molecules to histone proteins. With serotonin attached, DNA loosens on its spool, allowing for increased gene expression.
The team found that histone serotonylation takes place in serotonin-producing human neurons derived from induced pluripotent stem cells (iPSCs). They also observed this process occurring in the brains of developing mice.
In fact, the researchers found evidence of those serotonin marks in many parts of the body. They are especially prevalent in the brain and gut, where serotonin also is produced in significant amounts. Those marks consistently correlate with areas of active gene expression.
The serotonin mark often occurs on histones in combination with a second methyl mark. The researchers suggest that this double marking of histones might help to further reinforce an active state of gene expression.
This work demonstrates that serotonin can directly influence gene expression in a manner that’s wholly separate from its previously known role in transmitting chemical messages from one neuron to the next. And, there are likely other surprises in store.
The newly discovered role of serotonin in modifying gene expression may contribute significantly to our understanding of mood disorders and other psychiatric conditions with known links to serotonin signals, suggesting potentially new targets for therapeutic intervention. But for now, this fundamental discovery raises many more intriguing questions than it answers.
Science is full of surprises, and this paper is definitely one of them. Will this kind of histone marking occur with other chemical messengers, such as dopamine and acetylcholine? This unexpected discovery now allows us to track serotonin and perhaps some of the brain’s other chemical messengers to see what they might be doing in the cell nucleus and whether this information might one day help in treating the millions of Americans with mood and behavioral disorders.
Reference:
[1] Histone serotonylation is a permissive modification that enhances TFIID binding to H3K4me3. Farrelly LA, Thompson RE, Zhao S, Lepack AE, Lyu Y, Bhanu NV, Zhang B, Loh YE, Ramakrishnan A, Vadodaria KC, Heard KJ, Erikson G, Nakadai T, Bastle RM, Lukasak BJ, Zebroski H 3rd, Alenina N, Bader M, Berton O, Roeder RG, Molina H, Gage FH, Shen L, Garcia BA, Li H, Muir TW, Maze I. Nature. 2019 Mar 13. [Epub ahead of print]
Links:
Any Mood Disorder (National Institute of Mental Health/NIH)
Drugs, Brains, and Behavior: The Science of Addiction (National Institute on Drug Abuse/NIH)
Epigenomics (National Human Genome Research Institute/NIH)
Maze Lab (Icahn School of Medicine at Mount Sinai, New York, NY)
NIH Support: National Institute on Drug Abuse; National Institute of Mental Health; National Institute of General Medical Sciences; National Cancer Institute
Researchers Elucidate Role of Stress Gene in Chronic Pain
Posted on by Dr. Francis Collins

Credit: Getty Images/simonkr
For most people, pain eventually fades away as an injury heals. But for others, the pain persists beyond the initial healing and becomes chronic, hanging on for weeks, months, or even years. Now, we may have uncovered an answer to help explain why: subtle differences in a gene that controls how the body responds to stress.
In a recent study of more than 1,600 people injured in traffic accidents, researchers discovered that individuals with a certain variant in a stress-controlling gene, called FKBP5, were more likely to develop chronic pain than those with other variants [1]. These findings may point to new non-addictive strategies for preventing or controlling chronic pain, and underscore the importance of NIH-funded research for tackling our nation’s opioid overuse crisis.
All Scientific Hands on Deck to End the Opioid Crisis
Posted on by Dr. Nora Volkow and Dr. Francis Collins
 In 2015, 2 million people had a prescription opioid-use disorder and 591,000 suffered from a heroin-use disorder; prescription drug misuse alone cost the nation $78.5 billion in healthcare, law enforcement, and lost productivity. But while the scope of the crisis is staggering, it is not hopeless.
In 2015, 2 million people had a prescription opioid-use disorder and 591,000 suffered from a heroin-use disorder; prescription drug misuse alone cost the nation $78.5 billion in healthcare, law enforcement, and lost productivity. But while the scope of the crisis is staggering, it is not hopeless.
We understand opioid addiction better than many other drug use disorders; there are effective strategies that can be implemented right now to save lives and to prevent and treat opioid addiction. At the National Rx Drug Abuse and Heroin Summit in Atlanta last April, lawmakers and representatives from health care, law enforcement, and many private stakeholders from across the nation affirmed a strong commitment to end the crisis.
Research will be a critical component of achieving this goal. Today in the New England Journal of Medicine, we laid out a plan to accelerate research in three crucial areas: overdose reversal, addiction treatment, and pain management [1].
Widening Gap in U.S. Life Expectancy
Posted on by Dr. Francis Collins
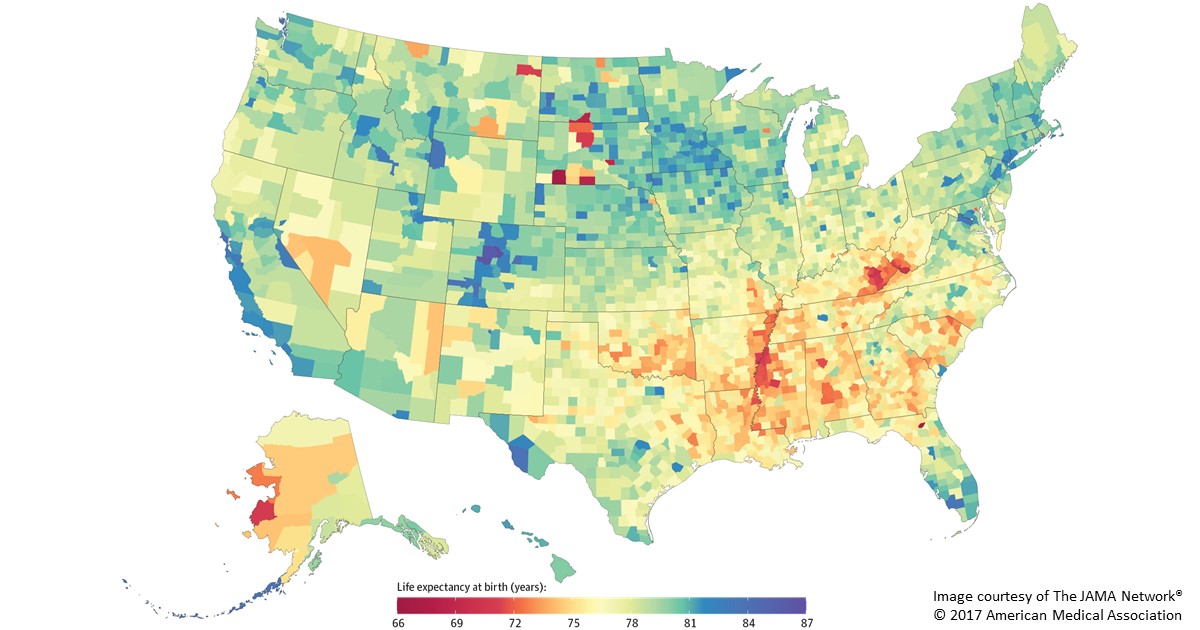
Caption: Life expectancy at birth by county, 2014. Life expectancy into 80s (blue), 70s (green, yellow, orange), 60s (red).
Americans are living longer than ever before, thanks in large part to NIH-supported research. But a new, heavily publicized study shows that recent gains in longevity aren’t being enjoyed equally in all corners of the United States. In fact, depending on where you live in this great country, life expectancy can vary more than 20 years—a surprisingly wide gap that has widened significantly in recent decades.
Researchers attribute this disturbing gap to a variety of social and economic influences, as well as differences in modifiable behavioral and lifestyle factors, such as obesity, inactivity, and tobacco use. The findings serve as a sobering reminder that, despite the considerable progress made possible by biomedical science, more research is needed to figure out better ways of addressing health disparities and improving life expectancy for all Americans.
In the new study published in JAMA Internal Medicine, a research team, partially funded by NIH, found that the average American baby born in 2014 can expect to live to about age 79 [1]. That’s up from a national average of about 73 in 1980 and around 68 in 1950. However, babies born in 2014 in remote Oglala Lakota County, SD, home to the Pine Ridge Indian Reservation, can expect to live only about 66 years. That’s in stark contrast to a child born about 400 miles away in Summit County, CO, where life expectancy at birth now exceeds age 86.
Cool Videos: Flashes of Neuronal Brilliance
Posted on by Dr. Francis Collins
When you have a bright idea or suddenly understand something, you might say that a light bulb just went on in your head. But, as the flashing lights of this very cool video show, the brain’s signaling cells, called neurons, continually switch on and off in response to a wide range of factors, simple or sublime.
The technology used to produce this video—a recent winner in the Federation of American Societies for Experimental Biology’s BioArt contest—takes advantage of the fact that whenever a neuron is activated, levels of calcium increase inside the cell. To capture that activity, graduate student Caitlin Vander Weele in Kay M. Tye’s lab at the Picower Institute for Learning and Memory, Massachusetts Institute of Technology (MIT), Cambridge, MA, engineered neurons in a mouse’s brain to produce a bright fluorescent signal whenever calcium increases. Consequently, each time a neuron was activated, the fluorescent indicator lit up and the changes were detected with a miniature microscope. The brighter the flash, the greater the activity!
Previous Page Next Page