vision loss
Metabolomics: A New Approach to Understanding Glaucoma
Posted on by Michael F. Chiang, M.D., National Eye Institute

Glaucoma remains one of the most common causes of vision loss and blindness in the U.S. and much of the world, disproportionately affecting older people, African Americans, and Hispanics and Latinos. Early signs of glaucoma can vary, from eye pressure to changes in the appearance of the optic nerve, and the disease can progress for years undetected while causing irreversible vision loss. More research is needed to understand the complex processes that underpin how glaucoma develops and progresses. If detected early enough, doctors can intervene and stop or slow its progression, thus preventing or minimizing vision loss.
While more than 120 genetic factors have been linked to glaucoma, these genes account for less than 10% of glaucoma cases. Scientists are exploring other ways to predict glaucoma, including studying metabolites to see if they hold any clues. These small molecules are produced by metabolism, including the breakdown of nutrients when we digest food or byproducts from the medicine we take. Identifying at-risk individuals based on their metabolic profile might present an opportunity to intercept disease before vision loss.
Researchers already use metabolites as biomarkers or indicators to help diagnose disease or assess disease risk. There’s a standard blood test called a comprehensive metabolic blood panel that doctors use to measure levels of metabolites circulating in your blood—sugars like glucose, minerals such as calcium, and proteins such as creatinine.
Your metabolome is the complete set of metabolites not in just your blood but in your entire body. National Eye Institute-funded researchers led by Louis Pasquale, Icahn School of Medicine at Mount Sinai, New York, in collaboration with Oana A. Zeleznik and Jae Hee Kang of Brigham and Women’s Hospital, Boston, recently explored 369 blood metabolites in relation to glaucoma in a large study.1
The research team examined blood that had been stored frozen from two long-term studies of health professionals: the Nurses’ Health Studies and the Health Professionals’ Follow-Up Study. They compared about 600 participants who had developed glaucoma after study enrollment to a group of similar participants who didn’t. On average, the participants who developed glaucoma did so about 10 years after their initial blood draw in the study.
The researchers found a particularly strong association between glaucoma and two classes of lipids (fats): triglycerides and diglycerides. Patients with elevated triglycerides and diglycerides were more likely to develop glaucoma, and the association was strongest in a subtype of glaucoma that causes early loss of central vision. They confirmed their findings in a cross-sectional analysis of data from the UK Biobank.
High levels of triglycerides have been linked to a variety of health problems, notably heart disease and stroke. The good news is that effective treatments to control triglyceride levels already exist. Statin drugs, for example, lower blood lipid levels. While studies looking at statin use and glaucoma risk have shown mixed results, we may learn that specific subtypes of glaucoma can be effectively controlled with statins. More research is needed to know if existing drugs might prevent glaucoma.
Pasquale’s work adds to a growing body of evidence that links health status to metabolism. Similar associations have been made between various metabolites and kidney cancer,2 pregnancy complications,3 type 2 diabetes,4 and Alzheimer’s disease.5 For researchers interested in exploring associations between metabolites and disease risk, the NIH Common Fund offers scientists a national and international repository for metabolomics data and metadata called the Metabolomics Workbench Metabolite Database, which contained more than 167,000 entries in 2022.
These findings and others offer the potential to prevent more and treat less. We urge anyone in an at-risk group, including people with a family history of glaucoma, to get regular, comprehensive eye exams.
References:
[1] OA Zeleznik, et al. Plasma metabolite profile for primary open-angle glaucoma in three US cohorts and the UK Biobank. Nature Communications DOI:10.1038/s41467-023-38466-x (2023)
[2] OO Bifarin, et al. Urine-Based Metabolomics and Machine Learning Reveals Metabolites Associated with Renal Cell Carcinoma Stage. Cancers (Basel) DOI:10.3390/cancers13246253 (2021)
[3] EW Harville, et al. Untargeted analysis of first trimester serum to reveal biomarkers of pregnancy complications: a case-control discovery phase study. Scientific Reports DOI:10.1038/s41598-021-82804-1 (2021)
[4] Nightingale Health Biobank Collaborative Group, et al. Metabolomic and genomic prediction of common diseases in 477,706 participants in three national biobanks. medRxiv DOI: 10.1101/2023.06.09.23291213 (2023). *note this article is a pre-print and is not peer-reviewed
[5] DK Barupal, et al. Sets of coregulated serum lipids are associated with Alzheimer’s disease pathophysiology. Alzheimer’s & Dementia: Diagnosis, Assessment & Disease Monitoring. DOI:10.1016/j.dadm.2019.07.002 (2019)
NIH Support: National Eye Institute, National Cancer Institute
Editor’s note: This blog post was updated on Jan. 18, 2024, to include Oana A. Zeleznik as one of the collaborators.
Finding Better Ways to Image the Retina
Posted on by Dr. Francis Collins
Every day, all around the world, eye care professionals are busy performing dilated eye exams. By looking through a patient’s widened pupil, they can view the retina—the postage stamp-sized tissue lining the back of the inner eye—and look for irregularities that may signal the development of vision loss.
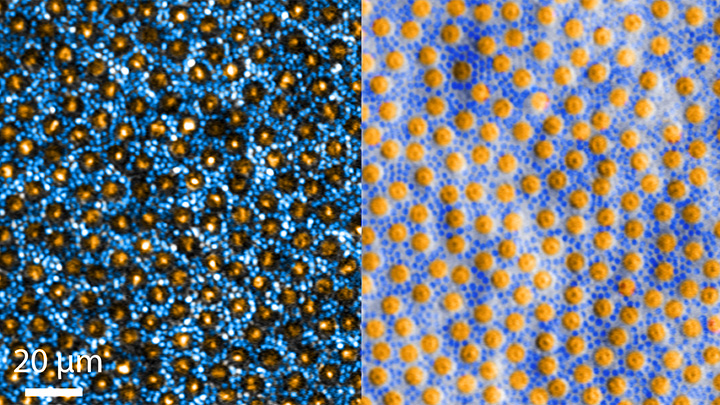
The great news is that, thanks to research, retinal imaging just keeps getting better and better. The images above, which show the same cells viewed with two different microscopic techniques, provide good examples of how tweaking existing approaches can significantly improve our ability to visualize the retina’s two types of light-sensitive neurons: rod and cone cells.
Specifically, these images show an area of the outer retina, which is the part of the tissue that’s observed during a dilated eye exam. Thanks to colorization and other techniques, a viewer can readily distinguish between the light-sensing, color-detecting cone cells (orange) and the much smaller, lowlight-sensing rod cells (blue).
These high-res images come from Johnny Tam, a researcher with NIH’s National Eye Institute. Working with Alfredo Dubra, Stanford University, Palo Alto, CA, Tam and his team figured out how to limit light distortion of the rod cells. The key was illuminating the eye using less light, provided as a halo instead of the usual solid, circular beam.
But the researchers’ solution hit a temporary snag when the halo reflected from the rods and cones created another undesirable ring of light. To block it out, Tam’s team introduced a tiny pinhole, called a sub-Airy disk. Along with use of adaptive optics technology [1] to correct for other distortions of light, the scientists were excited to see such a clear view of individual rods and cones. They published their findings recently in the journal Optica [2]
The resolution produced using these techniques is so much improved (33 percent better than with current methods) that it’s even possible to visualize the tiny inner segments of both rods and cones. In the cones, for example, these inner segments help direct light coming into the eye to other, photosensitive parts that absorb single photons of light. The light is then converted into electrical signals that stream to the brain’s visual centers in the occipital cortex, which makes it possible for us to experience vision.
Tam and team are currently working with physician-scientists in the NIH Clinical Center to image the retinas of people with a variety of retinal diseases, including age-related macular degeneration (AMD), a leading cause of vision loss in older adults. These research studies are ongoing, but offer hopeful possibilities for safe and non-intrusive monitoring of individual rods and cones over time, as well as across disease types. That’s obviously good news for patients. Plus it will help scientists understand how a rod or cone cell stops working, as well as more precisely test the effects of gene therapy and other experimental treatments aimed at restoring vision.
References:
[1] Noninvasive imaging of the human rod photoreceptor mosaic using a confocal adaptive optics scanning ophthalmoscope. Dubra A, Sulai Y, Norris JL, Cooper RF, Dubis AM, Williams DR, Carroll J. Biomed Opt Express. 2011 Jul 1;2(7):1864-76.
[1] In-vivo sub-diffraction adaptive optics imaging of photoreceptors in the human eye with annular pupil illumination and sub-Airy detection. Rongwen L, Aguilera N, Liu T, Liu J, Giannini JP, Li J, Bower AJ, Dubra A, Tam J. Optica 2021 8, 333-343. https://doi.org/10.1364/OPTICA.414206
Links:
Get a Dilated Eye Exam (National Eye Institute/NIH)
How the Eyes Work (NEI)
Eye Health Data and Statistics (NEI)
Tam Lab (NEI)
Dubra Lab (Stanford University, Palo Alto, CA)
NIH Support: National Eye Institute
Nano-Sized Solution for Efficient and Versatile CRISPR Gene Editing
Posted on by Dr. Francis Collins

Credit: Guojun Chen and Amr Abdeen, University of Wisconsin-Madison
If used to make non-heritable genetic changes, CRISPR gene-editing technology holds tremendous promise for treating or curing a wide range of devastating disorders, including sickle cell disease, vision loss, and muscular dystrophy. Early efforts to deliver CRISPR-based therapies to affected tissues in a patient’s body typically have involved packing the gene-editing tools into viral vectors, which may cause unwanted immune reactions and other adverse effects.
Now, NIH-supported researchers have developed an alternative CRISPR delivery system: nanocapsules. Not only do these tiny, synthetic capsules appear to pose a lower risk of side effects, they can be precisely customized to deliver their gene-editing payloads to many different types of cells or tissues in the body, which can be extremely tough to do with a virus. Another advantage of these gene-editing nanocapsules is that they can be freeze-dried into a powder that’s easier than viral systems to transport, store, and administer at different doses.
In findings published in Nature Nanotechnology [1], researchers, led by Shaoqin Gong and Krishanu Saha, University of Wisconsin-Madison, developed the nanocapsules with specific design criteria in mind. They would need to be extremely small, about the size of a small virus, for easy entry into cells. Their surface would need to be adaptable for targeting different cell types. They also had to be highly stable in the bloodstream and yet easily degraded to release their contents once inside a cell.
After much hard work in the lab, they created their prototype. It features a thin polymer shell that’s easily decorated with peptides or other ingredients to target the nanocapsule to a predetermined cell type.
At just 25 nanometers in diameter, each nanocapsule still has room to carry cargo. That cargo includes a single CRISPR/Cas9 scissor-like enzyme for snipping DNA and a guide RNA that directs it to the right spot in the genome for editing.
In the bloodstream, the nanocapsules remain fully intact. But, once inside a cell, their polymer shells quickly disintegrate and release the gene-editing payload. How is this possible? The crosslinking molecules that hold the polymer together immediately degrade in the presence of another molecule, called glutathione, which is found at high levels inside cells.
The studies showed that human cells grown in the lab readily engulf and take the gene-editing nanocapsules into bubble-like endosomes. Their gene-editing contents are then released into the cytoplasm where they can begin making their way to a cell’s nucleus within a few hours.
Further study in lab dishes showed that nanocapsule delivery of CRISPR led to precise gene editing of up to about 80 percent of human cells with little sign of toxicity. The gene-editing nanocapsules also retained their potency even after they were freeze-dried and reconstituted.
But would the nanocapsules work in a living system? To find out, the researchers turned to mice, targeting their nanocapsules to skeletal muscle and tissue in the retina at the back of eye. Their studies showed that nanocapsules injected into muscle or the tight subretinal space led to efficient gene editing. In the eye, the nanocapsules worked especially well in editing retinal cells when they were decorated with a chemical ingredient known to bind an important retinal protein.
Based on their initial results, the researchers anticipate that their delivery system could reach most cells and tissues for virtually any gene-editing application. In fact, they are now exploring the potential of their nanocapsules for editing genes within brain tissue.
I’m also pleased to note that Gong and Saha’s team is part of a nationwide consortium on genome editing supported by NIH’s recently launched Somatic Cell Genome Editing program. This program is dedicated to translating breakthroughs in gene editing into treatments for as many genetic diseases as possible. So, we can all look forward to many more advances like this one.
Reference:
[1] A biodegradable nanocapsule delivers a Cas9 ribonucleoprotein complex for in vivo genome editing. Chen G, Abdeen AA, Wang Y, Shahi PK, Robertson S, Xie R, Suzuki M, Pattnaik BR, Saha K, Gong S. Nat Nanotechnol. 2019 Sep 9.
Links:
Somatic Cell Genome Editing (NIH)
Saha Lab (University of Wisconsin-Madison)
Shaoqin (Sarah) Gong (University of Wisconsin-Madison)
NIH Support: National Eye Institute; National Institute of General Medical Sciences; National Institute of Neurological Disorders and Stroke; National Heart, Lung, and Blood Institute; Common Fund
The Amazing Brain: Making Up for Lost Vision
Posted on by Dr. Francis Collins
Recently, I’ve highlighted just a few of the many amazing advances coming out of the NIH-led Brain Research through Advancing Innovative Neurotechnologies® (BRAIN) Initiative. And for our grand finale, I’d like to share a cool video that reveals how this revolutionary effort to map the human brain is opening up potential plans to help people with disabilities, such as vision loss, that were once unimaginable.
This video, produced by Jordi Chanovas and narrated by Stephen Macknik, State University of New York Downstate Health Sciences University, Brooklyn, outlines a new strategy aimed at restoring loss of central vision in people with age-related macular degeneration (AMD), a leading cause of vision loss among people age 50 and older. The researchers’ ultimate goal is to give such people the ability to see the faces of their loved ones or possibly even read again.
In the innovative approach you see here, neuroscientists aren’t even trying to repair the part of the eye destroyed by AMD: the light-sensitive retina. Instead, they are attempting to recreate the light-recording function of the retina within the brain itself.
How is that possible? Normally, the retina streams visual information continuously to the brain’s primary visual cortex, which receives the information and processes it into the vision that allows you to read these words. In folks with AMD-related vision loss, even though many cells in the center of the retina have stopped streaming, the primary visual cortex remains fully functional to receive and process visual information.
About five years ago, Macknik and his collaborator Susana Martinez-Conde, also at Downstate, wondered whether it might be possible to circumvent the eyes and stream an alternative source of visual information to the brain’s primary visual cortex, thereby restoring vision in people with AMD. They sketched out some possibilities and settled on an innovative system that they call OBServ.
Among the vital components of this experimental system are tiny, implantable neuro-prosthetic recording devices. Created in the Macknik and Martinez-Conde labs, this 1-centimeter device is powered by induction coils similar to those in the cochlear implants used to help people with profound hearing loss. The researchers propose to surgically implant two of these devices in the rear of the brain, where they will orchestrate the visual process.
For technical reasons, the restoration of central vision will likely be partial, with the window of vision spanning only about the size of one-third of an adult thumbnail held at arm’s length. But researchers think that would be enough central vision for people with AMD to regain some of their lost independence.
As demonstrated in this video from the BRAIN Initiative’s “Show Us Your Brain!” contest, here’s how researchers envision the system would ultimately work:
• A person with vision loss puts on a specially designed set of glasses. Each lens contains two cameras: one to record visual information in the person’s field of vision; the other to track that person’s eye movements enabled by residual peripheral vision.
• The eyeglass cameras wirelessly stream the visual information they have recorded to two neuro-prosthetic devices implanted in the rear of the brain.
• The neuro-prosthetic devices process and project this information onto a specific set of excitatory neurons in the brain’s hard-wired visual pathway. Researchers have previously used genetic engineering to turn these neurons into surrogate photoreceptor cells, which function much like those in the eye’s retina.
• The surrogate photoreceptor cells in the brain relay visual information to the primary visual cortex for processing.
• All the while, the neuro-prosthetic devices perform quality control of the visual signals, calibrating them to optimize their contrast and clarity.
While this might sound like the stuff of science-fiction (and this actual application still lies several years in the future), the OBServ project is now actually conceivable thanks to decades of advances in the fields of neuroscience, vision, bioengineering, and bioinformatics research. All this hard work has made the primary visual cortex, with its switchboard-like wiring system, among the brain’s best-understood regions.
OBServ also has implications that extend far beyond vision loss. This project provides hope that once other parts of the brain are fully mapped, it may be possible to design equally innovative systems to help make life easier for people with other disabilities and conditions.
Links:
Age-Related Macular Degeneration (National Eye Institute/NIH)
Macknik Lab (SUNY Downstate Health Sciences University, Brooklyn)
Martinez-Conde Laboratory (SUNY Downstate Health Sciences University)
Show Us Your Brain! (BRAIN Initiative/NIH)
Brain Research through Advancing Innovative Neurotechnologies® (BRAIN) Initiative (NIH)
NIH Support: BRAIN Initiative
Regenerative Medicine: The Promise and Peril
Posted on by Dr. Francis Collins

Caption: Scanning electron micrograph of iPSC-derived retinal pigment epithelial cells growing on a nanofiber scaffold (blue).
Credit: Sheldon Miller, Arvydas Maminishkis, Robert Fariss, and Kapil Bharti, National Eye Institute/NIH
Stem cells derived from a person’s own body have the potential to replace tissue damaged by a wide array of diseases. Now, two reports published in the New England Journal of Medicine highlight the promise—and the peril—of this rapidly advancing area of regenerative medicine. Both groups took aim at the same disorder: age-related macular degeneration (AMD), a common, progressive form of vision loss. Unfortunately for several patients, the results couldn’t have been more different.
In the first case, researchers in Japan took cells from the skin of a female volunteer with AMD and used them to create induced pluripotent stem cells (iPSCs) in the lab. Those iPSCs were coaxed into differentiating into cells that closely resemble those found near the macula, a tiny area in the center of the eye’s retina that is damaged in AMD. The lab-grown tissue, made of retinal pigment epithelial cells, was then transplanted into one of the woman’s eyes. While there was hope that there might be actual visual improvement, the main goal of this first in human clinical research project was to assess safety. The patient’s vision remained stable in the treated eye, no adverse events occurred, and the transplanted cells remained viable for more than a year.
Exciting stuff, but, as the second report shows, it is imperative that all human tests of regenerative approaches be designed and carried out with the utmost care and scientific rigor. In that instance, three elderly women with AMD each paid $5,000 to a Florida clinic to be injected in both eyes with a slurry of cells, including stem cells isolated from their own abdominal fat. The sad result? All of the women suffered severe and irreversible vision loss that left them legally or, in one case, completely blind.
Snapshots of Life: Lighting up the Promise of Retinal Gene Therapy
Posted on by Dr. Francis Collins

Caption: Large-scale mosaic confocal micrograph showing expression of a marker gene (yellow) transferred by gene therapy techniques into the ganglion cells (blue) of a mouse retina.
Credit: Keunyoung Kim, Wonkyu Ju, and Mark Ellisman, National Center for Microscopy and Imaging Research, University of California, San Diego
The retina, like this one from a mouse that is flattened out and captured in a beautiful image, is a thin tissue that lines the back of the eye. Although only about the size of a postage stamp, the retina contains more than 100 distinct cell types that are organized into multiple information-processing layers. These layers work together to absorb light and translate it into electrical signals that stream via the optic nerve to the brain.
In people with inherited disorders in which the retina degenerates, an altered gene somewhere within this nexus of cells progressively robs them of their sight. This has led to a number of human clinical trials—with some encouraging progress being reported for at least one condition, Leber congenital amaurosis—that are transferring a normal version of the affected gene into retinal cells in hopes of restoring lost vision.
To better understand and improve this potential therapeutic strategy, researchers are gauging the efficiency of gene transfer into the retina via an imaging technique called large-scale mosaic confocal microscopy, which computationally assembles many small, high-resolution images in a way similar to Google Earth. In the example you see above, NIH-supported researchers Wonkyu Ju, Mark Ellisman, and their colleagues at the University of California, San Diego, engineered adeno-associated virus serotype 2 (AAV2) to deliver a dummy gene tagged with a fluorescent marker (yellow) into the ganglion cells (blue) of a mouse retina. Two months after AAV-mediated gene delivery, yellow had overlaid most of the blue, indicating the dummy gene had been selectively transferred into retinal ganglion cells at a high rate of efficiency [1].
Creative Minds: Reverse Engineering Vision
Posted on by Dr. Francis Collins
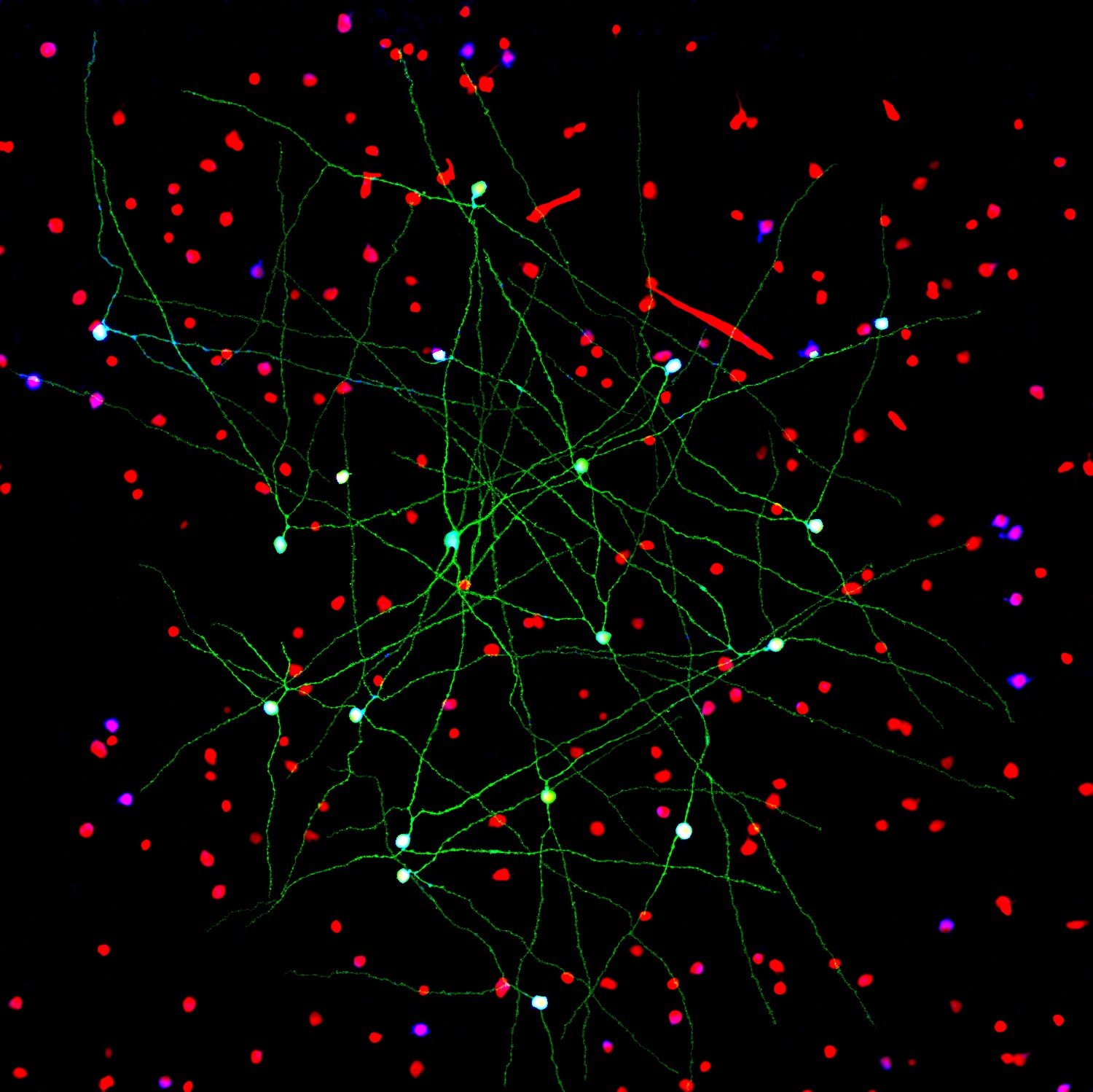
Caption: Networks of neurons in the mouse retina. Green cells form a special electrically coupled network; red cells express a distinctive fluorescent marker to distinguish them from other cells; blue cells are tagged with an antibody against an enzyme that makes nitric oxide, important in retinal signaling. Such images help to identify retinal cell types, their signaling molecules, and their patterns of connectivity.
Credit: Jason Jacoby and Gregory Schwartz, Northwestern University
For Gregory Schwartz, working in total darkness has its benefits. Only in the pitch black can Schwartz isolate resting neurons from the eye’s retina and stimulate them with their natural input—light—to get them to fire electrical signals. Such signals not only provide a readout of the intrinsic properties of each neuron, but information that enables the vision researcher to deduce how it functions and forges connections with other neurons.
The retina is the light-sensitive neural tissue that lines the back of the eye. Although only about the size of a postage stamp, each of our retinas contains an estimated 130 million cells and more than 100 distinct cell types. These cells are organized into multiple information-processing layers that work together to absorb light and translate it into electrical signals that stream via the optic nerve to the appropriate visual center in the brain. Like other parts of the eye, the retina can break down, and retinal diseases, including age-related macular degeneration, retinitis pigmentosa, and diabetic retinopathy, continue to be leading causes of vision loss and blindness worldwide.
In his lab at Northwestern University’s Feinberg School of Medicine, Chicago, Schwartz performs basic research that is part of a much larger effort among vision researchers to assemble a parts list that accounts for all of the cell types needed to make a retina. Once Schwartz and others get closer to wrapping up this list, the next step will be to work out the details of the internal wiring of the retina to understand better how it generates visual signals. It’s the kind of information that holds the key for detecting retinal diseases earlier and more precisely, fixing miswired circuits that affect vision, and perhaps even one day creating an improved prosthetic retina.
Guarding Against Glaucoma: What Can We Do?
Posted on by Dr. Francis Collins

This graph provides a frightening look at a problem that could threaten the vision of more than 6 million Americans by 2050: glaucoma. Glaucoma is a group of diseases that damage the eye’s optic nerve — a bundle of 1 million-plus nerve fibers connecting the light-sensitive retina to the brain — and that can lead to vision loss and blindness.
NIH research is trying to change this picture by developing better strategies for treatment and prevention. But you can also help. How? By getting your eyes checked regularly.

With early detection and treatment, serious vision loss can often be prevented. Anyone can develop glaucoma, but some folks are at higher risk:
- African Americans over age 40
- Everyone over age 60, especially Mexican Americans
- People with a family history of glaucoma
Glaucoma often has no symptoms until a lot of damage has already been done. So the best way to prevent a bad outcome from glaucoma is by undergoing a simple eye exam that can be done by an ophthalmologist or an optometrist — at least once every 2 years for people in high-risk groups.
Source: National Eye Institute, NIH