‘Decoy’ Protein Works Against Multiple Coronavirus Variants in Early Study
Posted on by Lawrence Tabak, D.D.S., Ph.D.
The NIH continues to support the development of some very innovative therapies to control SARS-CoV-2, the coronavirus that causes COVID-19. One innovative idea involves a molecular decoy to thwart the coronavirus.
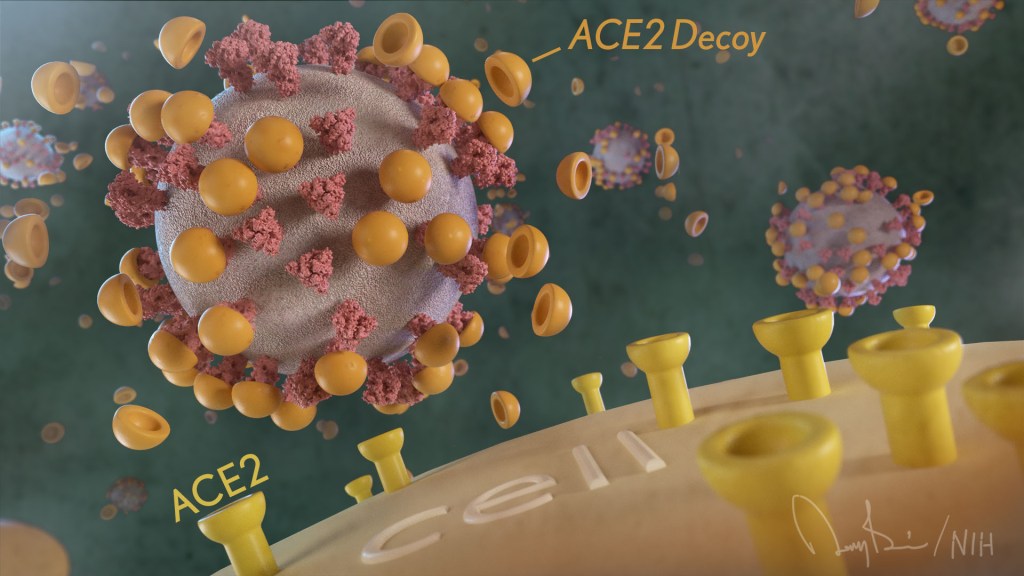
How’s that? The decoy is a specially engineered protein particle that mimics the 3D structure of the ACE2 receptor, a protein on the surface of our cells that the virus’s spike proteins bind to as the first step in causing an infection.
The idea is when these ACE2 decoys are administered therapeutically, they will stick to the spike proteins that crown the coronavirus (see image above). With its spikes covered tightly in decoy, SARS-CoV-2 has a more-limited ability to attach to the real ACE2 and infect our cells.
Recently, the researchers published their initial results in the journal Nature Chemical Biology, and the early data look promising [1]. They found in mouse models of severe COVID-19 that intravenous infusion of an engineered ACE2 decoy prevented lung damage and death. Though more study is needed, the researchers say the decoy therapy could potentially be delivered directly to the lungs through an inhaler and used alone or in combination with other COVID-19 treatments.
The findings come from a research team at the University of Illinois Chicago team, led by Asrar Malik and Jalees Rehman, working in close collaboration with their colleagues at the University of Illinois Urbana-Champaign. The researchers had been intrigued by an earlier clinical trial testing the ACE2 decoy strategy [2]. However, in this earlier attempt, the clinical trial found no reduction in mortality. The ACE2 drug candidate, which is soluble and degrades in the body, also proved ineffective in neutralizing the virus.
Rather than give up on the idea, the UIC team decided to give it a try. They engineered a new soluble version of ACE2 that structurally might work better as a decoy than the original one. Their version of ACE2, which includes three changes in the protein’s amino acid building blocks, binds the SARS-CoV-2 spike protein much more tightly. In the lab, it also appeared to neutralize the virus as well as monoclonal antibodies used to treat COVID-19.
To put it to the test, they conducted studies in mice. Normal mice don’t get sick from SARS-CoV-2 because the viral spike can’t bind well to the mouse version of the ACE2 receptor. So, the researchers did their studies in a mouse that carries the human ACE2 and develops a severe acute respiratory syndrome somewhat similar to that seen in humans with severe COVID-19.
In their studies, using both the original viral isolate from Washington State and the Gamma variant (P.1) first detected in Brazil, they found that infected mice infused with their therapeutic ACE2 protein had much lower mortality and showed few signs of severe acute respiratory syndrome. While the protein worked against both versions of the virus, infection with the more aggressive Gamma variant required earlier treatment. The treated mice also regained their appetite and weight, suggesting that they were making a recovery.
Further studies showed that the decoy bound to spike proteins from every variant tested, including Alpha, Beta, Delta and Epsilon. (Omicron wasn’t yet available at the time of the study.) In fact, the decoy bound just as well, if not better, to new variants compared to the original virus.
The researchers will continue their preclinical work. If all goes well, they hope to move their ACE2 decoy into a clinical trial. What’s especially promising about this approach is it could be used in combination with treatments that work in other ways, such as by preventing virus that’s already infected cells from growing or limiting an excessive and damaging immune response to the infection.
Last week, more than 17,500 people in the United States were hospitalized with severe COVID-19. We’ve got to continue to do all we can to save lives, and it will take lots of innovative ideas, like this ACE2 decoy, to put us in a better position to beat this virus once and for all.
References:
[1] Engineered ACE2 decoy mitigates lung injury and death induced by SARS-CoV-2 variants.
Zhang L, Dutta S, Xiong S, Chan M, Chan KK, Fan TM, Bailey KL, Lindeblad M, Cooper LM, Rong L, Gugliuzza AF, Shukla D, Procko E, Rehman J, Malik AB. Nat Chem Biol. 2022 Jan 19.
[2] Recombinant human angiotensin-converting enzyme 2 (rhACE2) as a treatment for patients with COVID-19 (APN01-COVID-19). ClinicalTrials.gov.
Links:
COVID-19 Research (NIH)
Accelerating COVID-19 Therapeutic Interventions and Vaccines (NIH)
Asrar Malik (University of Illinois Chicago)
Jalees Rehman (University of Illinois Chicago)
NIH Support: National Heart, Lung, and Blood Institute; National Institute of Allergy and Infectious Diseases
Hope this would work on the Omicron mutation. It is my understanding that the current monoclonal treatments have not been effective on that strain of C-19.
The monoclonal antibodies that had been used effectively prior to the Omicron variant do not neutralize Omicron. However, a newer one (sotrovimab) does work against it, as does a different one, Evusheld. Both are in very short supply at the moment.
Even though we did not study the efficacy against omicron in this paper, there is new data from our collaborators that the decoy also neutralizes the omicron variant. One of the reasons we were so interested in this research project is that the variants seem to bind the decoy we used even better because the decoy is engineered to outcompete the ACE2 receptor on cells. The contagious or aggressive variants are very good at binding ACE2 (this is why they enter the cells of our body so quickly) but the decoy we used leveraged this increased binding and “fooled” the contagious variants to bind the decoy even more.
I’m sorry but I know people who were helped greatly by the monoclonal antibodies. They say they didn’t work. They say they had side effects but I know people who are greatful they had them. I couldn’t get them. I’d like to know if this treatment is avaiiable under the ‘right to try’ as if I get covid again I’d like to try!
Thanks for this bit of potentially good news, and for continuing with an excellent feature.
Suggestion: the links for sharing this article are fine, but old-timers like me would appreciate
an email option.
Fantastic! Your research and dedication to solving this virus outbreak can’t properly be thanked.
How is the decoy cleared from body of patients?
Once the decoy binds the virus and prevents it from entering the cells, the virus-decoy complex remains in the blood and is recognized as well as eliminated by the immune system
Will the decoy protein not act as an antigen and elicit an immune response which may have untoward effects?
They saw no such effects in the mice they studied but, of course, that only gives a hint as to whether or not the same results would be seen in humans. That will have to be ascertained in human trials.
The immunogenicity is a good question which we did not address in the paper. But there are reasons to be hopeful that this decoy will have a low risk of provoking an immune response. It is based on an endogenous protein with very focused engineering so that the protein is likely still seen as part of the “self”. Additionally, immune reactions to therapeutic proteins occur during repeat treatments over many weeks and months. For treating COVID-19, the treatment duration will likely be short and focused (several days).
Decoy protein and Coronavirus-19 spike intersections warrant dynamic global collaborations with immunotherapeutic targeting of the enigmatic Toll-like Receptors and ACE-2 in genetically susceptible pooled population-subsets symptomatic of Omicron vs Delta variants in the Covid-19 vaccination era!
Ang 1-7 is a breakdown product of Ang-II. It is a specific ligand for the ACE-2 receptor. Lowers BP. Anti inflammatory effects. Can Ang 1-7 fragment block S spike binding at ACE-2R?
Thanks for this extraordinary therapeutic perspective, we hope that it will be available also outside the hospital environment.
One question:
In the study: “A Possible Role for Anti-idiotype Antibodies in SARS-CoV-2 Infection and Vaccination”
– William J. Murphy, Ph.D., and Dan L. Longo, M.D.-
the Authors report the presence and possible role of antibodies called Anti-idiotype Antibodies ( Ab2, produced both in SARS-CoV-2 Infection and in Vaccination):
“… “Ab2” antibodies that are specific for Ab1 can structurally resemble that of the original antigens themselves…”
“… Ab2 antibodies can bind to the protective neutralizing Ab1 antibody, resulting in immune-complex formation and clearance, thus impairing Ab1 efficacy. Some of the Ab2 binding regions, or paratopes, can also mirror the spike protein itself and bind to the same target as the spike protein, the ACE2 receptor..”
In all this strategic scenario of antibodies (Ab1 and Ab2), spike protein, ACE2 receptors and finally with these ACE2 decoys what result of immune complexes do we find?
Will an antibody titer test be considered useful if the patient has had a previous vaccination or covid infection with another viral variant? Also consider antiplatelet prophylaxis useful, especially in these cases?
I thank the Acting Director Dr. Tabak, who illustrates these fundamental efforts in the fight against SARS-CoV-2.
The cells of the mucous membranes of the digestive system widely express ACE2 receptors and many people who contract SARS-CoV-2, especially with Omicron, develop the unpleasant gastrointestinal symptoms.
This premise suggests the idea of soon having a formulation of the ACE2 Decoy, which can be administered orally: in this way, we could take it as a preventive measure whenever it is suspected of having been exposed to SARS-CoV-2, before it enters from the mucous membranes into the bloodstream.
I understand the need for ACE2 research in this direction. What I am wondering is if there is any research into actual ACE2 inhibitors, instead of just decoys, in the nasal passages specifically, to stop the infection from airborne spread?
ACE inhibitors are blood pressure drugs that primarily work on ACE1 (not so much on ACE2) but the virus uses ACE2 as a receptor to enter cells. The decoy approach has the advantange that it minimally affects normal functions of ACE1 and ACE2. Giving the decoy intranasally would be a very good approach to reduce viral entry into the nasal passage cells and therefore also reduce viral spreading.
Thank you for your reply! I am aware of the difference between ACE and ACE2. I am aware of ACE inhibitors for blood pressure and cardiology. I’m aware of the “yin yang” relationship between the two enzymes ACE and ACE2, and as far as I understand, if ACE is inhibited ACE2 can increase. My question remains, if there are ACE2 (not ACE) inhibitors that can be used for the nasal passages, or if any research is being done on this?
If this decoy can defeat Covid, then Omicron is possible, right?
When can we expect ACTIV-5 data? Stopping cytokine storms in my opinion is how we make Covid-19 manageable for the years to come.
What about spike proteins from the vaccines causing harm in the body? Why would this happen? How can it be addressed? No doctor has any answers or ways to treat it so far. Hoping if goes away.