How Immunity Generated from COVID-19 Vaccines Differs from an Infection
Posted on by Dr. Francis Collins
A key issue as we move closer to ending the pandemic is determining more precisely how long people exposed to SARS-CoV-2, the COVID-19 virus, will make neutralizing antibodies against this dangerous coronavirus. Finding the answer is also potentially complicated with new SARS-CoV-2 “variants of concern” appearing around the world that could find ways to evade acquired immunity, increasing the chances of new outbreaks.
Now, a new NIH-supported study shows that the answer to this question will vary based on how an individual’s antibodies against SARS-CoV-2 were generated: over the course of a naturally acquired infection or from a COVID-19 vaccine. The new evidence shows that protective antibodies generated in response to an mRNA vaccine will target a broader range of SARS-CoV-2 variants carrying “single letter” changes in a key portion of their spike protein compared to antibodies acquired from an infection.
These results add to evidence that people with acquired immunity may have differing levels of protection to emerging SARS-CoV-2 variants. More importantly, the data provide further documentation that those who’ve had and recovered from a COVID-19 infection still stand to benefit from getting vaccinated.
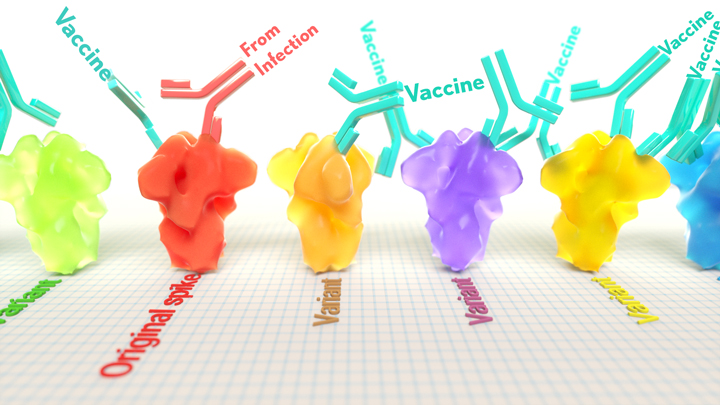
These latest findings come from Jesse Bloom, Allison Greaney, and their team at Fred Hutchinson Cancer Research Center, Seattle. In an earlier study, this same team focused on the receptor binding domain (RBD), a key region of the spike protein that studs SARS-CoV-2’s outer surface. This RBD is especially important because the virus uses this part of its spike protein to anchor to another protein called ACE2 on human cells before infecting them. That makes RBD a prime target for both naturally acquired antibodies and those generated by vaccines. Using a method called deep mutational scanning, the Seattle group’s previous study mapped out all possible mutations in the RBD that would change the ability of the virus to bind ACE2 and/or for RBD-directed antibodies to strike their targets.
In their new study, published in the journal Science Translational Medicine, Bloom, Greaney, and colleagues looked again to the thousands of possible RBD variants to understand how antibodies might be expected to hit their targets there [1]. This time, they wanted to explore any differences between RBD-directed antibodies based on how they were acquired.
Again, they turned to deep mutational scanning. First, they created libraries of all 3,800 possible RBD single amino acid mutants and exposed the libraries to samples taken from vaccinated individuals and unvaccinated individuals who’d been previously infected. All vaccinated individuals had received two doses of the Moderna mRNA vaccine. This vaccine works by prompting a person’s cells to produce the spike protein, thereby launching an immune response and the production of antibodies.
By closely examining the results, the researchers uncovered important differences between acquired immunity in people who’d been vaccinated and unvaccinated people who’d been previously infected with SARS-CoV-2. Specifically, antibodies elicited by the mRNA vaccine were more focused to the RBD compared to antibodies elicited by an infection, which more often targeted other portions of the spike protein. Importantly, the vaccine-elicited antibodies targeted a broader range of places on the RBD than those elicited by natural infection.
These findings suggest that natural immunity and vaccine-generated immunity to SARS-CoV-2 will differ in how they recognize new viral variants. What’s more, antibodies acquired with the help of a vaccine may be more likely to target new SARS-CoV-2 variants potently, even when the variants carry new mutations in the RBD.
It’s not entirely clear why these differences in vaccine- and infection-elicited antibody responses exist. In both cases, RBD-directed antibodies are acquired from the immune system’s recognition and response to viral spike proteins. The Seattle team suggests these differences may arise because the vaccine presents the viral protein in slightly different conformations.
Also, it’s possible that mRNA delivery may change the way antigens are presented to the immune system, leading to differences in the antibodies that get produced. A third difference is that natural infection only exposes the body to the virus in the respiratory tract (unless the illness is very severe), while the vaccine is delivered to muscle, where the immune system may have an even better chance of seeing it and responding vigorously.
Whatever the underlying reasons turn out to be, it’s important to consider that humans are routinely infected and re-infected with other common coronaviruses, which are responsible for the common cold. It’s not at all unusual to catch a cold from seasonal coronaviruses year after year. That’s at least in part because those viruses tend to evolve to escape acquired immunity, much as SARS-CoV-2 is now in the process of doing.
The good news so far is that, unlike the situation for the common cold, we have now developed multiple COVID-19 vaccines. The evidence continues to suggest that acquired immunity from vaccines still offers substantial protection against the new variants now circulating around the globe.
The hope is that acquired immunity from the vaccines will indeed produce long-lasting protection against SARS-CoV-2 and bring an end to the pandemic. These new findings point encouragingly in that direction. They also serve as an important reminder to roll up your sleeve for the vaccine if you haven’t already done so, whether or not you’ve had COVID-19. Our best hope of winning this contest with the virus is to get as many people immunized now as possible. That will save lives, and reduce the likelihood of even more variants appearing that might evade protection from the current vaccines.
Reference:
[1] Antibodies elicited by mRNA-1273 vaccination bind more broadly to the receptor binding domain than do those from SARS-CoV-2 infection. Greaney AJ, Loes AN, Gentles LE, Crawford KHD, Starr TN, Malone KD, Chu HY, Bloom JD. Sci Transl Med. 2021 Jun 8.
Links:
COVID-19 Research (NIH)
Bloom Lab (Fred Hutchinson Cancer Research Center, Seattle)
NIH Support: National Institute of Allergy and Infectious Diseases
I am fully vaccinated with Pfizer . I believe I have a breakthrough infection with possibly delta variant, but haven’t had a test to verify yet.
Will the antibodies generated by the breakthrough infection possibly function like a booster Pfizer is contemplating, much like for persons who had Covid 19 and then had full vaccinations later? Doesn’t seem to be much discussion or conjecture about this. I realize this is probably not studied yet, but am curios what you think these breakthrough infections could cause
When I had COVID back in February (not vaccinated as they were not even available then), I used the I-Mask+ protocol and my symptoms were extremely mild (like a cold with a 99 degree temperature). My husband didn’t even have any temp – just felt a bit unwell. No headaches, loss of smell or taste, etc. and no long-term issues at all. Early treatment is important!! Right now the data coming out of Israel indicates a reinfection rate of 0.0086% for previously infected individuals. No one knows how long the immunity will last, but so far it looks to be great protection. I also wish there was more study on this issue as it affects MILLIONS of us! Best wishes to you for a super speedy recovery.
Joanne I agree with you. Why are other countries studying Natural Immunity and the US is not?
Lisa – I wish the NIH/CDC would realize that THIS issue – that the natural immunity of MILLIONS of Americans is not recognized and people who have previously recovered are being FORCED to accept shots that numerous studies have shown offer no demonstrated benefit or lose their employment, access to education, and/or loss of freedom due to their recommendations – is what is causing so much distrust for the government. There needs to be a risk versus reward analysis done on this issue. Yes, vaccination in the previously infected causes an increase in CERTAIN antibodies, but does this really offer any benefit, especially in light of the increasing amount of Delta variant breakthrough cases? Real-life results seems to indicate it does not. At the same time, “Self-reported real-world safety and reactogenicity of COVID-19 vaccines: An international vaccine-recipient survey” shows an increased incidence of vaccination side effects by 2-3 times. It all just doesn’t make any sense. I am against mandates in general, but Certificates of Recovery could easily be issued to recovered individuals, even if for just a specified period of time until more data comes in. Europe is currently offering these to individuals for a six-month period after recovery (and they state that amount of time may increase as more data becomes available). Additionally, this would free up vaccine doses for other underserved areas of the world. Isn’t it just selfish not to direct the resources towards the most needy?
I agree 100% with all you’ve stated. I had no idea that Europe was offering the Certificate of Recovery. It would make so much sense to monthly or quarterly test recovered covid patients for antibody levels. I still can not taste and smell 7 months after having covid. The last thing I want to do right now when I feel I am still recovering is to be forced or shamed into taking a vaccine that is made up of a chemical compound that my body reacts to.
I agree. I came across information about the Certificate of Recovery on the EU Commission site last week. Ireland went so far as to recommend 9 months but I think they are going with the six months like other EU (27 countries) and EEA.
The Commission also proposed that people who have received a single dose of a two-dose vaccine after having previously been infected with COVID-19 should be considered fully vaccinated for the purpose of travel.
This is based on multiple studies and at least 640,000 participants. Why is the conversation and the guidance for those who have recovered not given serious time and attention. It’s always, just get the vaccine.
” …….This is based on multiple studies and at least 640,000 participants. Why is the conversation and the guidance for those who have recovered not given serious time and attention. It’s always, just get the vaccine…………” Isn’t that most curious? Somehow the brilliant medical authorities heading our nations health bureaucracies have either not noticed or considered the immunity of the recovered, or maybe more likely, decided to put a lid on that discussion. It is impossible to look at that logically and not suspect something nefarious going on. Exactly what, I do not know. All I know is that they are blatantly ignoring the science by ignoring those of us who have survived the disease and our resulting immunity to COVID-19. It is not right or ethical for them to ignore it, but that is exactly what is happening.
I concur with you JR. Why are our blood types not being studied as Diana stated and why is our blood not being used to create new safer vaccines with known natural antibodies instead of chemical compounds made to replicate the virus?
Joanne, One additional thing I found interesting from the Israeli study I didn’t seen your comment is that vaccinated people are almost 7 times more likely to become reinfected than those who have natural immunity. Like with most viruses, natural immunity appears to be stronger and longer lasting then the vaccination. I think there must be a political component To why natural immunity is not being recognized like vaccines are.
Ryan – Agreed it must be political as all the recent data coming out supports the notion that natural immunity is AT LEAST as good as vaccination (it actually appears that natural is indeed much better, but I will even accept “as good as” recognition). So many of us put ourselves out there as first responders, kept the country running, got sick and recovered, and now get nothing for our sacrifice. Instead, we get bombarded with mandates which should not apply to us. All the recent data indicates we are much less of a risk to others than the vaccinated. Meanwhile, our doses could be sent to other countries to help with the overall global situation. The whole thing just makes no logical sense!!
I agree with all of you. I had severe COVID this past January, At that time vaccines were just coming into view. I have written to the CDC & WHO. Never got an answer. However, as you all have stated, recovery from COVID is not recognized here in the USA. All we ever hear is vaccine, vaccine, vaccine. This week it’s being said if you are not completely vaccinated, you will be punished (it wasn’t said in that way) But, without proof of vaccines, you might lose your job. All federal employees must be vaccinated, Everyone in the medical field everywhere (even if you have recovered from Covid & have positive test to SARS-COV-2 (covid-19) In New York city, you can not eat indoors, cannot go to the gym, movies, stadium & other things I can’t remember (I have a covid memory) if you are not fully vaccinated (2 vaccines,not1)
I can’t even show proof of having a positive response to sars-cov-2. They only want proof of having the vaccines.
I love the sound of a “certificate of recovery” How do we get it?
I want to add to this discussion a recently published medical article that appeared in The Lancet entitled, “Correlates of protection from SARS-CoV-2 infection.” To summarize this: “The findings of the authors suggest that infection and the development of an antibody response provides protection similar to or even better than currently used SARS-CoV-2 vaccines. Although antibodies induced by SARS-CoV-2 infection are more variable and often lower in titre than antibody responses induced after vaccination, this observation does make sense considering current SARS-CoV-2 vaccines induce systemic immune responses to spike proteins while natural infection also induces mucosal immune responses and immune responses against the many other open reading frames encoded by the approximately 29,900 nucleotides of SARS-CoV-2. The SIREN study adds to a growing number of studies, which demonstrate that infection does protect against reinfection, and probably in an antibody-dependent manner.” . . .
The article you cited is an editorial commenting on a study in The Lancet titled, “SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: a large, multicentre, prospective cohort study (SIREN).” Both were dated April 9, 2021. The study involved assessing participants between June 18, 2020, and Jan 11, 2021. The only variant for which protection was assessed (in addition to the original strain) was the Alpha variant.
The Beta, Gamma and (most notably) Delta variants were not assessed in this study, as they were not detected in the participants during the study. Since these variants have shown some increased ability to evade immune protection, this study, while helpful, is a bit out of date, as the Delta variant is so dominant in the world now.
Additionally, while it was good to see that natural immunity provided significant protection against reinfection, it wasn’t the near-invulnerable shield some portray it to be. From the original Lancet study cited above, “A previous history of SARS-CoV-2 infection was associated with an 84% lower risk of infection, with median protective effect observed 7 months following primary infection.” That means, of course, that there was a 16% risk of reinfection, with some of those reinfections occurring less than 7 months after the initial infection.
With the Delta variant so dominant now, those numbers for reinfection risk likely are even lower than they were at the end of the study almost 7 months ago. While the odds of reinfection likely remain low, my guess is that they are not as good as they had been (very good, but not fantastic).
The bottom line is that natural immunity is at least as robust as, and likely superior to, vaccinated immunity. That is very well established now with the multiple studies indicating that to be the case, and with ZERO studies showing vaccinated immunity superior to natural immunity. This only reinforces what common sense tells us, namely, that if you only recognize a hand of someone you are looking for, that is inferior to recognizing the whole person. Those of use who have recovered from COVID-19 have immune systems that have met the WHOLE GERM as opposed to those who have vaccinated immunity in which their immune systems have only met a simulated hand of the germ. It’s not hard to understand which immunity would be superior . . .
I disagree about your bottom line. The concern is not which immunity is better, the real concern (“bottom line,” if you wish) is whether the likelihood of a reinfection is trivial, whether vaccination in someone having suffered a previous infection is worthwhile.
For a 16% risk at a median of 7 months, that is not trivial. Those who have had an infection are not immune from reinfection as the cited study shows, and the 16% figure was at only 7 months. What is the risk at 12 months? Almost certainly greater than 16%.
The “bottom line” is those who have unfortunately been infected with SARS-CoV-2 face a real risk of reinfection and should be vaccinated, for their sakes and for the sakes of their communities.
Please do not spread this false information, especially on a valuable site like the NIH site, where you could be confusing people who think your posts are coming from fact (which the article has, but your responses to it do not)…
Everyone needs to get vaccinated to reduce the planeload full of people that are dying in the United States every day. This will reduce the 97-99% of cases that are happening by the ~50% of people that haven’t been vaccinated yet. If everyone was vaccinated, we’d have 97-99% less deaths every day… and that would soon reduce to less than a car load of people dying every day through needless confusion as prompted by misleading comments like yours.
Agreed on all points. Additionally, for those like myself who have recovered from COVID-19 (validated by a positive COVID test and a following positive antigen test), it’s easy enough to base the Certificate of Recovery date on a 6 month time frame, and test again at 6 months for the antibodies.
Joanne, they have… google this on NIH website: nih-research-matters – lasting-immunity-found-after-recovery-covid-19. I had it in November and had Antibodies, confirmed by blood test as of late July.
WOW I didn’t know that either. 18 of us in our family had covid in December 2020, beginning of, and we’re all fine. We will not get a vaccine as we know and believe our immunity is for sure stronger than those out there getting vaccinated. I’ve had too many friends recently who’ve been vaccinated, got severely sick and were in ICU. They just got out this week from hospital.
My question, with Lambda variant not being stopped by vaccines at all, and the new push for natural immunity to be boosted by a shot, is my natural immunity no longer going to stop variants? will it make my natural antibodies more synthetic in nature?
🎯 Yes!!!
antibody mediated viral enhancement Joanne – this is why with vaccine Israeli study indicates greater chance of reinfection.
Also, the vaccine is a hedge and also a status symbol in many ways. This entire mismanagement of the pandemic is widespread but as always, each individual must have the discernment to make decisions for them and their loved ones. Another huge problem is the false sense of security from the vacc. I know people that got it and are out and about, I have not taken it but my moves are still the same even before covid, I was a bit on the compulsive side of sanitation.
. . . Now there is a T-cell test that can show immunity (natural or vaccine induced). It infuriates me everyday that our CDC and government officials continue to ignore the mounting evidence and science that natural immunity obtained by recovering from covid is just as good, possibly better than, vaccine induced immunity. Especially with the onset of the Delta variant! So many “breakthrough” cases of fully vaccinated people meanwhile covid reinfection for people who who have already recovered from the virus is extremely rare. This is also supported by the studies out of Israel. It should no longer be “vaccinated” or “not vaccinated” but rather “immune or “not immune”. Being able to show proof of having been recovered from covid, either by showing positive PCR test result or this new T-cell test should be good enough to serve as exemption from vaccine mandates imposed by employers.
I don’t know if you’re referring to T-Detect, which is one test of T cells that can be used to see if someone has, or has not, had an infection with SARS-CoV-2. If you are, a positive test would only tell you that you were infected; it would tell you nothing about the robustness of your immunity to a reinfection. (And it costs $219-$299.)
T-Detect’s website itself states: “A T cell response is typically detectable in blood as early as several days after initial infection. How long this response lasts post-infection and **the implications for immunity are not known.** [my emphasis]
The La Jolla Institute of Immunology answered that question and they believe robust immunity of COVID survivors likely lasts for decades, but what do they know. It is clear, IMHO, from reading your posts that you are committed to the dogma that everybody must be vaccinated, including COVID survivors, without regard to any fact and/or study presented here. That is curious to say the least. But what do I know.
Speculation exists as to the robustness of the immunity that develops after infection with SARS-CoV-2. Trends have been identified that, on a population level, appear to show that those with severe (but not very severe, necessarily) infection develop longer lasting immunity than those with mild or asymptomatic infection. Unfortunately, when examined on an individual level, those trends lose a large degree of their reliability in predicting who is protected against reinfection.
There are many components of immunity against infection, from mucosal to humoral to cell-mediated. And each of these have a variety of sub-components. This is good in general as it allows the immune system, when it is working perfectly, to be very flexible, adaptable and resilient.
For our purposes in this discussion, the issue is how does one ascertain that one’s natural immunity is currently sufficient to make it unlikely that exposure to SARS-CoV-2 will result in a reinfection. It would be nice if we could simply check someone’s neutralizing antibody titer, or do a T cell test, or measure one or more of dozens of other parameters of the immune system, look at the result(s) and say that one very likely is or is not protected.
But we can’t. At least not yet.
In these days of AI, I think it would be possible to input many parameters of immune status (as it relates to SARS-CoV-2) and correlate that with the status of a test population comprised of those with previous infection, some of whom have had reinfections and some of whom have not. My guess is that some parameters will be strongly correlated with ongoing protection and others not so much. Ideally, there would be a few, easily measured, that would demonstrate strong correlation on an individual basis with protection (or lack thereof).
As I wrote, we’re not there yet. I presume someone, somewhere is working on such a project, but I don’t know that for a fact.
What I DO know, though, is that reinfections do occur. If you’ve read through the comments just on this forum alone, you’ve read comments from several people who have had reinfections, so I presume you’re not denying that reinfections occur.
My goal in engaging in this whole discussion is to remind people that, while an infection with SARS-CoV-2 likely has offered some protection from reinfection, it is demonstrably not a guarantee against reinfection. The vaccines are very safe (not 100%, but very safe) and likely far safer than an infection or reinfection. Infections or reinfections are a clear and present danger to some in society, if not to the person currently infected then potentially to others to whom the infection could be transmitted.
This is why I’ve been an advocate for vaccination, even in those with previous infections. As a physician, one of my guiding principles has been “Primum non nocere,” (First, do no harm). The course of action that best follows that principle is not always easy to calculate but, when it comes to COVID-19 vaccinations, given all the evidence of which I am aware, and allowing for the rare exceptions for unusual medical circumstances, it has been and remains my determination that all who are eligible for a vaccine should receive it.
Your problem is that you expect them to make decisions based on science. No doubt the public health authorities are aware of ALL of this, yet they keep pushing the vaccine on everyone, and mark my words here and now, they will eventually be requiring booster shots of everyone as well . . .
Have you seen the study entitled “Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections,” which was posted on August 25, 2021 on medrixiv.org (in preprint, so not peer reviewed yet, but very detailed)? Conclusion: “This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity.”
This was a very large study. Anonymized Electronic Medical Records (EMRs) were retrieved from MHS’ centralized computerized database for the study period of March 1, 2020 to August 14, 2021. MHS is a 2.5-million-member, state-mandated, non-for-profit, second largest health fund in Israel, which covers 26% of the population and provides a representative sample of the Israeli population. Overall, 673,676 MHS members 16 years and older were eligible for the study group of fully vaccinated SARS-CoV-2-naïve individuals; 62,883 were eligible for the study group of unvaccinated previously infected individuals and 42,099 individuals were eligible for the study group of previously infected and single-dose vaccinees.
To be fair, it also stated that those individuals who received ONE dose of the vaccine gained additional protection against the Delta variant. They stated that “When performing this analysis, we found a similar, though not significant, trend of decreased risk of reinfection, with an OR of 0.68 (95% CI, 0.38 to 1.21, P-value=0.188).” Obviously less than 1% is not a very significant difference at all, especially given the increased risk of side effects.
Because there is no money to be made or control to be leveraged with such a study.
My doctor wouldn’t order an antibody test for me because he said they were unreliable. I previously had covid last week of December, 2020. Had a positive antibody test in January. Now trying to get another antibody test to see if I still have the antibodies. Very frustrating.
You should find a new doctor who will help you. I visited our nurse practitioner and she had no problem at all ordering the test for me. Unfortunately, I’ve heard you can get a number to see levels. I wasn’t able to get my levels but received the positive test result. Good luck
You are all missing the point. It’s financial. Time to find out how many of those in control own stocks in the pharmaceutical companies providing the vaccines. Consumers are not paying for the vaccines, but the government is. In other words. the pharmaceutical companies ARE getting paid per dose out of our tax money. If you eliminate all the people who have already had COVID, the market for vaccines shrinks significantly. Ergo the potential for profit also shrinks.
.
I agree. The push for the J&J vaccine has dwindled and no one is holding them accountable for the harm their vaccine has caused. We have a friend who got that one and died the next day of a massive heart attack after having nosebleeds all day long that day. No accountability, just government funding. How many politicians from both sides of the aisle own their stocks.
The time has come for COVID survivors to take on the healthcare bureaucracies, other government agencies, and the private sector that carries water for the vaccine mandate crowd. It is time to take them all to court, along with the doctors who are telling their survivor patients they need to get vaccinated. The science is ample at this point to hold doctors liable for malpractice since the risk of the vaccine for a survivor is worse than the risk of reinfection. That is well established by “the data.” In regards to the rest of those who now discriminate against unvaccinated survivors, the science is not on their side. Based on the multiple studies showing acquired immunity equal to or superior to vaccinated immunity and ZERO studies showing vaccinated immunity superior to acquired immunity, any fair and honest court would have to rule in favor of the unvaccinated survivors and against the vaccine mandate crowd. The one big IF is this – It requires a court that still believes in the rule of law to rule according to the facts and the law, rather than the judge’s personal philosophical and/or political beliefs. It would also take a judge that has the courage to not be intimidated by the mob that riots in cities when they don’t like something. These days, unfortunately, that is a big if. It’s getting harder and harder to find judges of integrity who also have the guts to do the right thing.
Because it would kill their agenda. They do not want you to ask sensible questions because they don’t want to give you the obvious and sensible answer. The truth conflicts with their plan. Plain and simple.
It’s relatively easy to database who comes through for a vax, with brand and serial number. It’s not evil to factor in what’s inexpensive to track, especially globally.
Everyone clamoring for an antibody test and/or trying to prove natural immunity, may work out fine in some communities or whole nations such as Ireland, but I can see where the public health people, if they really thought the vax genuinely positive, would urge that upon everyone as it’s the easiest on the metrics. The United States is nowhere close to that organized.
How many old folks stayed home, gave each other a serious cold, and/or the flu even, and are now going around saying they had covid and recovered?
How many expensive antibody tests would it take to verify all those stories.
And yes of course, many do have proof, tests taken already, hospital records and so on. Maybe issuance of “I had covid and got well cards” should be left to each treating clinic or hospital to offer, and then see what that buys you in Vegas, maybe nothing.
Please read the article. This study, conducted in Seattle (USA), shows that the vaccine is more effective than “natural immunity”, as the antibodies target the RBD in a wider variety of places.
You are reading this and responding as if you don’t realize that the vaccine is better than getting the disease.
Note that all a vaccine does in the first place is to develop a person’s “natural immunity”, but instead of using a disease that can kill you to generate this natural immunity, it creates a dummy “foreign invader” that has no long-term negative effects, and the body is then well protected.
I think you are probably just creating false information here to confuse others coming to this website. But if you just don’t understand how this stuff works, that’s OK, don’t worry. Take the vaccine and make sure everyone else takes the vaccine.
If breakthrough infections do occur, than it’s possible/likely that the additional antibodies generated from the “natural immunity” would be add on to the vaccine-generated antibodies to improve the body’s response to future infections, reducing the already relatively remote chance of getting further breakthrough infections.
Of course, as long as people don’t get vaccinated, more and more people will suffer from breakthrough infections as the virus will be kept alive and mutating by those who aren’t getting vaccinated.
Sean – If you read all the comments, I think you will see that no one is saying that going out and intentionally trying to catch the disease is better than being poked. What the majority of us are stating is that MILLIONS OF US, through no fault of our own, caught and recovered from the virus and we now have natural immunity that has been shown to be at least as good as vaccinated immunity, if not better. You even state that natural immunity would be a boost to the shots. My position is that the shots are not necessary for us at this time. I can refer you to numerous studies that back up this claim. For example, see “Longitudinal analysis shows durable and broad immune memory after SARS-CoV-2 infection with persisting antibody responses and memory B and T cells (June 18, 2021).” To summarize this study: Ending the COVID-19 pandemic will require long-lived immunity to SARS-CoV-2. Here, we evaluate 254 COVID-19 patients longitudinally up to eight months and find durable broad-based immune responses. SARS-CoV-2 spike binding and neutralizing antibodies exhibit a bi-phasic decay with an extended half-life of >200 days suggesting the generation of longer-lived plasma cells. SARS-CoV-2 infection also boosts antibody titers to SARS-CoV-1 and common betacoronaviruses. In addition, spike-specific IgG+ memory B cells persist, which bodes well for a rapid antibody response upon virus re-exposure or vaccination. Virus-specific CD4+ and CD8+ T cells are polyfunctional and maintained with an estimated half-life of 200 days. Interestingly, CD4+ T cell responses equally target several SARS-CoV-2 proteins, whereas the CD8+ T cell responses preferentially target the nucleoprotein, highlighting the potential importance of including the nucleoprotein in future vaccines. Taken together, these results suggest that broad and effective immunity may persist long-term in recovered COVID-19 patients.
Whether or not that changes in the future is to be seen, but at this time it would be much more beneficial to EVERYONE if our immunity was recognized and the doses that would be used for us instead redistributed to other parts of the world. Given the extremely low rate of demonstrated reinfection, the science is on our side.
The study in The Lancet titled, “SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: a large, multicentre, prospective cohort study (SIREN)” showed a reinfection rate of 16% at a median of 7 months. That is hardly an “extremely low rate of demonstrated reinfection.”
As I understand the article, the vaccine targets more parts of the virus than natural immunity does which makes it more effective at launching a successful immune response. My question is why can’t we get REAL data on the harm these vaccines are doing? I’ve looked everywhere and there are no charts or numbers of people who have died or are seriously ill from taking the vaccines. I keep seeing 3,400 deaths attributed but it would be great to see more comprehensive data supporting or showing number has been down-played.
Sean, your comments seem sensible but you are slightly misstating some things yourself. The article above SUGGESTS that the vaccine immunity may be more effective than natural immunity because of the mechanism you stated. All they really “showed” was that it binds to more places on the RBD. So we can’t treat this as fact or conclusive, and we do need to consider other studies.
Second, your claim that the vaccine induces “no long term side effects” cannot possibly be substantiated. If this were true, the FDA could approve it tomorrow. Plus we obviously don’t have long-term studies on a virus/vaccine combination that has existed for all of 8 months. It’s overreaches like this that can make people feel as if you aren’t being intellectually honest.
I personally don’t think the majority of people come on here to “create false information”. I think there are a lot of legitimate questions about COVID and the answers are often incomplete or contradictory, as you would expect with a novel virus! The jury is still out. That is something we should all be able to agree on, if we still adhere to the strict scientific standards that we have in the past (ie. FDA approval).
Which leads to maybe the most contentious issue, mandatory vaccination. Despite the jury being out, the data being SUGGESTIVE but not complete, there are loads of people like yourself who say “Just get the vaccine and tell everyone you know to get it”. There are threats of civil liberties being taken away (and some instances of follow through). The TRUE problem is that when the average person asks “why should I get an experimental vaccine?”, which most do, people like you do not have answers that inspire security and trust. I’ve outlined above how you yourself just misstated and overstated information, and worse, used it to make an authoritative demand on others. It’s this attitude that is very prevalent right now, and why studies are finding that PhD’s actually comprise the largest group of anti-vaxxers. PhD’s ask questions and scrutinize answers. PhD’s want to know that drugs are safe by the same standards that we have always had historically. PhD’s aren’t going to be threatened into playing roulette with their bodies, especially if it may not have a substantial benefit.
I’m offering this critique that a few people might see it and think harder about the statements they use. Right now, we are all trying to figure this thing out, and if you want to persuade people, you’ll need to be very careful about your statements, lack of citations, and respect for the intelligence of other people.
This is very well put and the most succinct answer to the entire virus/vaccine issues. The unknowns of the virus and the unknowns of the vaccine and the unknowns of our immunity all need more time. Rush to judgement and rush to force vaccinations are going against common sense and not giving science enough time to work. Unfortunately, I fell to family pressure and have gotten one shot so far. Yet I had a positive antibody test after having covid 8 months ago. Common sense tells me I was okay, but pressure of not being allowed to see children forced my hand. I’m not happy with my decision.
Overall, I agree with most of your post—thoughtful and cogent—and I agree that “…if you want to persuade people, you’ll need to be very careful about your statements,…” In that regard, one phrase within your reply caught my attention.
“The TRUE problem is that when the average person asks ‘why should I get an experimental vaccine?’…”
In the age groups for which the COVID-19 vaccines are recommended, they are not “experimental” (nor currently approved), they are authorized. For the age groups in Phase 3 trials (or earlier), the COVID-19 vaccines currently are experimental, that is true.
I understand that the reference to the “average person” was not necessarily referring to you, but to those who have concerns about the vaccines (possibly including yourself), and likely in part because they have not yet been approved. But I thought it was important to point out that the authorized vaccines have more evidence of their safety and efficacy than “experimental” vaccines, which is, in part, why they are now “authorized.”
What other countries are saying don’t get vaccinated if you’ve already had it? The UK recommends getting vaccinated anyway. So does Australia. So do all the EU countries. The only places advising against it are doing so because they haven’t been able to obtain enough vaccine doses and are forced to ration it out.
Regardless, this very page you are commenting on has links to papers shows that getting natural immunity from a vaccine (and yes that’s what vaccines do, give you natural immunity, its not an either/or) seems to be more effective than getting it solely from infection, an activity that can expose you to serious disability or worse.
One other thing I wanted to add is that the 6.72 increased infection rate for vaccinated individuals from the Israeli study is being suppressed by google and you can’t easily find it by doing a google search, yet you can easily find it doing a search on bing. The attempted suppression of this information also bothers me.
Ryan, do you have a citation for the “7 times more likely” infection in vaccinated vs natural immunity?
It doesn’t look like this blog lets you post links to websites…but I will give you the relevant part of the study and if you post some of it in bing, you should be able to come up with the citation…again, this really disturbs me that you cannot find this doing a google search…even if it was “fake news” (which it is not), it is complete big tech censorship and very ugly…
“Health Ministry data on the wave of COVID outbreaks which began this May show that Israelis with immunity from natural infection were far less likely to become infected again in comparison to Israelis who only had immunity via vaccination.”
“With a total of 835,792 Israelis known to have recovered from the virus, the 72 instances of reinfection amount to 0.0086% of people who were already infected with COVID.
By contrast, Israelis who were vaccinated were 6.72 times more likely to get infected after the shot than after natural infection, with over 3,000 of the 5,193,499, or 0.0578%, of Israelis who were vaccinated getting infected in the latest wave.”
As for posting links, you are correct that they apparently are not allowed in the comments.
The workaround is to post the title of the article you would have linked, along with (if possible) the date, the name of the journal (if relevant) or the name of the website, or any other localizing/identifying information that might also help.
Do you need a citation for legitimacy? Sounds like the Israeli study reasoning.
I wonder if the NIH can explain whether an immune population can destroy the virus. Do antibodies kill or neutralize COVID-19 virus in vaccinated people? Does the virus die inside a healthy immune person? In other words if a large portion of people were immune or vaccinated, would the virus population die from antibodies in healthy people because the virus cannot grow, mutate, or spread? Is natural immunity better than vaccination?
Wow, so we are assigning ALL immunity to COVID to a single binding site on the virus? Not a bad study just a very presumptive title for something we know very little about. Does natural immunity target other parts of the virus that the vaccine does not? Seems to be very little appetite, aka grant funding, to even look into this.
There is a distinction between a “key issue” and an “only issue.”
No mention of the study posted on this site as to key study showing blood type may predict outcomes and severity of Covid.
Oxford University and the Office of National Statistics have found the opposite.
Once someone has fully recovered from an infection there is statistically zero chance of being infected with a high viral load again.
(Low viral loads have been detected, but this is at levels where the subject isn’t I’ll or able to pass it on).
Whereas, vaccinated people are regularly becoming infected and very ill.
Axios has an article from July 26 (“GOP Rep. Clay Higgins says he has COVID for second time”) showing just the opposite of your claim. According to him, “this episode is far more challenging.”
I wouldnt accept an anecdotal claim from him as any reliable evidence of reinfection. Perhaps he didn’t have a verified case of COVID-19 one or both times. The tests have a history of both false negatives and false positives. In addition, does he even say he was tested? We also know that a lot of Flu cases have been misdiagnosed as COVID-19, especially back in 2020. Most likely, the politcian didn’t have COVID-19, but rather, had the Flu or something else on one of, if not on both occasions.
I am currently recovering from my 3rd bout with Covid 19 AND got my second Pfizer shot in May. My first & worst Covid infection was Jan. 2020. I was contact traced and there was a direct link to China. I was contact traced with the current infection from a salon I went to two weeks ago. My first hair cut in over a year and the stylist ended up in the hospital with Covid, she was not vaccinated. I rarely leave my property and have always worn a mask in public. I am retired medical and know how to wash my hands and do so often. I don’t want there to be another lockdown but am ready for it. I don’t have enough faith that more people will get vaccinated . . .
Have you tested positive for the virus each time? Or just feel like you have it again? It might be that you have a “long haulers” case, which would involve your body experiencing “flare ups” on occasion due to a number of factors. Dr. Mobeen Syed has done some excellent videos on the subject. HIs latest one with Dr. Bruce Patterson is a must see! Dr. Bruce Patterson’s team has discovered that the S1 pieces of the spike proteins persist in the monocytes resulting in immune dysregulation and long-haul syndrome. I hope his research brings you and others in your same situation much needed relief.
A salient point for sure and seemingly more important than reinfection per se. If the rare reinfections of the naturally immune are not spreading the virus or resulting in hospitalizations, then WHO CARES?! Please investigate this further and prove it to be false OR start treating the recovered the same as vaccinated immediately.
A quick Google search revealed a WJLA (ABC News affiliate) article by Brooke Conrad dated June 4, 2021, titled “Natural COVID infection provides similar protection to vaccines, Israeli study shows.” This particular article provides live links to a reprint of the Israeli article other posters have mentioned. There are other links to articles mentioned in The NY Times related to long-lasting immunity after recovery.
In this present situation it is so difficult to say that ‘we move closer to ending the pandemic’.
100% of scientists agree with the people funding them.
Do you want to know why studies aren’t being done on natural immunity? $3.5 billion in the first quarter, that’s why.
We have a BINGO !!!!!! That is also the same reason that proven safe, yet cheap, therapeutics that enjoyed substantial success amongst the patients of some very distinguished doctors, was shoved aside in favor of new and VERY expensive drugs which were no more effective, and perhaps not even as effective, as the cheap generic. FOLLOW THE MONEY !!!!
One, the mRNA vaccine and its results on humans will provide enough information to pave the way for future mRNA anti-cancer and other disease therapy. Secondly, the mRNA money-making business goes way beyond COVID and disease. Any country can release a virus accidently, or purposely. We just experienced that. The mRNA vaccine was decided to be the quick defense response much like shooting downing a missile aimed at your country. Governments need a fast to produce shield, Pharma wants the money, Scientists want the fame. No other time in history was there an opportunity so great as we see today to have the world as one clinical trial cohort. Why would Pharma, the Governments, and Scientists refuse this golden opportunity? Yes, we simpletons are being used and lied to, but according to them, all in the name of the greater good. I just feel so sorry for all those people who suffered and died needlessly when a simple cocktail of pre-purposed drugs would have most likely saved their lives. I praise all doctors who fight against being a chess piece and tirelessly uphold their Hippocratic Oath. I never signed up nor agreed to this experiment, and I will never do so. I will rely on my healthy body and highly functioning immune system to protect me . . .
Very well said.
It pleases me to know the FDA has finally revised the emergency use authorization for casirivimab and imdevimab (REGEN-COV, Regeneron) to allow their use as a post-exposure prophylaxis (PEP) for COVID-19 in adults and children 12 years of age and older, weighing at least 40 kg, who are at high risk for progression to severe COVID-19, including hospitalization or death. Excellent news for all. Better late than never.
This completely contradicts what Israel just released. Their study shows that those who recovered from COVID has 6.7 times the protection against COVID and the variants. While we all know this virus was produced in a Chinese lab so it may not act like normal viruses, we all know that the antibodies produced from having a virus are far superior to the vaccine, especially when there are new variants. Can you imagine if they suggested that people get the flu vaccine after they recovered from the flu? The vaccine seldom matches the flu virus of a season. So why would someone get a flu vaccine which doesn’t cover the strains our there when the body produced antibodies from the actual virus? $$
Please, please, please get vaccinated.
If anyone is reading these comments, please be aware that there are a large number of anti-vaxxers on here parading around false data, agreeing with themselves that the vaccine is somehow dangerous, when we all know:
* the chance of death from COVID is about 1 or 2 in 100 (600,000+ dead from 35M confirmed infections in the United States) vs.
* the chance of death (related to women who are on birth control with the J&J vaccine, due to blood clots) is about 7 chances in 1,000,000.
* the chance of death to unvaccinated people who get COVID is 10x higher (about 70 chances per 1,000,000) to die from blood clots.
If you are a woman on birth control, and the J&J vaccine is the only available vaccine, by all means, take it. It reduces your chance of death from COVID from 1 or 2 in 100 to 7 in 1,000,000.
* That improves your odds of survival by about 1,500x. That’s 150,000% less chance of death.
* Not to mention all the people that suffer from lifelong disability due to COVID, which some people thing is actually worse than dying.
* Oh, and your chance of dying from a blood clot will also be reduced by 10x.
But if you are a women who is on birth control and another (Pfizer, Moderna) vaccine is available to you, take that instead. Your chance of dying from a COVID will be reduced massively, and you will have no chance to develop a blood clot.
If you are a man, or a woman who is not on birth control, take the vaccine. You will reduce the chance of dying from COVID to less than 1 out of 100,000, vs. 1-2 out of 100.
Many people do not understand math, and they simply don’t do this comparison. They rely on anecdotes and inferences. It’s about 1,500x better to take the vaccine than to take your chances.
Your chances of dying while texting go up by 27x. If you see people texting while driving, please don’t complain if you are unvaccinated. That’s 55x safer than not getting vaccinated. In other words, imagine you’re on a highway with 55 cars around you and every single one of those drivers is texting and no one is looking at the road. That’s how dangerous you are to society by not getting vaccinated.
Please take the vaccine, not just for yourself, but for all the people, especially the unvaccinated children, who are being infected with this disease.
Do the math, stop trying to confuse people, get yourself vaccinated, and let’s put an end to this disease, and this society destroying madness.
The question isn’t if the vaccination is safer than not getting it. The question is, is the vaccine worth the risk if you’ve already had Covid? I had Covid last October. I got vaccinated with Pfizer in April. The vaccine provoked a clot as I have a clotting disorder. In my clotting groups, it seems like only the people that were previously infected are clotting. It needs to be discussed so it can be studied!
Crystal – So sorry you are going through this and I agree with you 100%. The risk versus reward just doesn’t add up for recovered folks. We are at a much higher risk for serious side effects after the shots than the naive population. To the people who would call us “selfish” – we already did our part to create “herd immunity.” Most of us are frontline and/or essential workers who had no choice but to be put at risk.
Everything you said!
Thanks for saying that because it’s true. Natural immunity is better, 18 of us in my family got Covid last December. All recovered. Many of us have health issues as one of my daughters has one kidney and I have kidney disease. My other daughter who’s still in CALIFORNIA has health issues but hasn’t gotten Covid. My oldest sister died May 1 , 2021, she had a lot of health problems and they shouldn’t have given her the vaccine. She died. My best friend here got the vaccine she died 10 days later. My accupuncturist got Covid along with her entire family of 6 last December. They’re in the health field so they had to get vaccine. The grandparents got violently ill one went to hospital all others got sick for a week . They all got more Severe symptoms of Covid from the vaccine after they all had Covid. My step daughter had Covid last December also, she had cancer few years before. She recovered fine from the virus she decided to get the two shot vaccine, got violently ill from the vaccine and decided not to get 2nd. My grandson got Covid along with all of us last December. He was 10 at time. He recovered fine in 3 days. I recovered fully in 5 days. Our 83 year old in law with diabetes got Covid and recovered fine. No one has had any problems since. I myself have low kidney function and I felt the virus affected me during the time I had it. I will not put myself through undue sickness. NATURAL IMMUNITY NEEDS TO BE RECOGNIZED BY NIH AND PUT OUT TO THE PUBLIC. We will see many more deaths from people getting vaccine after having had Covid and getting vaccine and those who’ve had vaccine who’ve gotten Covid after vaccine.all the truth is not out there and this is politically motivated.
Thanks
I don’t believe you have a bunch of “anti-Vaxers” commenting here with false info….. they are simply stating that vaccines may not be necessary for people with natural immunity at this time. And that since they are Currently protected, their vaccines could be given to someone at a higher risk group…… a reasonable game plan
Sean, you are posting false data or simply “do not understand math”
FALSE: “the chance of death from COVID is about 1 or 2 in 100 (600,000+ dead from 35M confirmed infections in the United States)”
CDC website: “Estimated COVID-19 Infections, Symptomatic Illnesses, Hospitalizations, and Deaths in the United States”
CDC estimates that from February 2020–May 2021 the chance of death from COVID is 0.6 in 100 (120.2 Million Estimated Total Infections and 767,000 estimated deaths).
One size does not fit all my friend, nor do aggregated, population level statistics.
A relevant, recent pre-publication (not peer-reviewed) from Emory University, Atlanta. : TITLE Longitudinal analysis shows durable and broad immune memory after SARS-CoV-2 infection with persisting antibody responses and memory B and T cells.” (medRxiv).
My comment: There are now a series of outcome studies which provide compelling evidence of noninferiority of natural infection with Sars-CoV-2 vs. vaccination, with respect to efficacy and duration of protection against reinfection. However, in keeping with the current discussion of RBD-directed antibodies and protection against variants of the virus, this pre-publication longitudinal study of SARS-CoV-2 specific B and T cell memory after infection in 254 patients who recovered from COVID (not yet peer reviewed) from Emory University two weeks ago may be of interest to the group. It discusses the possibility that natural immunity may provide enhanced protection against the SARs-Cov-2 variants.
Selected quotation: “Overcoming the challenges to end the pandemic is accentuated by the recognition that SARS-CoV-2 can undergo rapid antigenic variation that may lower vaccine effectiveness in preventing new cases and progression to severe disease. (24,28,29) Our findings show that most COVID-19 patients induce a wide-ranging immune defense against SARS-CoV-2 infection, encompassing antibodies and memory B cells recognizing both the RBD and other regions of the spike, broadly-specific and polyfunctional CD4+ T cells, and polyfunctional CD8+ T cells. The immune response to natural infection is likely to provide some degree of protective immunity even against SARS-CoV-2 variants because the CD4+ and CD8+ T cell epitopes will likely be conserved.”
Thanks for posting that.
Numbers and other characteristics of T cells and B cells are not unimportant, of course, but to assume that they can predict what will happen out in the world is not as good as seeing what, you know, happens in the world.
If you haven’t done so already, look at the study in The Lancet titled, “SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: a large, multicentre, prospective cohort study (SIREN). It showed that 16% of people with previous SARS-C0V-2 infections were reinfected at a median of 7 months. And the only variant they dealt with (in addition to the original strain) was the Alpha variant.
The fact is that those who have had the misfortune of having been infected with SARS-CoV-2 can be infected again, and their risk is far from trivial. Until someone can derive a reliable metric (currently nonexistent) of some sort that can predict with a high degree of confidence what the risk of reinfection is in any one person, assuming one is protected simply because they previously had a SARS-CoV-2 infection is unwise. Unless they have a medical contraindication to being vaccinated (ideally a decision arrived at in conjunction with their personal physician), vaccination is definitely what should occur. Maybe one shot, maybe two, but certainly something.
I just want to point out that the Johnson & Johnson shot has an efficacy rate of 66.3% (see “Johnson & Johnson’s Janssen COVID-19 Vaccine Overview and Safety” on the CDC website). And yet, that is considered an effective vaccine. Additionally, with the Delta variant, we are continuing to see the efficacy of all the vaccines go down. Plus even if someone gets reinfected, the cases are generally not resulting in hospitalization and/or death, which is the criteria being used by the CDC to define a breakthrough case for vaccinated individuals. You also continue to discount the risk associated with these shots, which studies have shown to be much higher than with naive individuals. I honesty do not see the point at all in recovered folks getting vaccinated. IF data changed down the line and I saw the number of reinfections rise, I would reconsider my position (and hopefully at that point the Novavax will be available), but at this point I just don’t see the need. Also, the WHO has come out and said that we need to get the rest of the world vaccinated or else this nightmare will just continue on. Vaccinating recovered individuals is just wasting doses that could be sent to high-risk individuals around the world.
Fortunately (at least for those of us in the US), the J&J vaccine has been used only in about 7%. The mRNA vaccines show significantly higher effectiveness, including against the Delta variant. Nonetheless, the J&J vaccine is working reasonably well, even against the Delta variant, if the metric is preventing hospitalization and death, as a recent study released August 6 from South Africa showed (See “Sisonke Update on the Janssen®(JNJ) Ad26.COV2.S vaccine”).
The prevailing discussion on this thread has been that, once infected, the risk of reinfection was minuscule (some claiming there are none, some claiming only 52 in the whole world). The Lancet study showed otherwise, and convincingly so.
Whether or not someone who has experienced a SARS-CoV-2 infection wishes to take their chances against reinfection is, of course, up to them. This virus has been shown to have the potential to not only kill, but also to wreak damage on multiple organ systems, and that damage has persisted in some of its victims. Will it be permanent? I don’t know, but likely so in some. Will the infection result in future consequences not yet seen? Increased risks of pulmonary fibrosis, chronic renal failure, neurocognitive impairment, neurodegenerative disorders? Time will tell.
The more defenses, and the more robust those defenses, against the virus that can be implemented, the better the chance that infection will not occur, or reoccur. If I had had COVID-19, I certainly would do everything in my power to prevent reinfection, including and especially being vaccinated. Even though the clinical illness of a reinfection might not be so bad (though no guarantees of even that), that would still mean that, once again, a highly and broadly pathogenic virus gained access to my body that I would very much like to prevent, if not the first time, then most definitely the second.
“Whether or not someone who has experienced a SARS-CoV-2 infection wishes to take their chances against reinfection is, of course, up to them.” Not if they want to remain employed. Based on your data, the probability of reinfection for a recovered individual is far less than one vaccinated with J&J, yet the vaccinated individual is granted increasingly more rights. It’s glaringly illogical. Add it to the list.
antibody mediated viral enhancement
One more point regarding your reply.
“Also, the WHO has come out and said that we need to get the rest of the world vaccinated or else this nightmare will just continue on.”
I’m glad to see that you’re a fan of WHO’s recommendations. Here’s one regarding vaccinations in those with previous infection: “Take whatever vaccine is made available to you first, even if you have already had COVID-19.” (from the WHO website, “COVID-19 advice for the public: Getting vaccinated”)
And WHO also said “To conclude, available tests and current knowledge do not tell us about the duration of immunity and protection against reinfection, but recent evidence suggests that natural infection may provide similar protection against symptomatic disease as vaccination, at least for the available follow up period.” See Guidance from WHO dated May 10, 2021 – COVID-19 Natural Immunity
And the statement from the WHO regarding getting vaccinated even if you’ve had an infection (that I had posted) was updated July 14, 2021, so that is their most recent recommendation regarding vaccinations in those previously infected.
Note also in the sentence quoted by you the word “suggests.” That connotes uncertainty about the robustness and duration of natural immunity, which is probably why, despite that statement, they still recommend vaccinations in those previously infected.
Based on the lack of candor on the part of the WHO, which is well documented back to the beginning of the pandemic, I do not believe they have any credibility left with anybody who has been paying attention. That goes for the CDC and FDA as well. Fool me once, shame on you. Fool me twice, shame on me.
If the vaccine were undeniably safe and effective, per logic the vaccine stockpiles should be scarce as early pandemic toilet paper. And yet some humans have an incredible capacity to resist logic and argumentation.
Should we order the suggest protocol for the Delta or Covid virus prior to possibly getting sick as a precaution?
I recently recovered from the delta variant. I’m 55 years old and have never experienced any kind of sickness like this. In my opinion, this horrible plague was released on purpose to destabilise the world and our great nation which was ready to distance ourselves from other competitive nations. It has worked to perfection. We are fighting amongst ourselves and growing apart, when we should be coming together. As for the virus, it’s not going anywhere. It will keep coming around every year just like other viruses. I just wish we would spend more time on finding the truth about how it got released. Someone needs to pay! Just my 2 cents.
There was an excellent article published today by Katelyn Jetelina. She has a Masters Degree in Public Health and a PhD in Epidemiology and Biostatistics.
Search for “Your Local Epidemiologist “Natural” immunity protection and variants”
The article has many relevant and informative links, along with an up-to-date summary of some of what is known about how natural and vaccine-induced immunity compare.
I was infected with the original COVID back in October, and then the Delta variant about a month ago. The first infection was like a heavy cold and I lost my sense of taste and smell (returned after 7 days). The Delta variant infection was barely there (extremely mild cold) with a muted taste and smell. There is zero percent chance that I want or need a vaccine. I have no doubt if I got a third variant that it would also be mild. My body’s natural response to the Corona virus is plenty good enough for me. It’s frustrating that we only focus our testing on vaccines for political reasons, and media only runs with one side of the story. BTW… I support vaccines… I just don’t need or want this one.
I agree with you as well. I haven’t had the variant as far as I know and I may never know. I had covid and 8 months later have antibodies per doctor testing. I still don’t have taste and smell. I think my body will fight the next round as it fought off the first round without hospitalization which Supposedly was the main goal of the vaccine. Some are thinking its a cure! It was never to be that. Only to reduce the stress on the hospitals. Well, our natural immunity did and is doing the exact same thing.
Thanks for your post, and for confirming (for those who doubted the possibility) that second infections do occur. I am glad to read that your second illness was mild. I hope there are no long-term implications for your health from the first or second infection.
Reinfections are not always mild, though it may be more likely in older populations for the reinfection(s) to be more severe; I don’t think enough is yet known about that. The CDC issued a MMWR report on February 26, 2021 (“Suspected Recurrent SARS-CoV-2 Infections Among Residents of a Skilled Nursing Facility During a Second COVID-19 Outbreak — Kentucky, July–November 2020”) in which the “Severity of disease in the five residents during the second outbreak was worse than that during the first outbreak and included one death.”
This forum has broadened to a more general discussion of the efficacy of natural immunity vs vaccination. This is very reasonable, since the index article for these comments is a study of a very specific research test, which is not a meaningful outcome on which to base any clinical decisions . . .
Some commenters have cited the SIREN study. This study showed about a 7% reinfection rate (not 16% which is where they broadened the definition to “all possible or probable” — criteria no clinical trials have used), which is exactly in the range of the best vaccines currently available.
Here is a quote from that article:
“Using a COVID-19 symptomatic case definition aligned with positive PCR results, previous infection reduced the incidence of infection by at least 90% (aIRR 0·07, 95% CI 0·06 to 0·10) and even when we included all possible and probable reinfections reduced the incidence of reinfection by at least 84%(aIRR 0·159, 0·13–0·19).”
As you can see, the criteria for the extremely conservative 16% reinfection is not realistic in real-world terms. Moreover, the major outcome here basically tracks the various immunities with respect to a laboratory test: COVID test positive. The best evidence would be where there are more true meaningful outcomes, such as hospitalization, intubation and mortality. That having been said, it provides some of the strongest evidence in support of natural immunity.
Perhaps the readers are aware of the previous article in New England Journal of Medicine, from Dec 2020, which found an extremely low rate of re-infection in those who have a positive antibody test. Those with antibodies had no symptomatic infections. To quote that study: “In this longitudinal cohort study, the presence of anti-spike antibodies was associated with a substantially reduced risk of PCR-confirmed SARS-CoV-2 infection over 31 weeks of follow-up. No symptomatic infections and only two PCR-positive results in asymptomatic health care workers were seen in those with anti-spike antibodies, which suggests that previous infection resulting in antibodies to SARS-CoV-2 is associated with protection from reinfection for most people for at least 6 months.”
The Cleveland study referenced by the previous reader is not yet peer reviewed, but it is possible to view the results oneself . . .
Readers will agree it quite impressively demonstrates the efficacy of natural immunity. Again, please note that the study includes healthy, highly exposed workers. Those with natural immunity had an average of 10 months of data. The main challenge of this study is that it gives little information about the new variants. The delta variant started appearing in the Midwest (location of this study) approximately mid-March, which is 60 days prior to the end of the study (data ends on May 15, 2021), and was still of low prevalence. There is a very small split in the data at the end, suggesting superior immunity among those with natural immunity and/or vaccine plus natural immunity, but the difference is too small to draw meaningful conclusions. Since the delta variant just started to appear at this time, it would be fascinating to conjecture that there may be improved protection from delta among those previously infected, but this would be an extreme extrapolation.(3)
IMPORTANT CONCLUDING COMMENT ABOUT VACCINATION
I hope that the readers will agree that vaccination is still the best option for those who no do not have natural immunity. Also, although the previously mentioned studies are quite compelling in support of natural immunity as non-inferior to available vaccines, these were conducted in employees, a generally healthier population (i.e. a potential “healthy worker effect”). If a person is immunocompromised, obese or has any other important risk factors, I would strongly encourage these individuals to receive vaccination even if previously infected, since we do not have data to support otherwise at this point.
Perhaps it would be even better to characterize the results of the SIREN trial as showing a minimum of 7% reinfection, possibly as high as 15.9%. Or alternatively, the reinfection risk was 7–15.9%.
Even at the minimum of 7%, that risk is not “extremely low” as the reinfection risk has been characterized by others on this forum. Also, it is notable that the median interval between infection and reinfection was only 7 months. Not only is this a relatively short interval, it indicates that some of those studied were reinfected even before 7 months. And again, it is worth pointing out that the SIREN trial dealt only with the original strain and the Alpha variant, not the much more contagious Delta now so prevalent in the United States (and elsewhere). I think it likely (speculation on my part) that the reinfection risk, relative to Delta exposure, exceeds that minimum 7% risk found in the SIREN study.
D Hart MD, you continuously reference the SIREN study in defense of vaccinating those who have already been infected with COVID, even as it appears that more and more evidence builds against that position. You do realize that the final conclusion of the SIREN study was “This study shows that previous infection with SARS-CoV-2 induces effective immunity to future infections in most individuals.”
It would appear that you have drawn a different conclusion from the data than the authors.
Phil Warwick, thank you for your reply.
“‘This study shows that previous infection with SARS-CoV-2 induces effective immunity to future infections in most individuals.’
It would appear that you have drawn a different conclusion from the data than the authors.”
Appearances can be deceiving, particularly when you don’t pay attention to words that, in context, turn out to be key words.
In this case, the key word is **most**. “Most” means “greatest in quantity, extent, or degree; the majority of.” That would span the range of 50.1% – 99.9%.
As the SIREN study showed 7% – 15.9% of previously infected individuals were reinfected, that means that 84.1% -93% of individuals (“most”) were not reinfected (at least for the duration of the study; they certainly could have been reinfected subsequent to the conclusion of the study, but whatever).
Therefore, my conclusion that vaccinating those with previous SARS-CoV-2 infections is prudent is entirely consistent with the results of the SIREN study and not different from the conclusion of the authors. While **most** individuals will have effective immunity to future infections, a nontrivial minority will not.
Agreed and very clear summary. I am a healthy young person in my 20s and am at risk of being thrown out of college due to not being vaccinated. I do not plan on vaccinating because my body is strong and has already recovered from COVID in March of 2020, and will recover again should I contract the virus. The new variants are so mild compared to original COVID that I do not understand why the world is panicking about it. It can be compared to seasonal illnesses that come around regularly. I am ready to quit college (I am in my final year of graduate school) because they are removing personal choice and freedom, and that is more important to me than my degree. It seems that they don’t care much about my personal choice or about medical information that has guided the globe for centuries; namely, that someone who had already recovered from a virus will be able to fight it again successfully.
So sad to hear of your predicament. You should be issued a Certificate of Recovery in lieu of a vaccination card, as is the case in Europe and Israel, but because of widespread corruption in our government, you are being screwed over, like millions of others.
Can a breakthrough case with covid 19 infection in a vaccinated person result in a variant? If not, please explain.
Variants can arise any time the virus replicates. The virus cannot replicate unless it has infected a host, vaccinated or not. So, yes, a variant can arise as a result of a breakthrough infection.
My immune system is overactive which can cause health problems. I recovered from Covid 19 and I am confident that my overactive immune defenses along with typical remedies to upper and lower respiratory infections helped My primary Dr agreed that I am adequately protected and it is reasonable not to take the vaccine. However, I get a lot of blow back from friends and family who even say my Dr is a quack. The CDC especially is advertising a hard sale on vaccines while ignoring people like me. It has become clear that they only care about pushing this shot. It is something going on that is suspicious and dangerous. I am not sure what but I keep thinking money.
Wow. Hardly anyone read the article before spreading malarkey.
Vaccines are better than natural immunity. Get with the program!!
Tell the Israelis. They ‘re vaccinated and getting sick. By the thousands.
Proof that the injections do not work.
I am a layperson who has spent a couple of hours trying to read through the article and the (seemingly) hundreds of comments. I was interested because I have had Covid antibodies for at least a year — though their number has never been quantified, so I do not know if they are diminishing. I have been trying to decide whether or not to also get a Covid vaccination. I found the debate informative and fascinating, especially the interchanges between Dr. Hart and his commentators. The conclusion that I draw is that the evidence for longevity and durability of natural immunity is strong but not conclusive. What persuades me to continue to wait (while seeking periodic antibody tests) is that both Israel and the EU have established as official policy to provide Covid Recovery Certificates which exempt recoverers from the mandate to either be vaccinated or regularly tested, or be faced with increasingly extreme limitations on what activities one will be allowed to participate in. These Recovery Certificates will have equal stature to Vaccine Passports, and will be extended for 6 months at a time, in order to allow more evidence to accumulate about the durability of natural immunity. This week the matter became especially fierce in New York City, where I live. There are people who will lose their jobs, and all of us unvaccinated recoverers will be denied access to the cultural riches of New York, which is the reason we have chosen to live here. There is even the possibility that we will lose the right as democratic citizens to attend official governmental public policy decision discussions of the New York City Council, New York State legislature, courts, school board meetings, and more. All because we want to have the same policy adopted in New York, and throughout the US as exists in Israel and the EU. If it is good enough for them, why not for us?
Muscle strain is an injury to a muscle or a tendon — the fibrous tissue that connects muscles to bones. The data I found in this blog was beyond my expectations.
Thanks for sharing such content.