How Immunity Generated from COVID-19 Vaccines Differs from an Infection
Posted on by Dr. Francis Collins
A key issue as we move closer to ending the pandemic is determining more precisely how long people exposed to SARS-CoV-2, the COVID-19 virus, will make neutralizing antibodies against this dangerous coronavirus. Finding the answer is also potentially complicated with new SARS-CoV-2 “variants of concern” appearing around the world that could find ways to evade acquired immunity, increasing the chances of new outbreaks.
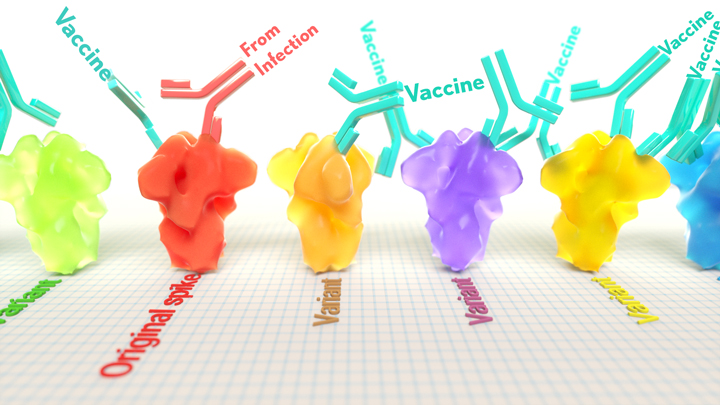
Now, a new NIH-supported study shows that the answer to this question will vary based on how an individual’s antibodies against SARS-CoV-2 were generated: over the course of a naturally acquired infection or from a COVID-19 vaccine. The new evidence shows that protective antibodies generated in response to an mRNA vaccine will target a broader range of SARS-CoV-2 variants carrying “single letter” changes in a key portion of their spike protein compared to antibodies acquired from an infection.
These results add to evidence that people with acquired immunity may have differing levels of protection to emerging SARS-CoV-2 variants. More importantly, the data provide further documentation that those who’ve had and recovered from a COVID-19 infection still stand to benefit from getting vaccinated.
These latest findings come from Jesse Bloom, Allison Greaney, and their team at Fred Hutchinson Cancer Research Center, Seattle. In an earlier study, this same team focused on the receptor binding domain (RBD), a key region of the spike protein that studs SARS-CoV-2’s outer surface. This RBD is especially important because the virus uses this part of its spike protein to anchor to another protein called ACE2 on human cells before infecting them. That makes RBD a prime target for both naturally acquired antibodies and those generated by vaccines. Using a method called deep mutational scanning, the Seattle group’s previous study mapped out all possible mutations in the RBD that would change the ability of the virus to bind ACE2 and/or for RBD-directed antibodies to strike their targets.
In their new study, published in the journal Science Translational Medicine, Bloom, Greaney, and colleagues looked again to the thousands of possible RBD variants to understand how antibodies might be expected to hit their targets there [1]. This time, they wanted to explore any differences between RBD-directed antibodies based on how they were acquired.
Again, they turned to deep mutational scanning. First, they created libraries of all 3,800 possible RBD single amino acid mutants and exposed the libraries to samples taken from vaccinated individuals and unvaccinated individuals who’d been previously infected. All vaccinated individuals had received two doses of the Moderna mRNA vaccine. This vaccine works by prompting a person’s cells to produce the spike protein, thereby launching an immune response and the production of antibodies.
By closely examining the results, the researchers uncovered important differences between acquired immunity in people who’d been vaccinated and unvaccinated people who’d been previously infected with SARS-CoV-2. Specifically, antibodies elicited by the mRNA vaccine were more focused to the RBD compared to antibodies elicited by an infection, which more often targeted other portions of the spike protein. Importantly, the vaccine-elicited antibodies targeted a broader range of places on the RBD than those elicited by natural infection.
These findings suggest that natural immunity and vaccine-generated immunity to SARS-CoV-2 will differ in how they recognize new viral variants. What’s more, antibodies acquired with the help of a vaccine may be more likely to target new SARS-CoV-2 variants potently, even when the variants carry new mutations in the RBD.
It’s not entirely clear why these differences in vaccine- and infection-elicited antibody responses exist. In both cases, RBD-directed antibodies are acquired from the immune system’s recognition and response to viral spike proteins. The Seattle team suggests these differences may arise because the vaccine presents the viral protein in slightly different conformations.
Also, it’s possible that mRNA delivery may change the way antigens are presented to the immune system, leading to differences in the antibodies that get produced. A third difference is that natural infection only exposes the body to the virus in the respiratory tract (unless the illness is very severe), while the vaccine is delivered to muscle, where the immune system may have an even better chance of seeing it and responding vigorously.
Whatever the underlying reasons turn out to be, it’s important to consider that humans are routinely infected and re-infected with other common coronaviruses, which are responsible for the common cold. It’s not at all unusual to catch a cold from seasonal coronaviruses year after year. That’s at least in part because those viruses tend to evolve to escape acquired immunity, much as SARS-CoV-2 is now in the process of doing.
The good news so far is that, unlike the situation for the common cold, we have now developed multiple COVID-19 vaccines. The evidence continues to suggest that acquired immunity from vaccines still offers substantial protection against the new variants now circulating around the globe.
The hope is that acquired immunity from the vaccines will indeed produce long-lasting protection against SARS-CoV-2 and bring an end to the pandemic. These new findings point encouragingly in that direction. They also serve as an important reminder to roll up your sleeve for the vaccine if you haven’t already done so, whether or not you’ve had COVID-19. Our best hope of winning this contest with the virus is to get as many people immunized now as possible. That will save lives, and reduce the likelihood of even more variants appearing that might evade protection from the current vaccines.
Reference:
[1] Antibodies elicited by mRNA-1273 vaccination bind more broadly to the receptor binding domain than do those from SARS-CoV-2 infection. Greaney AJ, Loes AN, Gentles LE, Crawford KHD, Starr TN, Malone KD, Chu HY, Bloom JD. Sci Transl Med. 2021 Jun 8.
Links:
COVID-19 Research (NIH)
Bloom Lab (Fred Hutchinson Cancer Research Center, Seattle)
NIH Support: National Institute of Allergy and Infectious Diseases
What happened to resistance against gleevac? I gather the rate of mutation in a virus during a pandemic is greater than the rate of mutation of cancer cells?
What are the actually numbers? A percentage? Seems more like a poorly written news article without it. If its a 1 or 2% difference its ridiculous to push a new vaccine on children and people who have robust antibodies already. There are several studies stating the difference is very small. What were the different variables in this study? Were the patients mostly elderly? What about the memory b cells etc? Still lower? This text lacks context and real values, please update and comment on the other studies for context, thank you.
I would like to understand how (and why) the antibody binding to RBD affects the pathology of the disease. If the goal is to neutralize the disease, it seems to me more antibody binding (i.e. to all viral proteins not just the S-protein) would neutralize the virus faster (natural immunity). I am not seeing a correlation of the antibody binding locations to the disease state in this article, only the affinity of antibodies to RBD.
I think the point is that if the virus is blocked from binding to the cell, it will not cause disease because it will not be able to enter the cell. My understanding is that was the rationale for why they targeted the RBD in the mRNA vaccines.
I understand why they would target RBD, however, if a mutation occurs in this area it would most likely render the vaccine less effective compared to natural immunity with its more diverse antibody targets. That being said, we do not have a correlation with RBD binding to increased immunity in this article to see if it even matters.
I agree that mutations that result in alterations in the RBD could make the vaccines less effective.
Check out the article in Science (AAAS) from June 4 (“Prevalent, protective, and convergent IgG recognition of SARS-CoV-2 non-RBD spike epitopes”). The investigators examined convalescent sera from 4 patients and found that up to 80% of the patients’ antibodies targeted parts of the coronavirus spike other than the RBD, primarily the N-terminal domain (NTD). The NTD mutates more frequently than the RBD, and it is mutations in the NTD that account for many of the variants of concern.
So, both vaccine-induced immunity and natural immunity are susceptible to being diminished by mutations in the virus, though, based on the limited evidence in the Science article, it appears natural immunity is at greater risk of that than the immunity induced by the vaccines.
“…So, both vaccine-induced immunity and natural immunity are susceptible to being diminished by mutations in the virus, though, based on the limited evidence in the Science article, it appears natural immunity is at greater risk of that than the immunity induced by the vaccines….. ” Aren’t you assuming a lot? Has anyone studied natural immunity to the point of identifying all the epitopes targeted in natural immunity? Everything I have read indicates that natural immunity targets far more epitopes than the vaccine does, which would logically make it a more robust immunity more likely to protect against new variants, directly contradicting the claim that vaccine immunity is superior, when indeed it is logically inferior.
It does not necessarily follow (though it might be true) that the more epitopes targeted, the greater the immunity against the virus. If the antibody response to all the targeted epitopes is weak across the board, the virus could overcome the immunity no matter how broad it might be. Add to that the finding that the NTD mutates frequently, the portion of the antibodies directed against the NTD may be functionally weaker if a new exposure to a SARS-CoV-2 variant has a mutation in the NTD.
Since the virus requires an attachment to the cell wall to invade the cell, creating a robust immunity against the portion of the virus responsible for carrying out that function could be all that’s needed to prevent infection, however narrow that defense may appear.
My understanding is that the epitopes are simply markers identifying the antigen as an invader. The more epitopes identified, the harder it is for the antigen to escape detection, and ultimate destruction. That is why it is highly likely that acquired immunity is far superior to vaccinated immunity, as seems to be corroborated by the ” break through” case rates involving vaccinated immunity, compared to the reinfection rates of acquired immunity. This also is supported by the very early research by virologists at the beginning of the pandemic who analyzed COVID-19 and found it is a virus that does not substantially mutate, but rather, just slightly mutates, which is also supported by the fact that the case rate, hospitalizations, and deaths plummeted late January and February when herd immunity started to manifest itself before the vaccines were distributed to the public in mass. It the virus mutates drastically enough to evade immunity, those who were infected early in 2020 would have likely come down with it again and there would have been no substantial drop in cases, hospitalizations, and deaths. In addition, since the vaccines were all modeled on the original strain, they would now probably be totally ineffective, especially being they target just one main epitope, the spike protein. Given a choice between the 2 immunities, I would choose the acquired immunity hands down if it didn’t mean having to contract the disease. Too bad there is no vaccine designed around deactivated COVID-19 virus. I am confident it would be superior to the mRNA narrowly targeted ones.
(1) If the majority of the antibodies resulting from natural immunity target a more rapidly mutating epitope (NTD), then it does not necessarily follow that a mutated virus will be neutralized by those antibodies if the mutation should affect the epitope in such a way that it renders those antibodies less effective or neutralized. The same, of course, applies to the epitopes targeted by the vaccines, but they mutate less often than the NTD, so the variants may be less able to escape vaccine-induced immunity than that induced by infection. At this point, no one knows how the two compare, and it’s a moving target in any case, as SARS-CoV-2 continues to mutate. It is one of the more slowly-mutating RNA viruses, but with the number of people infected, it’s being given enormous opportunities to mutate, not on the basis that it mutates rapidly (it doesn’t) but on the basis that it is replicating trillions of times.
(2) Natural immunity does not always result in superior immunity compared to vaccine-induced immunity (though it more commonly does). Vaccines against tetanus, pneumonococcal disease, and HPV all protect against disease better than natural infections.
(3) We can’t know what we don’t measure. One estimate in the US of the number of people infected by SARS-CoV-2 (based on seroprevalence) was 4.8X greater than the known cases to date. Some of these were mildly symptomatic, and many were asymptomatic. In order to diagnose a recurrent infection in someone, they had to have been diagnosed in the first place, and it is clear that many (the majority) have not been. How many have had recurrent infections is unknown, but it could be a substantial number.
(4) I disagree with the contention that the cases plummeted in the winter due to herd immunity. There is a clear correlation with the institution of vaccinations in mid-December. While herd immunity likely played a role, the timing related to vaccinations is obvious.
(5) The vaccines are not “totally ineffective” against the current variants. One study out of Scotland showed the Pfizer vaccine to be 79% effective against infection by the delta variant, and other studies show the mRNA vaccines to be even more effective against symptomatic disease, hospitalization and death.
(6) The mRNA vaccines may prove to not be ideal vaccines, but they are pretty darn good. Anyone without proven immunity to SARS-CoV-2 should get vaccinated. Yesterday.
The vaccines were not being administered in December, except maybe to political insiders and medical professionals. The public had to wait 2 – 3 more months. I clearly remember the cases plummeted before the public starting getting vaccinated. In regards to all the epitopes natural immunity has as opposed to the monolithic immunity of vaccines, there are lots of “what if’s” you have put forth, along with an apparent assumption that natural immunity doesn’t include the spike protein as an epitope. If it does indeed include the spike protein, then it is hands down a broader based immunity because of the broader base of epitopes including the one the vaccine targets. The “data” seems to indicate that is the case, as has previously been pointed out here, in which Israel has seen far more vaccinated people come down ill with Delta than natural immunity people coming down ill with it. In any event, logic would dictate that either vaccinated people or natural immunity people would more than likely have a milder sickness the second time around than the first. Surely the immunity from the germ and immunity from the vaccine must give the body an edge compared to a naive case.
Sandra Lindsay at Long Island Jewish Medical Center in NY was the first person in the US given the vaccination with the (I presume) Pfizer vaccine outside clinical trials on December 14, 2020. Yes, they started with the healthcare workers. A lot of the infections were occurring in HCWs at that point. About 4 weeks later cases began to decrease in the United States.
I’ve enjoyed our discussions, but I have other things to do and I think I’ve done what I can do here. If you’re not yet vaccinated, please do so and encourage your friends and family to do so. Good luck to you.
I agree with you 100%!
Everything in the human mind is of dubious validity (some far more dubious than others). Nothing is simple, stands alone, nor is complete and accurate. I attempt to gauge the humility of the source when vetting information. The more the source addresses what it does not or cannot know, the more validity it is likely to possess and the less I can assimilate without undue mental examination.
The more the source projects closed minded arrogance, political bias, or ignorance (that differs from lack of knowledge or cognitive capacity), the quicker I will dismiss the source. I automatically dismiss any source or institution that offers, mandates, or repeats over and over again redundantly a simplistic, short sighted, narrow minded “one size fits all” definition or solution to any problem, even more so a medical one.
The etiology, epidemiology, treatment, prognosis, and general profile of any contagion is complex. There is always room for improvement in the comprehension and application of all aspects of a contagion.
if there are 4 patients examined how do you get 80%? 3 out of 4 is 75%and 4/4 is 100% So how do you get 80% out of 4 examined patients?
“…80% of the patients’ antibodies…”
80% of the antibodies, not 80% of the patients. Note the possessive apostrophe at the end of “patients.”
Please search for CoronaVac (Chinese) as an example! There are vaccines using deactivated COVID-19 virus! But they are still not widespread. Turkey and Chile (many vaccinated) uses it for example . . .
This. Is this actual comparison of actual measured cases of reinfection to those who are infected after getting the vaccine? As a covid nurse who cares for patients for over a year who took my mask off at time so terrified hard of hearing patients could hear me and my reassurances, I have seen my natural immunity was very robust. And as we sit here, at least 5 vaccinated Texas state legislatures are sitting in DC after testing positive. I want to know how much increase, if at all, getting vaccinated now would give me before assaulting my immune system again by getting the vaccine. I don’t think I am unjustified in worrying at more assaults could trigger a more significant auto-immune condition when I highly suspect I have at least one mild condition that I just haven’t addressed. If, as I suspect, my natural immunity is very similar to vaccine immunity ( and likely greater than the J&J ), why can’t I let my immune system rest and just get a booster in the future if needed?
Thank you for your comment. I too am a nurse and I have not received the vaccine. I had COVID in Sept 2020, moderate case with some residual symptoms. I am on 2 immunosuppressants and am constantly being badgered and belittled for not receiving the vaccine. As I already have an autoimmune disease, I feel that it would be an assault to my immune system to get the vaccine. I too would like to know how much of an increased boost the vaccine would provide to my immune system. I have yet to find an answer that was not biased in one way or another. I can only assume that with the truly limited amount of info we have about the virus itself and the vaccine that targets it, those answers will remain to be seen for at least another couple of years.
CRabon and Kristen – Check out the article that just appeared in Israel National News entitled “Natural infection vs vaccination: Which gives more protection?” Israel is doing a much better job than the U.S. tracking everything and reporting it out. From the article: “More than 7,700 new cases of the virus have been detected during the most recent wave starting in May, but just 72 of the confirmed cases were reported in people who were known to have been infected previously – that is, less than 1% of the new cases. With a total of 835,792 Israelis known to have recovered from the virus, the 72 instances of reinfection amount to 0.0086% of people who were already infected with COVID.
By contrast, Israelis who were vaccinated were 6.72 times more likely to get infected after the shot than after natural infection, with over 3,000 of the 5,193,499, or 0.0578%, of Israelis who were vaccinated getting infected in the latest wave.”
Mind you, this is in a nation that was vastly vaccinated with Pfizer. The stats out of the U.K., where most people received AZ, is much worse for the vaccinated. And check out the study “Comparison of Neutralizing Antibody Titers Elicited by mRNA and Adenoviral Vector Vaccine against SARS-CoV-2 Variants.” To summarize this: “The increasing prevalence of SARS-CoV-2 variants has raised concerns regarding possible decreases in vaccine efficacy. Here, neutralizing antibody titers elicited by mRNA-based and an adenoviral vector-based vaccine against variant pseudotyped viruses were compared. BNT162b2 and mRNA-1273-elicited antibodies showed MODEST neutralization resistance against Beta, Delta, Delta plus and Lambda variants whereas Ad26.COV2.S-elicited antibodies from a significant fraction of vaccinated individuals were of LOW neutralizing titer (IC50 <50)."
So the real world data that is coming out is definitely in favor of the immunity of the naturally recovered being superior to immunization. And yet, our immunity is still not recognized. It is SO frustrating and, frankly, discriminatory in my opinion to the MILLIONS of us who were on the front lines through the pandemic and, through no fault of our own, caught and recovered from the virus.
There is no evidence that suggest people with auto-immune diseases reacted badly to vaccines. Especially in people on immunosuppressants immune response is usually very mild and wanes quickly. Almost one year after infection you’re most likely unprotected. Unless you fight off the virus in the meantime which is possible given your occupation.
I myself has a autoimmune disease, have liver transplant, use immunosuppresion, got both doses of Pfizer with no issue, but my antibodies are still low. Now I wait if there’s gonna be third booster for people like me.
Long story short, don’t go by your assumptions. If you have doubts consult your immunologist. There is lot of evidence out there.
Agree, not enough facts, too much propaganda. Anyone knows why FDA is “not recommending” evaluating antibodies after vaccination? How else we will know if we have an immunity?
I think the obvious answer is that the trials that occurred before the vaccines were authorized showed that the vast majority of those vaccinated had robust antibody levels, and to now determine antibody levels in every recipient would be a HUGE expenditure as a nation. Those monies are much better directed elsewhere.
Yet, vaccinated persons still get COVID and thus may be even more responsible for mutations as the virus continuously attempts to circumvent any defenses. By not letting natural immunity win, it could indeed turn into a super-virus and be resistant like we’re seeing with the prevalence of prescribing antibiotics for various infections.
It’s a feel good thing now, but as soon as the first mutation breaks thru in large numbers (and it will), vaccines will have been a false hope.
Common Sense, I’m not sure what you’re saying makes any sense. First of all, super-bugs are only super in that it evades the drug you’re trying to kill them with. It doesn’t suddenly give them other abilities. Second, there’s a reason that physicians use combination chemotherapies to minimize cancer cell mutations, and combination antibiotics to minimize antibiotic resistance. Honestly it just seems like you’re someone without any training in biology who chose to come to a conclusion without consulting any relevant resources or experts.
You nailed it . . . In my case, I’ve chosen my own common sense . . .
Too bad science doesn’t work with your own common sense
Mutations are the result of spreading within and between persons. Mutations occur when the virus replicates, but replicates with errors.
Vaccinated individuals are less likely to get infected, and less likely to spread the virus, reducing the chance of it replicating and producing errors (mutations).
Vaccines in no way promote mutations, they do the opposite – they prevent mutations from happening as widely because they reduce the spread and replication.
Vaccines certainly can promote mutations, and in a catastrophic way. Look up the term “leaky vaccines” which is the type our new vaccines are. And consider that the entire first year of Covid we had almost no mutations, and since the vaccines have rolled out we have new variants popping up frequently.
We have only recently scaled up actual testing and reporting for variants which is why they seem more frequent. But almost all of the variants of concern have come out of low vaccination places – Brazil, South Africa, India. Every virus replication is an opportunity for mutation, every mutation is an opportunity for increased fitness. More transmissible variants arise faster with more infections.
There have been variants from time 0. There was a European variant that was much more transmissible from the early days of the pandemic. In the U.S. the east coast had the European variant while the west coast saw the more wild type asian strain. East coast was much harder hit early on partially because of this more transmissible variant.
This paper demonstrates that natural infection is more “leaky” than the mRNA vaccines. Given all of that, vaccination is the best option.
Natural infection is not more “leaky” than a vaccine based on one strain, a vaccine that doesn’t fully sterilize the virus. Problem is, the paper is only comparing antibodies as the means of protection, which is a fallacy. We know there are several other mechanisms to immunity, particularly in those naturally infected. There is a significant amount of bias in the interpretation of this paper.
And sure, there were a few variants popping up last year, particularly in the UK, South Africa, and Brazil. Guess where Pfizer did their trials? UK, South Africa, and Brazil. Coincidence? Not to mention, cases were skyrocketing all last year, but this year cases are down, vaccines are up and variants are skyrocketing. It’s pretty clear what’s going on.
Replying to Brian M’s comment.
“And sure, there were a few variants popping up last year, particularly in the UK, South Africa, and Brazil. Guess where Pfizer did their trials? UK, South Africa, and Brazil.”
No, not the UK. According to Pfizer, “A breakdown of the diversity of clinical trial participants can be found here from approximately 150 clinical trials sites in United States, Germany, Turkey, South Africa, Brazil and Argentina.”
Brian M, you have the cause and effect backwards. Pfizer did the majority of their study in the US and then later on added the areas that had the mutations to see if they were effective. They didn’t cause the mutations, they followed the mutations. Also, the study population was such a tiny fraction of the overall population and the fraction that actually got the disease a tiny fraction of the study population, so that couldn’t have possible been the cause of the mutations. Finally, a mutation gains in prevalence because it spreads faster than the others that are out there. The Pfizer vaccine has been shown to be effective against all of them, so it is the unvaccinated people that are causing the mutations to gain ground, not the vaccinated people. This is further evidenced that the delta variation is spreading faster in the areas of the US that have the lowest vaccination rates.
In the last few days there have been an average of about 300,000 tests per day as opposed to 2.2 million in a day in Jan 2021. How canyou say that testing has been “scaled up” when the actual number show a decrease in testing in th USA.
Excellent point but I disagree because breakthrough infections are only at .08%. This new mRNA platform can by modified quickly enough to clamp down hard on any new variants.
Your concern for superbugs is valid but antibiotic abuse was mostly agricultural not from treating humans and we learned from it. Science can be abused or used wisely.
How about we stop crowding animals in filthy conditions? Here’s hoping we grow up as a species regarding ethical food production & regulation.
How do you know the number of breakthrough cases. They stopped testing vaccinated people as there were too many PCR positives. Quite amazingly, Asymptomatic no longer matters. So take all the asymptomatic cases of unvaccinated out of the former count to equalize the data.
You can’t get a positive test for Covid-19 any more often from an m-RNA vaccine than not being vaccinated because the test is looking for live virus. There is no live virus in the vaccine. Other types are vaccines such as ones that use attenuated or killed virus are a different story.
Right. Remarkably, the cited study has found that the vaccine elicited antibodies mostly target RBD sites 456 and 484. The mutation E484K. IT is found in variants B.1.351 (“South African”), P.1 (“Brazilian”), and others.
This might be a reason why Moderna created a special version of the vaccine against B.1.351 and shipped it to SA.
I learned that mutations are random and therefore do not depend on the presence of absence of external forces. The survival of mutant forms (as that of the wild type) depends on external forces. Consequently vaccines and medicines should reduce not increase the incidence of variant forms.
That’s not all true. Yes, you can still get infected if you’ve been vaccinated, but it’s WAY LESS likely and usually way less severe. The vaccine doesn’t have to provide sterilizing immunity to be extremely effective at controlling the pandemic. If people were getting vaccinated at the rate we really need, there would be less opportunity for variants to arise (globally, not just locally). And if we end up needing boosters for a an escape mutant, it won’t be a big deal and I will gladly accept when it is offered to me.
How does the J and J vaccine hold up against remaining vaccine
It appears that the J&J and AZ are only showing a 33% efficacy against the Delta variant at this time. See the study “Comparison of Neutralizing Antibody Titers Elicited by mRNA and Adenoviral Vector Vaccine against SARS-CoV-2 Variants” To summarize: The increasing prevalence of SARS-CoV-2 variants has raised concerns regarding possible decreases in vaccine efficacy. Here, neutralizing antibody titers elicited by mRNA-based and an adenoviral vector-based vaccine against variant pseudotyped viruses were compared. BNT162b2 and mRNA-1273-elicited antibodies showed modest neutralization resistance against Beta, Delta, Delta plus and Lambda variants whereas Ad26.COV2.S-elicited antibodies from a significant fraction of vaccinated individuals were of low neutralizing titer (IC50 <50). The data underscore the importance of surveillance for breakthrough infections that result in severe COVID-19 and suggest the benefit of a second immunization following Ad26.COV2.S to increase protection against the variants. Also see the recent article "One dose of Johnson & Johnson COVID vaccine is ineffective against delta variant, study suggests" that just appeared in the Chicago Tribune. To summarize this: The new study has not yet been peer reviewed nor published in a scientific journal, and relied on laboratory experiments. But it is consistent with observations that a single dose of the AstraZeneca vaccine — which has a similar architecture to the J&J vaccine — shows only about 33% efficacy against symptomatic disease caused by the delta variant.
An article in the NEJM (“Effectiveness of Covid-19 Vaccines against the B.1.617.2 (Delta) Variant”) from July 21 showed the effectiveness of the AZ vaccine to be 74.5% against the alpha variant and 67.0% against the delta variant (after 2 doses).
But what about the hospitalization and death rates? I heard that in England, and I would assume elsewhere where the Delta variant is reportedly on a tear, those rates are quite low. I heard that the Delta strain is a more mild strain. If this is true, shouldn’t the alarmist hype and over the top measures like mask earing and lockdowns come to an end? Seriously, if these new cases are almost all like a case of catching a cold, then the hospital resources should not be strained and when combined with the current knowledge on how to effectively treat the few serious cases, should put us back to life as usual at this point. For point of reference, we do not treat the Flu with this level of alarmism and I believe at this point the Flu is likely a bigger health threat than COVID-19.
The Delta variant being “a more mild strain” would be news to me; I’ve not read that.
An article out of Scotland (Lancet, June 14, “SARS-CoV-2 Delta VOC in Scotland: demographics, risk of hospital admission, and vaccine effectiveness”) showed the risk of hospitalization for someone infected with the Delta variant was twice the risk of someone infected with the Alpha variant.
That’s just one study, but it’s one that argues for increased virulence of the Delta variant, not less. At this point no one yet knows, it appears, how the Delta variant ranks among the different strains of SARS-CoV-2 in terms of virulence. What we do know, though, is that people are still being hospitalized and dying from it.
History has shown that underestimating one’s enemy in war often leads to increased casualties. I think the same lesson applies to SARS-CoV-2, no matter which variant we’re talking about.
If the Delta strain is such a deadly strain, why have the death rates plummeted so low in the USA, according to ” the data?” The death rate in the USA is now well below the historic death rate from Influenza . . .
Vaccines, along with better management of those infected based on experience with previously infected patients since the pandemic began.
“How Immunity Generated from COVID-19 Vaccines Differs from an Infection”. This a very interesting study. Do you have reference of studies for immunity generated by other vaccines?
Researchers find long-lived immunity to 1918 pandemic virus.
Do you have a reference for us re “Researchers find long-lived immunity to 1918 pandemic virus,” please?
Search for “Neutralizing antibodies derived from the B cells of 1918 influenza pandemic survivors” in the journal Nature dated 17 August 2008. Nature, Volume 455, 532–536 (2008).
Just a month ago, it was reported on this blog that natural immunity heavily targets other parts of the spike protein, including the S2 subunit and the NTD (Ippolito, Lavinder et al.). On June 8th, in the NIH Research Matters article “How COVID-19 variants evade immune response” the following is stated “…antibodies targeting sites outside of the RBS could protect against a range of virus variants.” The researchers found that naturally acquired antibodies to sites other than the RBS (the site of most variants of concern) are effective in neutralizing the virus, even with the variants of concern. Both of these studies indicate that solely focusing on the RBD does not indicate the effectiveness of an immune response, particularly in the context of naturally acquired immunity. … Wouldn’t it make sense to look at immunity in a more complete manner? It would seem that only looking at the RBD proves nothing, since it is discounting all of the other antibodies, as well as t- and b-cell responses observed with naturally acquired immunity.
Emily – I agree and was going to make the SAME comment. It is obvious that the S1 spike protein is only part of the answer and with an enormous population being vaccinated against just this one aspect when the pandemic is still running rampant, it only makes sense that the virus will find a way in through one of the other many pathways. Just take a look at the loss in efficacy with the Delta variant among vaccinated people, and this is only after a small amount of time. The immunity of a naturally recovered person is much broader and other recent studies have found that the immunity was actually better against other newer variants than that of vaccinated individuals.
Ms. Giannini can you point me to the study that showed natural immunity was more protective against newer variants than vaccine induced immunity? Thank you!
Yes, I’d very much like to see that study as well.
I can’t post a direct link because the NIH always rejects my comments when I do. The paper has been peer reviewed and accepted for publication in Open Forum Infectious Diseases. Here is a summary and you can just google for the actual study: “Our data, as well as the results from other groups, shows that the T cell response to COVID-19 in individuals infected with the initial viral variants appears to fully recognize the major new variants identified in the UK, South Africa and Brazil,” said Andrew Redd of the NIAID and Johns Hopkins University School of Medicine who led the study.
The researchers analyzed blood from 30 people who had recovered from COVID-19 before the emergence of the new more contagious variants.
From those samples, they identified a specific form of T cell that was active against the virus, and looked to see how these T cells fared against the concerning variants from South Africa, the UK and Brazil.
They found the T-cell responses remained largely intact and could recognize virtually all mutations in the variants studied.
The findings add to a prior study that also suggested T cell protection appears to remain intact against the variants.
Also see “Cross-Reactive Neutralizing Antibody Responses Elicited by SARS-CoV-2″ in the New England Journal of Medicine.”
Replying to Ms. Giannini.
Thank you for that information. I was able to access the article. My concern with it is that, while the T cells recognize the variants, the article says nothing about how robust and effective the responses to those variants are. T cells recognize HIV and HPV, but in a large majority of those infected, do not neutralize the virus. Recognition and eradication are two separate attributes.
D Hart – Did you also look at the other study I mentioned in my comment [Cross-Reactive Neutralizing Antibody Responses Elicited by SARS-CoV-2 501Y.V2 (B.1.351) in the New England Journal of Medicine]? Also, I would like to refer you to a recent article entitled “Natural vs Vaccine Immunity for COVID: Is One More Effective?” — Virologist Vincent Racaniello and Marty Makary discuss the mechanics of immunity against COVID-19. And finally, be sure to read Xiaocong Y, Tsibane T, McGraw P, et al. Neutralizing antibodies derived from the B cells of 1918 influenza pandemic survivors. Nature 2008. Please let me know your thoughts as I am curious.
I would like to point out that the news has many stories of break through infections and hardly any of re-infections.
Sometimes professionals overlook what is standing right in front of them because they are so focused on the trees, that they overlook the forest. To you professionals here, reflect on these obvious and blatant facts 1) The press has enthusiastically and vigorously reported every negative aspect regarding COVID-19 (real and imagined) since the pandemic started. 2) At this point in time, well over a year into this pandemic, if natural immunity does not impart robust and lasting immunity against the original strain and the variants, there would be a vast amount of reinfection cases, and the press would be reporting it 24/7/365. The fact that they are not, in itself is solid proof that COVID-19 survivors enjoy lasting immunity from all the variants thus far discovered. Like camping in the wilderness, it isn’t always what you hear that tells you a bear is approaching. Sometimes it is the sudden silence of the crickets and/or frogs that tells you a bear is approaching. It isn’t always what you hear that informs you. Sometimes, it is what you DON’T hear that informs you. Step back and take a look at the forest.
Yes. Even the CDC and WHO themselves state reinfection after natural immunity is rare. How rare, no one knows because they do not reference any reinfection cases. I have followed this issue since covid began and the first T cell study came out. The last I could find, there were only 52 documented reinfections in the ENTIRE WORLD. Now THAT is representative of my God given immunity. Thank You Jesus!
On the other hand, breakthrough hospitalizations and deaths of fully vaccinated is in the thousands documented by the CDC.
I will stick with what I was born with, thank you . . .
I have no good idea how many breakthrough infections, or how many re-infections, occur. However, I think it likely that infections occur in both instances and, because of the pre-existing (though not entirely 100% protective) immunity (whether vaccine-induced or natural), the infections very often are either asymptomatic or are mild enough to not prompt those infected to seek medical advice and, therefore, confirmation of the infection.
It is interesting to note the logical process of this article. We do know that vaccinated people are still getting COVID, so we have to take the claim that the vaccine is better at handling variants with a degree of skepticism. If antibodies are reliable to provide immunity APART from variants, then shouldn’t that be treated as reliable and long lasting? In other words, we don’t catch the same virus twice (let the more astute correct me please if this is wrong)
So if my naturally acquired immunity is good for only one variant, but absolutely so, and the artificially acquired immunity is always described carefully as a reducer — not an eliminator — of infection, then the quality claim that variant protection breadth makes the vaccine a better immunizer has to come with a disclaimer, does it not? In other words, the antibodies from each are admittedly different, and perhaps shouldn’t be framed as one being superior to the other. Naturally acquired ones are specific, and the bio-hacked ones are generic. There are two variables at least… variant breadth and virus match reliability (readers here have more refined descriptors than I) . . .
The sited study does not say what this article claims it says. Figure 1 of the sited study shows that patients that were exposed to SARS2 and recovered required less antibodies to neutralize SARS2 than vaccinated individuals in the short term and had similar NT50 in the long term. In fact, the study shows that sera from vaccinated individuals was highly susceptible to RBD depletion while sera from convalescent patients was not until 3 months post infection. This means that vaccinated individuals would be more susceptible to reinfection by SARS2 variants with a mutation in the RBD in the short term than convalescent patients. Figures 5 does show that sera collected after 3 months from vaccinated individuals is better at neutralizing SARS2 with mutations in the RBD compared to sera collected from convalescent patients 3 months post-infection, but it seems disingenuous that the same data was not provided for the one month group given that this group should show the opposite effect. It is even concerning that data for sera from convalescent in Figure 1 was collected by a different group than the authors of the sited paper and looks drastically different than the data for sera from convalescent patients that was collected by the authors. In the context of an ongoing pandemic it seems like the convalescent patients would be better protected with immunity that is less dependent on single epitopes that would be present during the time course of a mutating viral pathogen. To conclude the sited study in no way supports the claim that “The new evidence shows that protective antibodies generated in response to an mRNA vaccine will target a broader range of SARS-CoV-2 variants carrying “single letter” changes in a key portion of their spike protein compared to antibodies acquired from an infection” because data present in Figure 1 indicate otherwise and the sample was not tested with the mutants.
Exactly.
Thank you for explaining that. I have had COVID 19 and I (after 8 months) had >250 and I do not believe I need the vaccine and in fact have heard of instances of people who had COVID then got the vaccine and are having some varying issues, which they were told may not be because of the vaccine . . .
Now we know that your rebuttal to this blog’s over-reach is correct. New research proves that Dr. Collins conclusions above are incorrect as evidenced in the Cleveland Clinic study. The Cleveland Clinic study shows that while COVID-19 infection in previously vaccinated individuals (break-through infections) are rare, they do occur and have been documented in countless studies. Meanwhile, the Cleveland Clinic study sowed that exactly 0% of convalescent patients were re-infected with COVID-19. Conclusion – vaccines are effective but not perfect while natural immunity as a result of previous COVID-19 is the most effective protection against infection with COVID-19.
If there is a CC study that shows 0% of convalescent patients were re-infected with SARS-CoV-2, the study is either defective (number of patients too small, perhaps) or they didn’t allow enough time to pass for reinfection to occur. There may be other explanations.
You’ve got people just on this very forum attesting to the fact that they’ve had reinfections. Extrapolate that to the rest of the population with initial COVID-19 infections to better assess how likely reinfections are.
If you haven’t done so already, look at the study in The Lancet titled, “SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: a large, multicentre, prospective cohort study (SIREN).” It showed that 16% of people with previous SARS-C0V-2 infections were reinfected at a median of 7 months. And the only variant they dealt with (in addition to the original strain) was the Alpha variant.
The fact is that those who have had the misfortune of having been infected with SARS-CoV-2 can be infected again, and their risk is far from trivial. Until someone can derive a reliable metric (currently nonexistent) of some sort that can predict with a high degree of confidence what the risk of reinfection is in any one person, assuming one is protected simply because they previously had a SARS-CoV-2 infection is unwise. Unless they have a medical contraindication to being vaccinated (ideally a decision arrived at in conjunction with their personal physician), vaccination is definitely what should occur. Maybe one shot, maybe two, but certainly something.
This article missed the fact that people previously infected with COVID-19, have made antibodies against every protein in the virus, not just the Spike protein. It also fails to mention research that shows T-cell immunity after COVID-19 infection is long lasting and is just as an important component of immunity as is neutralizing antibodies.
Matt – Agreed! Unfortunately many people will read this blog and believe the headline and not dig any deeper. This is very important, as businesses are looking to the NIH when setting COVID policy, such as whether or not to mandate employees to be vaccinated who have already been exposed and recovered. I would also like to point out the study “CD8+ T cell responses in COVID-19 convalescent individuals target conserved epitopes from multiple prominent SARS-CoV-2 circulating variants.” To summarize this study: “This study examined whether CD8+ T-cell responses from COVID-19 convalescent individuals (n=30) potentially maintain recognition of the major SARS-CoV-2 variants (n=45 mutations assessed). Only one mutation found in B.1.351-Spike overlapped with a previously identified epitope (1/52), suggesting that virtually all anti-SARS-CoV-2 CD8+ T-cell responses should recognize these newly described variants.”
This blog post makes absolutely no sense. In a past blog post dated May 18th with title “Human Antibodies Target Many Parts of Coronavirus Spike Protein” https://directorsblog.nih.gov/2021/05/18/human-antibodies-target-many-parts-of-coronavirus-spike-protein/ Dr. Collins states the following:
“the vast majority of antibodies—about 84 percent—targeted other portions of the spike protein than the RBD. This suggests a successful immune response doesn’t concentrate on the RBD. It involves production of antibodies capable of covering areas across the entire spike.”
“Also noteworthy, about 40 percent of the circulating antibodies target yet another portion of the spike called the S2 subunit. This finding is especially encouraging because this portion of SARS-CoV-2 does not seem as mutable as the NTD segment, suggesting that S2-directed antibodies might offer a layer of protection against a wider array of variants.”
“Taken together, these findings will prove useful for designing COVID-19 vaccine booster shots or future vaccines tailored to combat SARS-COV-2 variants of concern.”
These statements imply that natural immunity covers a wider array of sites on the SARS-CoV-2 Virus and offers better protection against variants than current vaccines. It also states outright that the study of the human body’s natural immune response will be used to design better vaccines in the future.
Please explain to me why the CDC and NIH continue to imply that natural immunity is somehow inferior to vaccine immunity and why the NIH is only providing “I GOT MY COVID-19 VACCINE” images to be included as part of email signatures other than to discriminate against employees who have had the disease and have chosen not to be vaccinated?
John – I agree with your point. As the wife of an essential employee (Corrections Officer), my family was basically forced to be exposed to the virus. I now feel like our immunity is being discriminated against for no good reason. It has also been stated that naturally immune individuals are 2-3X’s more likely to suffer from severe side effects as a result of taking the vaccines. If our immunity is as good (or better) than a vaccinated individual, why subject us to the risk needlessly. Unexplained issues such as this are what is causing a loss of faith in the NIH and CDC.
It has also been shown that many of those with long term chronic effects from getting Covid have finally been cured once they got the vaccine.
Can you cite a source?
Steve – if you would, please site your sources.
The cited study finds that vaccine-elicited antibodies target mostly the same spike RBD sites 456 and 484 as the naturally acquired antibodies, except for the first 2-3 months. They can be disrupted by any mutation around any of these sites. The cited study shows that the vaccine-elicited immunity is even more focused on the RBD than was expected
Unlike vaccine-elicited antibodies, the naturally acquired antibodies target more epitopes on the spike, M- & N-proteins, and non-structural proteins.
The coronavirus variants have half-way escaped the vaccine-elicited humoral immunity, and are likely to escape it nearly completely by the fall
Of course, there remain specific T-cells, which will become the first line of defense after 6-9 months since vaccination, but they are weaker, and are likely to lead to proliferation of variants that can evade them, too.
You say “Of course, there remain specific T-cells, which will become the first line of defense after 6-9 months since vaccination, but they are weaker, and are likely to lead to proliferation of variants that can evade them, too.” How do you know this, that “they are weaker” ?? and then, what about the rest of the immune system response besides antibodies?
This was a “process-oriented” study, essentially checking if one test predicts another test. The hope is that the outcome test.somehow correlates to something that matters. What we really need are meaningful outcome studies that show who had a new-variant (especially delta virus) COVID-19 conversion to positive, or more importantly, was hospitalized, comparing natural immunity to vaccination-induced immunity.
If vaccine acquired immunity is better than naturally acquired immunity, why are there so many articles about break through infections and no major stories about covid re-infections that actually cite statistics over empirical data. The article above used the word “may” a lot and seemed to be about what may happen and not about what actually happens in the real world. I feel that the NIH does good work, but when it comes to Covid, their desire to get people vaccinated has clouded their view and they ignore the real world benefits of natural immunity. I would never recommend any one get infected just to get immunity, but when it happens it should count for something and not be cast aside. If we include those with natural immunity that would increase the goal for head immunity to by maybe 10 percent.
If vaccination is superior to natural immunity, then why is the effectiveness of the Pfizer vaccine down to 64% against the Delta variant, as was recently reported by Israel? There are no news reports of recovered individuals contracting the Delta variant, so that in itself should serve as proof that vaccination is NOT superior to natural immunity. The fact that the NIH and CDC is not recognizing natural immunity as at least equal to vaccination is one of the main reasons why the public is losing faith in these government agencies. More antibodies to just one segment of the RBD obviously does not equate to better protection against this complex virus.
“There are no news reports of recovered individuals contracting the Delta variant…”
Search “Hindustan Times 10% of those who had Covid-19 were reinfected during April wave: Study” This is a report from India (probably obvious) that, as determined by antibody studies, strongly suggests that reinfections likely occurred in 10% of those previously infected. With the delta variant so dominant in India, I think it is highly likely that the reinfections were substantially from the delta variant.
D Hart MD – Assuming 10% were indeed reinfected recovered individuals, this would STILL indicate that natural immunity is at least as good, if not better, than vaccinated immunity, as Israel has reported that the vaccine effectiveness is down to 64% against the Delta variant. I would also like to point you to new national surveillance of possible COVID-19 reinfection, published by Public Health England (dated June 17, 2021). To summarize: The current data shows that there is a low risk of reinfection with SARS-CoV-2 among recovered individuals. There were 15,893 POSSIBLE reinfections with SARS-CoV-2 identified up to 30 May 2021 in England throughout the pandemic, out of nearly 4 million people with confirmed infections. This is equivalent to around 0.4% cases becoming POSSIBLY reinfected (no positive test – but even with assumed only 0.4% reinfection rate, which is still better than vaccinated rates). Out of this, only 53 were confirmed cases (making the number statistically close to zero for confirmed reinfections via positive PCR test – which in itself is suspect if the cycles are set too high as it would pick up DNA from old, non-active past exposures). This data shows reinfections from June 2020 up until the end of May 2021 (about a year). Current evidence suggests that most reinfections will not cause symptoms. There is currently no evidence that the Delta variant, or any other Variants of Concern, are more likely to cause reinfection than others.
I offered the information from India in response to your stated lack of knowledge of reinfections from the Delta variant. As I had noted in a previous comment, it seems apparent that there are reinfections (as well as breakthrough infections) that occur that are not suspected (asymptomatic) or are not confirmed (mildly symptomatic, as well as others). For how long immunity (vaccine-induced or natural) lasts remains to be determined, though evidence exists that natural immunity can and does wane, particularly in older populations (search for “The Lancet Assessment of protection against reinfection with SARS-CoV-2 among 4 million PCR-tested individuals in Denmark in 2020: a population-level observational study” as well as “The Lancet Risk of SARS-CoV-2 reinfection after natural infection”). The other advantage of immunity from a vaccine is that it substantially reduces the risk of systemic viral infection, an infection which has demonstrated significant adverse effects on multiple organs. Additionally, it is unknown if SARS-CoV-2 persists in a reservoir (such as is seen with EBV, VZV, HS, for example). Whether or not a reinfection would increase the likelihood of that potential future burden remains to be determined.
I would again argue that I do not see evidence that vaccine immunity is superior to natural. If you look at that Danish study, the rate of reinfection was found to be 0.65%, which again is superior to the breakthrough rate that is currently being reported for the vaccinated against Delta. In general I think the target of the current vaccines is too narrow in focus and it will come back to bite us. If you look at natural immunity, there are antibodies to multiple pathways. Take at look at “Biological and Clinical Consequences of Integrin Binding via a Rogue RGD Motif in the SARS CoV-2 Spike Protein” for example. There is danger that the emergence of receptor-binding domain mutations that increase infectivity may also enhance access of the RGD motif for integrin binding, resulting in viral strains with ACE2 independent routes of cell entry and novel integrin-mediated biological and clinical impacts. A better target might be the B cells or T cells. See the study “Two Different Antibody-Dependent Enhancement (ADE) Risks for SARS-CoV-2 Antibodies” for more info on the benefits of these alternative targets. And regarding your comment on the substantial reduction of systemic viral infection and persistance of the virus in a reservoir, I am in no way suggesting that people CHOOSE to get the virus versus vaccination. What I am stating is that millions of people already GOT the virus through no fault of their own, recovered, and now have immunity that needs to be recognized as being as good as, or even better than, vaccination immunity.
The target of the neutralizing antibodies in convalescent serum of 4 recovered patients showed it to be largely directed against epitopes such as the N-terminal domain, epitopes that are frequently mutated in SARS-CoV-2 variants. See “Science Prevalent, protective, and convergent IgG recognition of SARS-CoV-2 non-RBD spike epitopes” from June 4.
Time will tell how the different immunities compare. I hope they are both long-lasting but previous coronavirus infections typically have not resulted in long-lasting immunity.
“…..I hope they are both long-lasting but previous coronavirus infections typically have not resulted in long-lasting immunity…..” That’s not true. The La Jolla Institute for Immunology found SARs-1 survivors are still immune 17 yrs later. In addition, they have found recovery from COVID-19 appears to be long lasting as well, most likely for years . . .
I did not say infections from none of the coronaviruses result in long-lasting immunity, I said for the most part. Seven coronaviruses can infect humans. A SARS-CoV-1 infection may indeed result in long-lasting immunity in some. As for SARS-CoV-2, that remains to be seen. I, for one, would not characterize 18 months (or less) as “long-lasting.” Immunity to the other coronaviruses, that ones that typically result in URIs, can wane rather promptly. See “Nature Medicine Seasonal coronavirus protective immunity is short-lasting” from September 2020.
Also, the NEJM published a letter to the editor today (July 7, 2021) (“Infection and Vaccine-Induced Neutralizing-Antibody Responses to the SARS-CoV-2 B.1.617 Variants”) from investigators from Emory, Stanford, NIAID, and St. Jude Children’s Research Hospital looking at the neutralizing activity of SARS-CoV-2 convalescent sera (natural immunity), as well as the activity of sera from those with vaccine-induced immunity from both mRNA vaccines in use in the US, against the kappa and delta variants. The results were very favorable across the board, but there were a total of 6 convalescent sera (out of 24) that failed to demonstrate neutralizing activity above the threshold of detection against one or both variants, whereas all of the 25 sera from vaccinated individuals showed neutralizing activity against both variants.
Do you have a specific reference for what you posted here: “The La Jolla Institute for Immunology found SARS-1 survivors are still immune 17 yrs later. In addition, they have found recovery from COVID-19 appears to be long lasting as well, most likely for years . .”
Something I consider when people start throwing numbers around based on PCR –
Kary Mullis has said on more than one occasion not to diagnose with PCR. The doctors in India are trying to get the gov to lower the CT rate because they’re at 40 CT. Vaccinated are tested at 25 and unvaccinated at 40 here in the states (per CDC)
Mullis said at 45CT youre looking at 97% false positive. Fauci said you’re essentially looking at dead nucleai.
I think it needs to be considered when people start using PCR as any kind of metric.
If I’m wrong, please enlighten me. Anyone.
The high Ct value problem relates to the infectiousness/contagiousness of the person, not to whether or not they’ve been infected. For all practical purposes, you won’t get a positive PCR if you have not been infected, no matter what the Ct level is. If the level is high (somewhere in the 37-40 range–it varies with the lab), then that person likely is not infectious, though they could still have extremely low levels of viable virus (or nonviable virus). What Dr. Fauci had said was that a PCR that was positive only at a high Ct threshold was worthless for stating that someone was contagious. That is my understanding of how the interpretation of the PCR results work as it relates to the high Ct thresholds.
News reports do not matter. Scientific DOCUMENTED reinfections is what matters. And the FACT is, look up CDC and WHO for documented reinfections for COVID19 recovered persons. Now look up BREAKTHROUGH cases at CDC.
Another study, involving over 50,000 people, is the Cleveland Clinic study. Of that group, they found the people who came down with COVID-19 broke down into 3 groups. Those who never before had COVID-19 and were never vaccinated comprised 99.3 % of those who got COVID-19. Those who never before had COVID-19 and were vaccinated comprised .7 % of those who got COVID-19. Not even one of the people in the group who previously had COVID-19 and were not vaccinated came down with a reinfection of COVID-19. The study concluded that there “is no benefit” from vaccination for COVID-19 survivors. . . .
There’s no such thing as the perfect study, and the one mentioned in your comment offers an excellent example. The study was conducted on 52,238 mask-wearing employees in the Cleveland Clinic. Of all enrolled participants, 5% had previous SARS-CoV-2 infection, and only 47% of previously infected participants were vaccinated by the end of the study. Of the other 95% of enrollees—the non-infected group—59% were vaccinated. Please note that this is a retrospective study with all the inherent quality-control flaws of this approach. But the design was simple. Since staff members received frequent COVID tests (standard PCR) as employees of the Cleveland Clinic, the authors went back and looked in an in-house database for positive tests, vaccine status, and previous self-reported COVID status.
The authors found, “Not one of the 1,359 previously-infected subjects who remained unvaccinated had a SARS-CoV-2 infection over the duration of the study.” The authors concluded, “Individuals who have had SARS-CoV-2 infection are unlikely to benefit from COVID-19 vaccination, and vaccines can be safely prioritized to those who have not been infected before.” That conclusion sounds a little wobbly to me, starting with the weasel word “unlikely.” They really don’t know, but their retrospective look showed an interesting trend in a large, but wildly disproportionate, cohort of healthcare workers.
Pushing that aside, the authors real point comes in the second part of their conclusion: vaccines should be prioritized to the unvaccinated. That presumes a scarcity of vaccines, which is no longer the case in the U.S. The authors don’t say that the previously infected shouldn’t get vaccinated. From a public health perspective, stopping the spread of the virus is critical. If vaccinations of the previously infected can boost their immunity to an even higher level, that’s good for them, their families, and their communities. And yes, social responsibility matters.
Antibodies are short lasting. The CDC even warns people to not use them as the standard of immunity status. Humoral immunity with T cell memory is where the real boxing gloves of the immune system comes out. If the mucosal immunity and immunoglobulins allow the little credents aka COVSARS2 past them, then the punches of the t cells start flying into a knockout win for the host!
No matter how the conclusion is worded by the authors does not matter. What matters is the data, which shows there were ZERO reinfections. Stop twisting it all into knots.
There have been documented reinfections, not “ZERO.” A simple search turns up reports of them from many countries, including the US.
Unfortunately, the US is not set up to ascertain the number of reinfections and, as a result, they are underestimated. In order to do that, every positive viral culture would need to be genetically sequenced to differentiate a reccurrence vs. a reinfection. Very few laboratories do that.
For a more expansive discussion, search “KHN Why the U.S. Is Underestimating Covid Reinfection”
There have been 52 documented reinfections for covid recovered persons in the ENTIRE WORLD. Link where you find all these scientifically proven documented reinfections. Funny that CDC just says it is rare. Well how rare is it? 52 out of all naturally immune is damn rare of CDC does not even show any data for it. But here they show breakthrough serious hospitalizations and deaths at over 5100 cases for vaccinated. The vaccinated keep spreading vivid all around and to each other and yet they want more vaccines for even those with natural immunity. Makes perfect sense. NOT.
Look at the website of idsociety dot org. Check the “Vaccines FAQ” in the COVID-19 section, and then read the portion under “Efficacy of COVID-19 Vaccines.”
Again, confirming reinfections, based on the nature of the beast, is much more complex, time- and resource-intensive than confirming breakthrough infections. The former may be fewer, they may be similar, or they may be greater than the latter. No one knows. What we DO know is that reinfections occur. The number of DOCUMENTED reinfections is rare, very rare. Whether or not the number of ACTUAL reinfections is rare is not known.
Good, solid comment on the CC study. Thanks.
Yesterday NEJM Journal Watch published a good summary of a couple of recent articles (links to which are contained within) regarding benefits of vaccination in those previously infected. Search for “NEJM Journal Watch People with Past COVID-19 Benefit from Immunization”
Also note from prior NIH Director’s Blog on natural immunity that “about 40 percent of the circulating antibodies target yet another portion of the spike called the S2 subunit. This finding is especially encouraging because this portion of SARS-CoV-2 does not seem as mutable as the NTD segment, suggesting that S2-directed antibodies might offer a layer of protection against a wider array of variants. What’s more, the S2 subunit may make an ideal target for a possible pan-coronavirus vaccine since this portion of the spike is widely conserved in SARS-CoV-2 and related coronaviruses.” As I stated, natural immunity is broader in general than current vaccination immunity, which I strongly believe will prove to be a force against new variants as they continue to arise. Also see “SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls” which shows that T Cell immunity was still found in people who had recovered from SARS 17 years after recovery (and counting, as that was the length of the study period). I would call that long-lasting immunity. I can pull out study after study that back up my case that vaccinated immunity is not better than natural. However, I share your hope that both natural and vaccinated immunity will prove to be long lasting and this nightmare will just end.
There is evidence both for and against one type of immunity being better than another (more robust, longer-lasting, more likely to be effective against current and future variants, etc. – take your pick). Time will tell.
The more important question is whether or not those who have been infected with SARS-CoV-2 should or should not be vaccinated.
Re-infections do occur. From what I’ve seen, the stats are derived from those who have experienced severe COVID-19 infections. The likelihood of re-infections is low (about 0.7% in one series). However, the robustness of the immune response also has been directly correlated with the severity of the infection, so it seems probable (but, admittedly, not certain) that the far larger group of those with less severe infections (and particularly those with asymptomatic infections) have an immune response that will be suboptimal in preventing re-infection.
One must weigh for themselves the risks of vaccination vs. the risks of re-infection and make their choice. In my opinion, the risks of vaccination are minuscule given the potential benefit, even in someone previously infected. As I wrote, time will tell.
Dr Hart. You need to look at the study done by the La Jolla Institute of Immunology that looked at survivors of mild cases who had robust immunity some 8 months out. Their conclusion is that the immunity is likely long lasting, as in years. In addition, just recognize what you DON’T see. Reinfections, if they truly exist at all, are exceedingly rare as evidenced by the fact that A) Hospitalizations, deaths, and active cases have plummeted and have stayed plummeted for months, and B) The press, which is eager to report any negative development, real or imagined, would be reporting it 24/7 if it were occurring. The FACT they are NOT, almost 1 1/2 years into the pandemic, is solid proof that the immunity is long lasting. We are either at or very close to herd immunity at this point and none of the variants have varied enough to evade immunity of either COVID-19 survivors or the vaccinated, just as predicted by Dr. Mike Yaedon who was a chief scientific officer at Pfizer. He said all the variants are over 99% identical to the original strain and, therefore, do not vary enough to evade immunity . . .
One can speculate about duration of immunity after 8 months, one cannot ascertain duration of immunity after 8 months.
Reinfections DO occur; they have been documented with different genomes, many months apart. We likely underestimate them because such genetic sequencing is rarely done on a routine basis, the only way a recurrence/recrudescence could be differentiated from a reinfection. If you don’t look for it, you won’t find it.
It’s summertime when infections were expected to decrease on that basis alone. While the reductions are large and gratifying, I am concerned that there will be increases (unfortunately, already being seen in some areas of the country).
Ignore the lessons of Manaus, Brazil at one’s peril . . .
Dr. Hart, look at your statement: “However, the robustness of the immune response also has been directly correlated with the severity of the infection, so it seems probable (but, admittedly, not certain) that the far larger group of those with less severe infections (and particularly those with asymptomatic infections) have an immune response that will be suboptimal in preventing re-infection.” You’re guessing. Then you have the JR July 9 11:14 AM reply. Looks like we have two basic teams here: those thinking natural immunity is sufficient and those thinking vaccination prophylaxis is superior to natural immunity. Tho sometimes the twain are meeting in these very interesting comments. Now we have to read the references, especially the La Jolla reference.
Also, check out “Real-Time Learning Network” (a collaboration of the CDC and the Infectious Disease Society of America) at the website of the latter organization. Look for the Vaccines & Immunity portion and then Vaccines FAQ (Efficacy of COVID-19 Vaccines). There you will find a great discussion of the various findings of natural and vaccine-induced immunity, including reports of multiple cases of reinfections.
Documenting reinfections is exceedingly difficult. The initial infection needs to be confirmed with PCR or viral culture, something almost never done in those with an asymptomatic initial infection, and likely infrequently done with mild infections that those afflicted choose to not seek care or confirmation. And then even when documented, unless the reinfection occurs 3 months or more later (and is confirmed), reinfections typically are written off as a recurrence or recrudescence of the initial infection, not a reinfection. And while some of those cases may, indeed, be a recurrence of the initial infection, unless genome sequencing was done during both infections, there is no way to differentiate between a recurrent infection or a reinfection. This is why DOCUMENTED reinfections are rare. If you don’t look for them, you won’t find them. As the saying goes, absence of evidence is not evidence of absence.
Again, please look at the forest. If reinfections are so hard to identify because they are either A) Asymptomatic or B) So mild the person does not seek care, isn’t the crisis past? Also, because the data is not present, doesn’t that also indicate that you and the other alarmists are basing your conclusions on mere conjecture and supposition? In addition, Michael Yaedon may or may not have a checkered past, but it seems he is correct about the variants. Instead of conjecture and suppositions, he gave a cogent and logical explanation of how the immune system develops immunity when exposed to the whole germ during infection and also how the body develops immunity when exposed to a piece of the germ through vaccination. In both cases he explained that the immunity is multi faceted(more so when developed in response to the whole germ) and that a variant would have be be substantially mutated to evade immunity provided from either source. To date, none of the variants are substantially mutated, according to the virologists, and therefore have not evaded immunity acquired from the original strain or from the vaccine, as evidenced by the continuing waining of the caseloads, hospitalizations, and deaths. In contrast, the alarmists offer no data, because as you submit, there is none. All they offer are suppositions that the reinfections are under the radar because they are asymptomatic or minor cases unworthy of medical intervention, which even if true, means there is no crisis anymore, because wasn’t the crisis the ICU class severe illnesses? Which now begs the question, why are we still wearing masks? I see people driving in their cars alone, wearing masks. I saw a police officer riding a motorcycle, wearing a mask. I see people walking outside with no one else in sight, wearing a mask. Why? The alarmists remind me of “EXPERTS” back when I was young. At that time the “EXPERTS” cautioned against eating eggs, salmon, avocados, etc., because they are high in cholesterol, will plug your arteries, and give you an MI. For a while, I heeded their advice. Then I noticed some people who followed their advice were dropping dead with MIs. I also noticed some people who ate bacon cheese burgers were doing fine. Then one day, as I was driving through the country, and saw some cows, it dawned on me. Cows eat nothing but grass and grow fat. Cougars eat nothing but meat and remain lean. Gee, maybe it is more about what your body does with your food than what you eat. I came to the high confidence conclusion that genetics plays a far more major role in heart disease than does diet. Then subsequent to that observation, the “EXPERTS” discovered they had been wrong. They realized that eggs, salmon, and avocados are high in “good” cholesterol that actually help your heart be healthy . . .
As for the former employee at Pfizer, search for “Reuters fact check ex-Pfizer scientist.” That will give you a good perspective, I think, on how much weight to give to his opinions.
How many of the vaccines were/are being tested in any way on Animals and how much of this testing has given accurate performance results after reasonable periods of use by Humans?
What are/were the accepted alternative testing methods for Covid development, that don’t involve Animals?
“…..If vaccinations of the previously infected can boost their immunity to an even higher level, that’s good for them, their families, and their communities. And yes, social responsibility matters……” Indeed, SOCIAL RESPONSIBILITY MATTERS !!! It matters when INSISTING that people who have recovered from COVID-19 take an experimental vaccine that has generated a plethora of serious side effects in thousands of people to date, with no fore warning of these possible side effects, especially young people who are at higher risk of serious side effects of the vaccine than they are to a serious case of COVID-19. It also matters when to date, there has been NO DATA demonstrating ANY benefit by vaccinating COVID-19 survivors who are also no more likely, and indeed perhaps less likely, than vaccinated people who have never had COVID-19, to transmit COVID-19 to the uninfected. I do not believe MALPRACTICE is too strong a word in characterizing this dogmatic campaign insisting that COVID-19 survivors and young people get vaccinated. Another thing. Why is it that a substantial number of people working at CDC have decided against being vaccinated? THAT is an interesting question that begs an answer. At this point, it is most suspicious as to the motivations of the government that is proceeding with reckless abandon in the promotion of these vaccines, without regard to the risk/benefit to the recipient.
JR – AGREED! Given the data that has been coming in to date via NUMEROUS studies, there is no way anyone can conclude that vaccine-induced immunity is superior to natural immunity. There are just NO real facts to back up the claim. Stating that a recovered individual will benefit from vaccination due to the development of more antibodies to JUST a subsection of the RBD is very short sighted and, in my opinion, just grasping at straws, especially as we see the effectiveness of these vaccines diminish against new strains and Pfizer pushing for booster shots already. It seems pretty obvious that if you continue to vaccinate millions of individuals against just this one aspect of the RBD in the middle of a pandemic, the virus is just going to continue to be pressured to prioritize another entry target (look into research by Geert Vanden Bossche, among others, for more on this).
And yes, social responsibility should be extended to recovered individuals, who have been shown to have 2-3X’s more serious side effects from vaccination. The study that shows the substantially higher rate of serious side effects among previously recovered individuals who received one of the vaccinations is entitled “Self-reported real-world safety and reactogenicity of COVID-19 vaccines: An international vaccine-recipient survey.”
It should all be about risk versus benefit – not blindly implimented mandates and recommendations. These vaccines are definitely not “safe and effective” across the board and should not be marketed as such. Even official guidance from WHO dated May 10, 2021 entitled “COVID-19 Natural Immunity,” stated that “To conclude, available tests and current knowledge do not tell us about the duration of immunity and protection against reinfection, but recent evidence suggests that natural infection may provide similar protection against symptomatic disease as vaccination, at least for the available follow up period.” Contrary to this, the country is using the CDC/NIH recommendations to come up with mandates for employment and education which are hurting thousands of people while offering no real health benefit! I am against mandates in general, but if nothing else, mandate exemptions NEED to be granted for recovered individuals. And if these recovered individuals decide that they want to also be vaccinated, so be it, but it absolutely needs to be an individual choice.
Thank you Joanne for your comments, they have been enlightening. Do you have training in biology or virology, or are you just an avid reader?
Have you looked at “SARS-CoV-2 seropositivity and subsequent infection risk in healthy young adults: a prospective cohort study”? It is a decent study that indicates that natural immunity reduces infection by “only” 80%. (It was published on July 1, so it’s not fair to expect you to have seen it.)
Justin K – No I haven’t but I will for sure! Thanks for the heads up! Even still, if what Israel is saying is correct – that the effectiveness of the mRNA vaccines is down to 64% and we can only assume it is even lower for the others – 80% is still great. Plus I’m guessing that even if 20% ends up being the reinfection rate, the cases will be very mild.
I am stunned, reading your comments, by the incredible intelligence and grace of your answers. I am admittedly already convinced by my own research (and infection) that a vaccine would offer no increase in protection and possibly cause harm. I am a nurse in the federal system and waiting in fear for the mandate that will cause me to lose my job if I don’t comply. I have already decided that I won’t comply so I expect I will be out of work soon. Many of my peers feel the same way, but the coercive threat of job loss will ensure compliance. Already in my community private hospitals have initiated the mandate. How completely insane that even with the lack of evidence (regardless of the ‘assumption’ of reinfection) the healthcare community has abandoned the foundational principle to “first do no harm”.
In the mRNA vaccine, the lipid nanoparticle is absorbed by the host cell. The mRNA then gets the host cell to replicate the virus spike protein. Once the spike protein is produced, it is moved to the host cell membrane, and it is then exposed to the immune system T-cells and B-cells. This triggers the immune system. As part of the immune system’s response, is the host cell then attacked and killed by the T-cells and/or B-cells?
Concise explanation, but 1) where exactly is the LNP “absorbed by the host cell?” only in the deltoid area, or does the mRNA and LNP enter “other” host cells in different parts of the body, actually? And then these replicated spike proteins circulate to different parts of the body, to be confronted by the immune system?? 2) What % of LNP coated mRNA go to different parts in the body, if they do, actually? Do we know that? ty
I’m having difficulty understanding how the same RNA can result in different antibodies. The synthetic mRNA is a duplicate of a piece of RNA of the virus itself; the one that make the spikes of the virus that attaches to human cells.
Maybe it was already said, but.. many of those, who were vaccinated, were previously… infected by sars-cov-2, or sick on covid – some of them had knew about it (of course having in mind that covid tests works as we assumed), but many hadn’t – assuming, that the most covid cases in previously unvaccinated people were hidden (80% of cases?).
So – we can simply assume, that the vacccines immunity based.. on natural immunity. But it is granted for.. vaccines.
Which came first, the chicken or the egg? 🙂
The different patterns described in this study between the antibody response to vaccine-acquired immunity versus infection-acquired immunity, could be used as a quality control mechanism to detect mRNA vaccines which were inactive when administered.
Unless samples of the highly unstable mRNA vaccines are being routinely collected from vaccination clinics and tested for “point-of-injection viability”, there can be no way of knowing the true break-through infection rates associated with the mRNA vaccines.
Therefore, if antibody patterns typically associated with infection-acquired immunity, occur in individuals who have been vaccinated with either of the mRNA vaccines, some indication of “point-of-injection viability” might be extrapolated, if asymptomatic infection were controlled for.
“Point-of-injection viability” is a significant issue of concern to both sides of the vaccination debate, in that concerns about the stability of the mRNA vaccines has been part of a “muted conversation” now contributing to vaccine hesitancy and an unnecessary conspiracy of silence surrounding a key issue.
I totally understand how testing for vaccine viability at the point-of-injection might stir up additional pro and anti-vax anxieties, but it also makes a clear case for a booster shot, until such time as point-of-injection quality control data becomes part of the conversation.