microfluidics
Clinical Center Doctors Testing 3D-Printed Miniature Ventilator
Posted on by James K. Gilman, MD, NIH Clinical Center

Here at the NIH Clinical Center, we are proud to be considered a world-renowned research hospital that provides hope through pioneering clinical research to improve human health. But what you may not know is that our doctors are constantly partnering with public and private sectors to come up with innovative technologies that will help to advance health outcomes.
I’m excited to bring to you a story that is perfect example of the ingenuity of our NIH doctors working with global strategic partners to create potentially life-saving technologies. This story begins during the COVID-19 pandemic with the global shortage of ventilators to help patients breathe. Hospitals had a profound need for inexpensive, easy-to-use, rapidly mass-produced resuscitation devices that could be quickly distributed in areas of critical need.
Through strategic partnerships, our Clinical Center doctors learned about and joined an international group of engineers, physicians, respiratory therapists, and patient advocates using their engineering skills to create a ventilator that was functional, affordable, and intuitive. After several iterations and bench testing, they devised a user-friendly ventilator.

Then, with the assistance of 3D-printing technology, they improved the original design and did something pretty incredible: the team created the smallest single-patient ventilator seen to date. The device is just 2.4 centimeters (about 1 inch) in diameter with a length of 7.4 centimeters (about 3 inches).
A typical ventilator in a hospital obviously is much larger and has a bellows system. It fills with oxygen and then forces it into the lungs followed by the patient passively exhaling. These systems have multiple moving parts, valves, hoses, and electronic or mechanical controls to manage all aspects of the oxygen flow into the lungs.
But our miniature, 3D-printed ventilator is single use, disposable, and has no moving parts. It’s based on principles of fluidics to ventilate patients by automatically oscillating between forced inspiration and assisted expiration as airway pressure changes. It requires only a continuous supply of pressurized oxygen.
The possibilities of this 3D-printed miniature ventilator are broad. The ventilators could be easily used in emergency transport, potentially treating battlefield casualties or responding to disasters and mass casualty events like earthquakes.
While refining a concept is important, the key is converting it to actual use, which our doctors are doing admirably in their preclinical and clinical studies. NIH’s William Pritchard, Andrew Mannes, Brad Wood, John Karanian, Ivane Bakhutashvili, Matthew Starost, David Eckstein, and medical student Sheridan Reed studied and have already tested the ventilators in swine with acute lung injury, a common severe outcome in a number of respiratory threats including COVID-19.
In the study, the doctors tested three versions of the device built to correspond to mild, moderate, and severe lung injury. The respirators provided adequate support for moderate and mild lung injuries, and the doctors recall how amazing it was initially to witness a 190-pound swine ventilated by this miniature ventilator.
The doctors believe that the 3D-printed miniature ventilator is a potential “game changer” from start to finish since it is lifesaving, small, simple to use, can be easily and inexpensively printed and stored, and does not require additional maintenance. They recently published their preclinical trial results in the journal Science Translational Medicine [1].
The NIH team is preparing to initiate first-in-human trials here at the Clinical Center in the coming months. Perhaps, in the not-too-distant future, a device designed to help people breathe could fit into your pocket next to your phone and keys.
Reference:
[1] In-line miniature 3D-printed pressure-cycled ventilator maintains respiratory homeostasis in swine with induced acute pulmonary injury. Pritchard WF, Karanian JW, Jung C, Bakhutashvili I, Reed SL, Starost MF, Froelke BR, Barnes TR, Stevenson D, Mendoza A, Eckstein DJ, Wood BJ, Walsh BK, Mannes AJ. Sci Transl Med. 2022 Oct 12;14(666):eabm8351.
Links:
Clinical Center (NIH)
Andrew Mannes (Clinical Center)
Bradford Wood (Clinical Center)
David Eckstein (Clinical Center)
Note: Dr. Lawrence Tabak, who performs the duties of the NIH Director, has asked the heads of NIH’s Institutes and Centers (ICs) to contribute occasional guest posts to the blog to highlight some of the interesting science that they support and conduct. This is the 21st in the series of NIH IC guest posts that will run until a new permanent NIH director is in place.
The Perfect Cytoskeletal Storm
Posted on by Dr. Francis Collins
Ever thought about giving cell biology a whirl? If so, I suggest you sit down and take a look at this full-blown cytoskeletal “storm,” which provides a spectacular dynamic view of the choreography of life.
Before a cell divides, it undergoes a process called mitosis that copies its chromosomes and produces two identical nuclei. As part of this process, microtubules, which are structural proteins that help make up the cell’s cytoskeleton, reorganize the newly copied chromosomes into a dense, football-shaped spindle. The position of this mitotic spindle tells the cell where to divide, allowing each daughter cell to contain its own identical set of DNA.
To gain a more detailed view of microtubules in action, researchers designed an experimental system that utilizes an extract of cells from the African clawed frog (Xenopus laevis). As the video begins, a star-like array of microtubules (red) radiate outward in an apparent effort to prepare for cell division. In this configuration, the microtubules continually adjust their lengths with the help of the protein EB-1 (green) at their tips. As the microtubules grow and bump into the walls of a lab-generated, jelly-textured enclosure (dark outline), they buckle—and the whole array then whirls around the center.
Abdullah Bashar Sami, a Ph.D. student in the NIH-supported lab of Jesse “Jay” Gatlin, University of Wyoming, Laramie, shot this movie as a part his basic research to explore the still poorly understood physical forces generated by microtubules. The movie won first place in the 2019 Green Fluorescent Protein Image and Video Contest sponsored by the American Society for Cell Biology. The contest honors the 25th anniversary of the discovery of green fluorescent protein (GFP), which transformed cell biology and earned the 2008 Nobel Prize in Chemistry for three scientists who had been supported by NIH.
Like many movies, the setting was key to this video’s success. The video was shot inside a microfluidic chamber, designed in the Gatlin lab, to study the physics of microtubule assembly just before cells divide. The tiny chamber holds a liquid droplet filled with the cell extract.
When the liquid is exposed to an ultra-thin beam of light, it forms a jelly-textured wall, which traps the molecular contents inside [1]. Then, using time-lapse microscopy, the researchers watch the mechanical behavior of GFP-labeled microtubules [2] to see how they work to position the mitotic spindle. To do this, microtubules act like shapeshifters—scaling to adjust to differences in cell size and geometry.
The Gatlin lab is continuing to use their X. laevis system to ask fundamental questions about microtubule assembly. For many decades, both GFP and this amphibian model have provided cell biologists with important insights into the choreography of life, and, as this work shows, we can expect much more to come!
References:
[1] Microtubule growth rates are sensitive to global and local changes in microtubule plus-end density. Geisterfer ZM, Zhu D, Mitchison T, Oakey J, Gatlin JC. November 20, 2019.
[2] Tau-based fluorescent protein fusions to visualize microtubules. Mooney P, Sulerud T, Pelletier JF, Dilsaver MR, et al. Cytoskeleton (Hoboken). 2017 Jun;74(6):221-232.
Links:
Mitosis (National Human Genome Research Institute/NIH)
Gatlin Lab (University of Wyoming, Laramie)
Green Fluorescent Protein Image and Video Contest (American Society for Cell Biology, Bethesda, MD)
2008 Nobel Prize in Chemistry (Nobel Foundation, Stockholm, Sweden)
NIH Support: National Institute of General Medical Sciences
Body-on-a-Chip Device Predicts Cancer Drug Responses
Posted on by Dr. Francis Collins
Researchers continue to produce impressive miniature human tissues that resemble the structure of a range of human organs, including the livers, kidneys, hearts, and even the brain. In fact, some researchers are now building on this success to take the next big technological step: placing key components of several miniature organs on a chip at once.
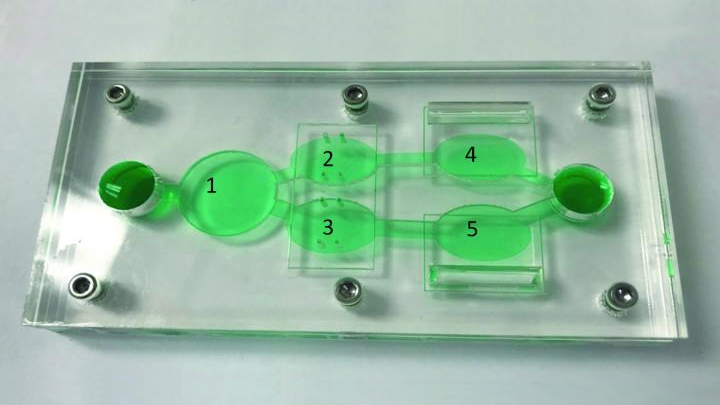
These body-on-a-chip (BOC) devices place each tissue type in its own pea-sized chamber and connect them via fluid-filled microchannels into living, integrated biological systems on a laboratory plate. In the photo above, the BOC chip is filled with green fluid to make it easier to see the various chambers. For example, this easy-to-reconfigure system can make it possible to culture liver cells (chamber 1) along with two cancer cell lines (chambers 3, 5) and cardiac function chips (chambers 2, 4).
Researchers circulate blood-mimicking fluid through the chip, along with chemotherapy drugs. This allows them to test the agents’ potential to fight human cancer cells, while simultaneously gathering evidence for potential adverse effects on tissues placed in the other chambers.
This BOC comes from a team of NIH-supported researchers, including James Hickman and Christopher McAleer, Hesperos Inc., Orlando, FL. The two were challenged by their Swiss colleagues at Roche Pharmaceuticals to create a leukemia-on-a-chip model. The challenge was to see whether it was possible to reproduce on the chip the known effects and toxicities of diclofenac and imatinib in people.
As published in Science Translational Medicine, they more than met the challenge. The researchers showed as expected that imatinib did not harm liver cells [1]. But, when treated with diclofenac, liver cells on the chip were reduced in number by about 30 percent, an observation consistent with the drug’s known liver toxicity profile.
As a second and more challenging test, the researchers reconfigured the BOC by placing a multi-drug resistant vulva cancer cell line in one chamber and, in another, a breast cancer cell line that responded to drug treatment. To explore side effects, the system also incorporated a chamber with human liver cells and two others containing beating human heart cells, along with devices to measure the cells’ electrical and mechanical activity separately.
These studies showed that tamoxifen, commonly used to treat breast cancer, indeed killed a significant number of the breast cancer cells on the BOC. But, it only did so after liver cells on the chip processed the tamoxifen to produce its more active metabolite!
Meanwhile, tamoxifen alone didn’t affect the drug-resistant vulva cancer cells on the chip, whether or not liver cells were present. This type of cancer cell has previously been shown to pump the drug out through a specific channel. Studies on the chip showed that this form of drug resistance could be overcome by adding a second drug called verapamil, which blocks the channel.
Both tamoxifen alone and the combination treatment showed some off-target effects on heart cells. While the heart cells survived the treatment, they contracted more slowly and with less force. The encouraging news was that the heart cells bounced back from the tamoxifen-only treatment within three days. But when the drug-drug combination was tested, the cardiac cells did not recover their function during the same time period.
What makes advances like this especially important is that only 1 in 10 drug candidates entering human clinical trials ultimately receives approval from the Food and Drug Administration (FDA) [2]. Often, drug candidates fail because they prove toxic to the human brain, liver, kidneys, or other organs in ways that preclinical studies in animals didn’t predict.
As BOCs are put to work in testing new drug candidates and especially treatment combinations, the hope is that we can do a better job of predicting early on which chemical compounds will prove safe and effective in humans. For those drug candidates that are ultimately doomed, “failing early” is key to reducing drug development costs. By culturing an individual patient’s cells in the chambers, BOCs also may be used to help doctors select the best treatment option for that particular patient. The ultimate goal is to accelerate the translation of basic discoveries into clinical breakthroughs. For more information about tissue chips, take a look at NIH’s Tissue Chip for Drug Screening program.
References:
[1] Multi-organ system for the evaluation of efficacy and off-target toxicity of anticancer therapeutics. McAleer CW, Long CJ, Elbrecht D, Sasserath T, Bridges LR, Rumsey JW, Martin C, Schnepper M, Wang Y, Schuler F, Roth AB, Funk C, Shuler ML, Hickman JJ. Sci Transl Med. 2019 Jun 19;11(497).
[2] Clinical development success rates for investigational drugs. Hay M, Thomas DW, Craighead JL, Economides C, Rosenthal J. Nat Biotechnol. 2014 Jan;32(1):40-51.
Links:
Tissue Chip for Drug Screening (National Center for Advancing Translational Sciences/NIH)
James Hickman (Hesperos, Inc., Orlando, FL)
NIH Support: National Center for Advancing Translational Sciences
Making Personalized Blood-Brain Barriers in a Dish
Posted on by Dr. Francis Collins

The blood-brain barrier, or BBB, is a dense sheet of cells that surrounds most of the brain’s blood vessels. The BBB’s tiny gaps let vital small molecules, such as oxygen and water, diffuse from the bloodstream into the brain while helping to keep out larger, impermeable foreign substances that don’t belong there.
But in people with certain neurological disorders—such as amyotrophic lateral sclerosis (ALS) and Huntington’s disease—abnormalities in this barrier may block the entry of biomolecules essential to healthy brain activity. The BBB also makes it difficult for needed therapies to reach their target in the brain.
To help look for solutions to these and other problems, researchers can now grow human blood-brain barriers on a chip like the one pictured above. The high-magnification image reveals some of the BBB’s cellular parts. There are endothelial-like cells (magenta), which are similar to those that line the small vessels surrounding the brain. In close association are supportive brain cells known as astrocytes (green), which help to regulate blood flow.
While similar organ chips have been created before, what sets apart this new BBB chip is its use of induced pluripotent stem cell (iPSC) technology combined with advanced chip engineering. The iPSCs, derived in this case from blood samples, make it possible to produce a living model of anyone’s unique BBB on demand.
The researchers, led by Clive Svendsen, Cedars-Sinai, Los Angeles, first use a biochemical recipe to coax a person’s white blood cells to become iPSCs. At this point, the iPSCs are capable of producing any other cell type. But the Svendsen team follows two different recipes to direct those iPSCs to differentiate into endothelial and neural cells needed to model the BBB.
Also making this BBB platform unique is its use of a sophisticated microfluidic chip, produced by Boston-based Emulate, Inc. The chip mimics conditions inside the human body, allowing the blood-brain barrier to function much as it would in a person.
The channels enable researchers to flow cerebral spinal fluid (CSF) through one side and blood through the other to create the fully functional model tissue. The BBB chips also show electrical resistance and permeability just as would be expected in a person. The model BBBs are even able to block the entry of certain drugs!
As described in Cell Stem Cell, the researchers have already created BBB chips using iPSCs from a person with Huntington’s disease and another from an individual with a rare congenital disorder called Allan-Herndon-Dudley syndrome, an inherited disorder of brain development.
In the near term, his team has plans to model ALS and Parkinson’s disease on the BBB chips. Because these chips hold the promise of modeling the human BBB more precisely than animal models, they may accelerate studies of potentially promising new drugs. Svendsen suggests that individuals with neurological conditions might one day have their own BBB chips made on demand to help in selecting the best-available therapeutic options for them. Now that’s a future we’d all like to see.
Reference:
[1] Human iPSC-Derived Blood-Brain Barrier Chips Enable Disease Modeling and Personalized Medicine Applications. Vatine GD, Barrile R, Workman MJ, Sances S, Barriga BK, Rahnama M, Barthakur S, Kasendra M, Lucchesi C, Kerns J, Wen N, Spivia WR, Chen Z, Van Eyk J, Svendsen CN. Cell Stem Cell. 2019 Jun 6;24(6):995-1005.e6.
Links:
Tissue Chip for Drug Screening (National Center for Advancing Translational Sciences/NIH)
Stem Cell Information (NIH)
Svendsen Lab (Cedars-Sinai, Los Angeles)
NIH Support: National Institute of Neurological Disorders and Stroke; National Center for Advancing Translational Sciences
Detecting Cancer with a Herringbone Nanochip
Posted on by Dr. Francis Collins

Credit: Yong Zeng, University of Kansas, Lawrence and Kansas City
The herringbone motif is familiar as the classic, V-shaped patterned weave long popular in tweed jackets. But the nano-sized herringbone pattern seen here is much more than a fashion statement. It helps to solve a tricky design problem for a cancer-detecting “lab-on-a-chip” device.
A research team, led by Yong Zeng, University of Kansas, Lawrence, and Andrew Godwin at the University of Kansas Medical Center, Kansas City. previously developed a lab-on-a-chip that senses exosomes. They are tiny bubble-shaped structures that most mammalian cells secrete constantly into the bloodstream [1]. Once thought of primarily as trash bags used by cells to rid themselves of waste products, exosomes carry important molecular information (RNA, protein, and metabolites) used by cells to communicate and influence the behavior of other cells.
What’s also interesting, tumor cells produce more exosomes than healthy cells. That makes these 30-to-150-nanometer structures (a nanometer is a billionth of a meter) potentially useful for detecting cancer. In fact, these NIH-funded researchers found that their microfluidic device can detect exosomes from ovarian cancer within a 2-microliter blood sample. That’s just 1/25th of a drop!
But there was a technical challenge. When such tiny samples are placed into microfluidic channels, the fluid and any particles within it tend to flow in parallel layers without any mixing between them. As a result, exosomes can easily pass through undetected, without ever touching the biosensors on the surface of the chip.
That’s where the herringbone comes in. As reported in Nature Biomedical Engineering, when fluid flows over those 3D herringbone structures, it produces a whirlpool-like effect [2]. As a result, exosomes are more reliably swept into contact with the biosensors.
The team’s distinctive herringbone structures also increase the surface area within the chip. Because the surface is also porous, it allows fluid to drain out slowly to further encourage exosomes to reach the biosensors.
Zeng’s team put their “lab-on-a-chip” to the test using blood samples from 20 patients with ovarian cancer and 10 age-matched controls. The chip was able to detect rapidly the presence of exosomal proteins known to be associated with ovarian cancer.
The researchers report that their device is sensitive enough to detect just 10 exosomes in a 1-microliter sample. It also could be easily adapted to detect exosomal proteins associated with other cancers, and perhaps other conditions as well.
Zeng and colleagues haven’t mentioned whether they’re also looking into trying other geometric patterns in their designs. But the next time you see a tweed jacket, just remember that there’s more to its herringbone pattern than meets the eye.
References:
[1] Ultrasensitive microfluidic analysis of circulating exosomes using a nanostructured graphene oxide/polydopamine coating. Zhang P, He M, Zeng Y. Lab Chip. 2016 Aug 2;16(16):3033-3042.
[2] Ultrasensitive detection of circulating exosomes with a 3D-nanopatterned microfluidic chip. Zhang P, Zhou X, He M, Shang Y, Tetlow AL, Godwin AK, Zeng Y. Nature Biomedical Engineering. February 25, 2019.
Links:
Ovarian, Fallopian Tube, and Primary Peritoneal Cancer—Patient Version (National Cancer Institute/NIH)
Cancer Screening Overview—Patient Version (NCI/NIH)
Extracellular RNA Communication (Common Fund/NIH)
Zeng Lab (University of Kansas, Lawrence)
Godwin Laboratory (University of Kansas Medical Center, Kansas City)
NIH Support: National Cancer Institute
Taking Microfluidics to New Lengths
Posted on by Dr. Francis Collins
Caption: Microfluidic fiber sorting a solution containing either live or dead cells. The type of cell being imaged and the real time voltage (30v) is displayed at bottom. It is easy to imagine how this could be used to sort a mixture of live and dead cells. Credit: Yuan et al., PNAS
Microfluidics—the manipulation of fluids on a microscopic scale— has made it possible to produce “lab-on-a-chip” devices that detect, for instance, the presence of Ebola virus in a single drop of blood. Now, researchers hope to apply the precision of microfluidics to a much broader range of biomedical problems. Their secret? Move the microlab from chips to fibers.
To do this, an NIH-funded team builds microscopic channels into individual synthetic polymer fibers reaching 525 feet, or nearly two football fields long! As shown in this video, the team has already used such fibers to sort live cells from dead ones about 100 times faster than current methods, relying only on natural differences in the cells’ electrical properties. With further design and development, the new, fiber-based systems hold great promise for, among other things, improving kidney dialysis and detecting metastatic cancer cells in a patient’s bloodstream.
Red Blood Cells and Mercury
Posted on by Dr. Francis Collins
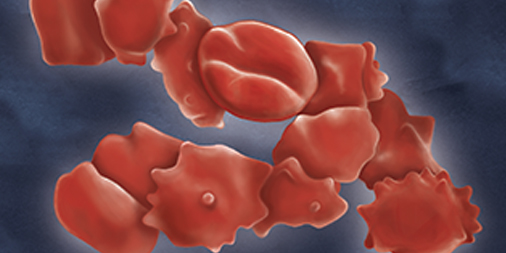
Credit: Courtney Fleming, Birnur Akkaya, and Umut Gurkan, Case Western Reserve University, Cleveland
Mercury is a naturally occurring heavy metal and a well-recognized environmental toxin. When absorbed into the bloodstream at elevated levels, mercury is also extremely harmful to people, causing a range of problems including cognitive impairments, skin rashes, and kidney problems [1].
In this illustration, it’s possible to see in red blood cells the effects of mercury chloride, a toxic chemical compound now sometimes used as a laboratory reagent. Normally, healthy red blood cells have a distinct, doughnut-like shape that helps them squeeze through the tiniest of blood vessels. But these cells are terribly disfigured, with unusual spiky projections, after 24 hours of exposure to low levels of a mercury chloride in solution.
Snapshots of Life: A Flare for the Dramatic
Posted on by Dr. Francis Collins

Credit: Valentin Romanov, University of Utah, Salt Lake City
Oil and water may not mix, but under the right conditions—like those in the photo above—it can sure produce some interesting science that resembles art. You’re looking at a water droplet suspended in an emulsion of olive oil (black and purple) and lipids, molecules that serve as the building blocks of cell membranes. Each lipid has been tagged with a red fluorescent marker, and what look like red and yellow flames are the markers reacting to a beam of UV light. Their glow shows the lipids sticking to the surface of the water droplet, which will soon engulf the droplet to form a single lipid bilayer, which can later be transformed into a lipid bilayer that closely resembles a cell membrane. Scientists use these bubbles, called liposomes, as artificial cells for a variety of research purposes.
In this case, the purpose is structural biology studies. Valentin Romanov, the graduate student at the University of Utah, Salt Lake City, who snapped the image, creates liposomes to study proteins that help cells multiply. By encapsulating and letting the proteins interact with lipids in the artificial cell membrane, Romanov and his colleagues in the NIH-supported labs of Bruce Gale at the University of Utah and Adam Frost at the University of California, San Francisco, can freeze and capture their changing 3D structures at various points in the cell division process with high-resolution imaging techniques. These snapshots will help the researchers to understand in finer detail how the proteins work and perhaps to design drugs to manipulate their functions.
Shining Light on Ebola Virus for Faster Diagnosis
Posted on by Dr. Francis Collins

Caption: A rapid Ebola detection system consisting of a microfluidic chip (left) and an optofluidic chip (right), connected by a curved tube (center).
Credit: Joshua Parks, University of California, Santa Cruz
Many lessons were learned during last year’s devastating outbreak of Ebola virus disease in West Africa. A big one is that field clinics operating in remote settings desperately need a simple, rapid, and accurate test that can tell doctors on the spot—with just a drop of blood—whether or not a person has an active Ebola infection.
A number of point-of-care tests are under development, and it’s exciting to see them moving in the right direction to fill this critical need [1]. As a recent example, a paper published in Nature Scientific Reports by a team of NIH-supported researchers and colleagues shows early success in rapid Ebola detection with an automated lab on a chip [2]. The hybrid system, which combines microfluidics for sample preparation with optofluidics for viral detection, identifies Ebola at concentrations that are typically seen in the bloodstream of an infected person. It also distinguishes between Ebola and the related Marburg and Sudan viruses, suggesting it could be used to detect other infectious diseases.
Snapping Together a New Microlab
Posted on by Dr. Francis Collins
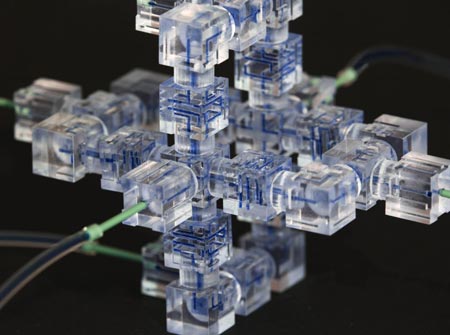
Credit: Viterbi School of Engineering, University of Southern California
Just as the computational power of yesterday’s desktop computer has been miniaturized to fit inside your mobile phone, bioengineers have shrunk traditional laboratory instruments to the size of a dime. To assemble a “snap lab” like the one you see above, all scientists have to do is click together some plastic components in much the same way that kids snap together the plastic bricks in their toy building sets.
The snap lab, developed by an NIH-funded team led by Noah Malmstadt at the University of Southern California (USC) Viterbi School of Engineering, Los Angeles, is an exciting example of a microfluidic circuit—tiny devices designed to test just a single drop of blood, saliva, or other fluids. Such devices have the potential to make DNA analysis, microbe detection, and other biomedical tests easier and cheaper to perform.